

Abstract
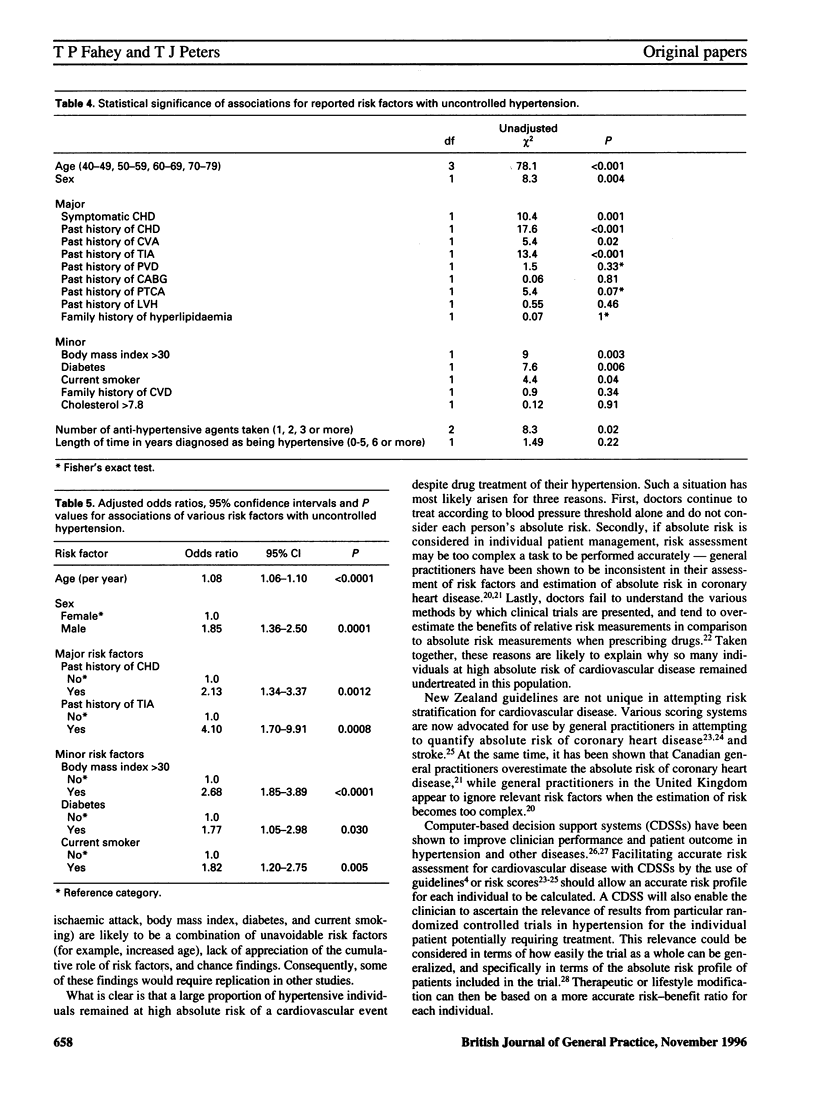
BACKGROUND: When managing hypertension, the assessment of the absolute risk of a cardiovascular' event is now advocated as the most accurate way in which the risks and benefits of anti-hypertensive therapy should be judged. Most studies that have examined control of hypertension have relied solely on the blood pressure level attained after treatment, with no measurement of the likely absolute risk in individual patients. AIM: To assess control of hypertension by quantifying the 10-year absolute risk of cardiovascular disease in patients treated by their general practitioners, and to assess which risk factors are associated with uncontrolled hypertension in this group of patients. METHOD: A cross-sectional study was made of patients on drug treatment for hypertension in 18 Oxfordshire general practices subscribing to the VAMP (value-added medical products) computer system. The absolute risk of suffering a cardiovascular event in the following 10 years was measured according to each individual's risk factor profile. Factors associated with uncontrolled hypertension were ascertained using multiple logistic regression analysis. RESULTS: Overall, 40.9% (37.6% to 44.1%) of the hypertensive population had an absolute risk exceeding 20% of having a cardiovascular event in the following 10 years. The distribution of risk factors varies throughout the population. A higher blood pressure reading was strongly associated with an increased likelihood of high absolute risk, but high blood pressure readings in individual patients did not necessarily equate to a high absolute risk. The factors independently associated with uncontrolled hypertension were age, sex, past history of stroke, ischaemic heart disease and transient ischaemic attack, a body mass index greater than 30, diabetes, and current smoking. CONCLUSIONS: Absolute risk assessment maximizes the risk-benefit ratio in treated hypertensive patients. Individual control and management requires multifactorial assessment and management. Treatment of hypertension according to blood pressure reading alone is not a reliable way of reducing the absolute risk of cardiovascular disease.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alderman M. H. Blood pressure management: individualized treatment based on absolute risk and the potential for benefit. Ann Intern Med. 1993 Aug 15;119(4):329–335. doi: 10.7326/0003-4819-119-4-199308150-00013. [DOI] [PubMed] [Google Scholar]
- Anderson K. M., Wilson P. W., Odell P. M., Kannel W. B. An updated coronary risk profile. A statement for health professionals. Circulation. 1991 Jan;83(1):356–362. doi: 10.1161/01.cir.83.1.356. [DOI] [PubMed] [Google Scholar]
- Bennet N. E. Hypertension in the elderly. Lancet. 1994 Aug 13;344(8920):447–449. doi: 10.1016/s0140-6736(94)91773-6. [DOI] [PubMed] [Google Scholar]
- Coppola W. G., Whincup P. H., Papacosta O., Walker M., Ebrahim S. Scoring system to identify men at high risk of stroke: a strategy for general practice. Br J Gen Pract. 1995 Apr;45(393):185–189. [PMC free article] [PubMed] [Google Scholar]
- Donner A., Birkett N., Buck C. Randomization by cluster. Sample size requirements and analysis. Am J Epidemiol. 1981 Dec;114(6):906–914. doi: 10.1093/oxfordjournals.aje.a113261. [DOI] [PubMed] [Google Scholar]
- Donner A., Klar N. Methods for comparing event rates in intervention studies when the unit of allocation is a cluster. Am J Epidemiol. 1994 Aug 1;140(3):279–301. doi: 10.1093/oxfordjournals.aje.a117247. [DOI] [PubMed] [Google Scholar]
- Evans J. S., Harries C., Dennis I., Dean J. General practitioners' tacit and stated policies in the prescription of lipid lowering agents. Br J Gen Pract. 1995 Jan;45(390):15–18. [PMC free article] [PubMed] [Google Scholar]
- Fahey T., Lancaster T. The detection and management of hypertension in the elderly of Northamptonshire. J Public Health Med. 1995 Mar;17(1):57–62. [PubMed] [Google Scholar]
- Grover S. A., Lowensteyn I., Esrey K. L., Steinert Y., Joseph L., Abrahamowicz M. Do doctors accurately assess coronary risk in their patients? Preliminary results of the coronary health assessment study. BMJ. 1995 Apr 15;310(6985):975–978. doi: 10.1136/bmj.310.6985.975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson R., Barham P., Bills J., Birch T., McLennan L., MacMahon S., Maling T. Management of raised blood pressure in New Zealand: a discussion document. BMJ. 1993 Jul 10;307(6896):107–110. doi: 10.1136/bmj.307.6896.107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson R. Which hypertensive patients should be treated? Lancet. 1994 Feb 26;343(8896):496–497. doi: 10.1016/s0140-6736(94)91456-7. [DOI] [PubMed] [Google Scholar]
- Johnston M. E., Langton K. B., Haynes R. B., Mathieu A. Effects of computer-based clinical decision support systems on clinician performance and patient outcome. A critical appraisal of research. Ann Intern Med. 1994 Jan 15;120(2):135–142. doi: 10.7326/0003-4819-120-2-199401150-00007. [DOI] [PubMed] [Google Scholar]
- McAlister N. H., Covvey H. D., Tong C., Lee A., Wigle E. D. Randomised controlled trial of computer assisted management of hypertension in primary care. Br Med J (Clin Res Ed) 1986 Sep 13;293(6548):670–674. doi: 10.1136/bmj.293.6548.670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mulrow C. D., Cornell J. A., Herrera C. R., Kadri A., Farnett L., Aguilar C. Hypertension in the elderly. Implications and generalizability of randomized trials. JAMA. 1994 Dec 28;272(24):1932–1938. [PubMed] [Google Scholar]
- Ménard J., Chatellier G. Mild hypertension: the mysterious viability of a faulty concept. J Hypertens. 1995 Oct;13(10):1071–1077. doi: 10.1097/00004872-199510000-00001. [DOI] [PubMed] [Google Scholar]
- Sackett D. L., Cook R. J. Understanding clinical trials. BMJ. 1994 Sep 24;309(6957):755–756. doi: 10.1136/bmj.309.6957.755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaper A. G., Pocock S. J., Phillips A. N., Walker M. Identifying men at high risk of heart attacks: strategy for use in general practice. Br Med J (Clin Res Ed) 1986 Aug 23;293(6545):474–479. doi: 10.1136/bmj.293.6545.474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shea S., Misra D., Ehrlich M. H., Field L., Francis C. K. Predisposing factors for severe, uncontrolled hypertension in an inner-city minority population. N Engl J Med. 1992 Sep 10;327(11):776–781. doi: 10.1056/NEJM199209103271107. [DOI] [PubMed] [Google Scholar]
- Silagy C., Mant D., Fowler G., Lodge M. Meta-analysis on efficacy of nicotine replacement therapies in smoking cessation. Lancet. 1994 Jan 15;343(8890):139–142. doi: 10.1016/s0140-6736(94)90933-4. [DOI] [PubMed] [Google Scholar]
- Smith W. C., Lee A. J., Crombie I. K., Tunstall-Pedoe H. Control of blood pressure in Scotland: the rule of halves. BMJ. 1990 Apr 14;300(6730):981–983. doi: 10.1136/bmj.300.6730.981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tunstall-Pedoe H. The Dundee coronary risk-disk for management of change in risk factors. BMJ. 1991 Sep 28;303(6805):744–747. doi: 10.1136/bmj.303.6805.744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whelton P. K., Brancati F. L. Hypertension management in populations. Clin Exp Hypertens. 1993 Nov;15(6):1147–1156. doi: 10.3109/10641969309037101. [DOI] [PubMed] [Google Scholar]
- Whelton P. K. Epidemiology of hypertension. Lancet. 1994 Jul 9;344(8915):101–106. doi: 10.1016/s0140-6736(94)91285-8. [DOI] [PubMed] [Google Scholar]
- Winickoff R. N., Murphy P. K. The persistent problem of poor blood pressure control. Arch Intern Med. 1987 Aug;147(8):1393–1396. [PubMed] [Google Scholar]
- Wolf P. A., D'Agostino R. B., Belanger A. J., Kannel W. B. Probability of stroke: a risk profile from the Framingham Study. Stroke. 1991 Mar;22(3):312–318. doi: 10.1161/01.str.22.3.312. [DOI] [PubMed] [Google Scholar]