

Abstract
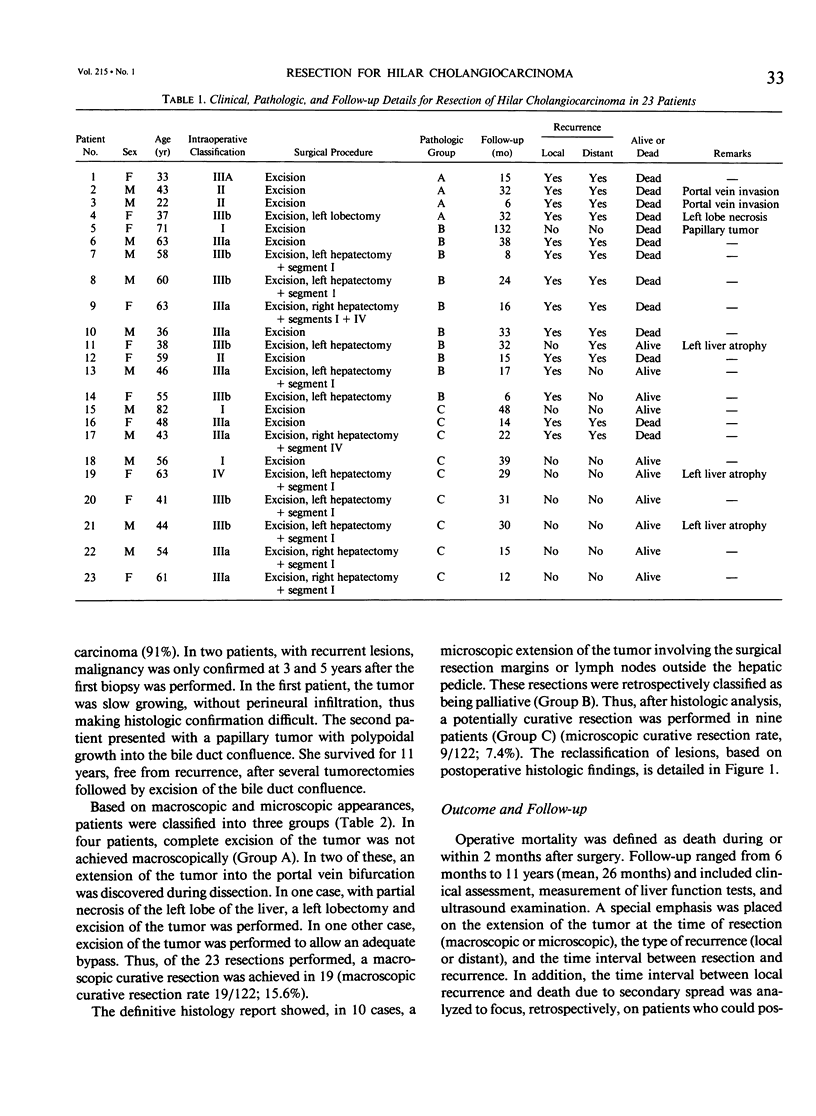
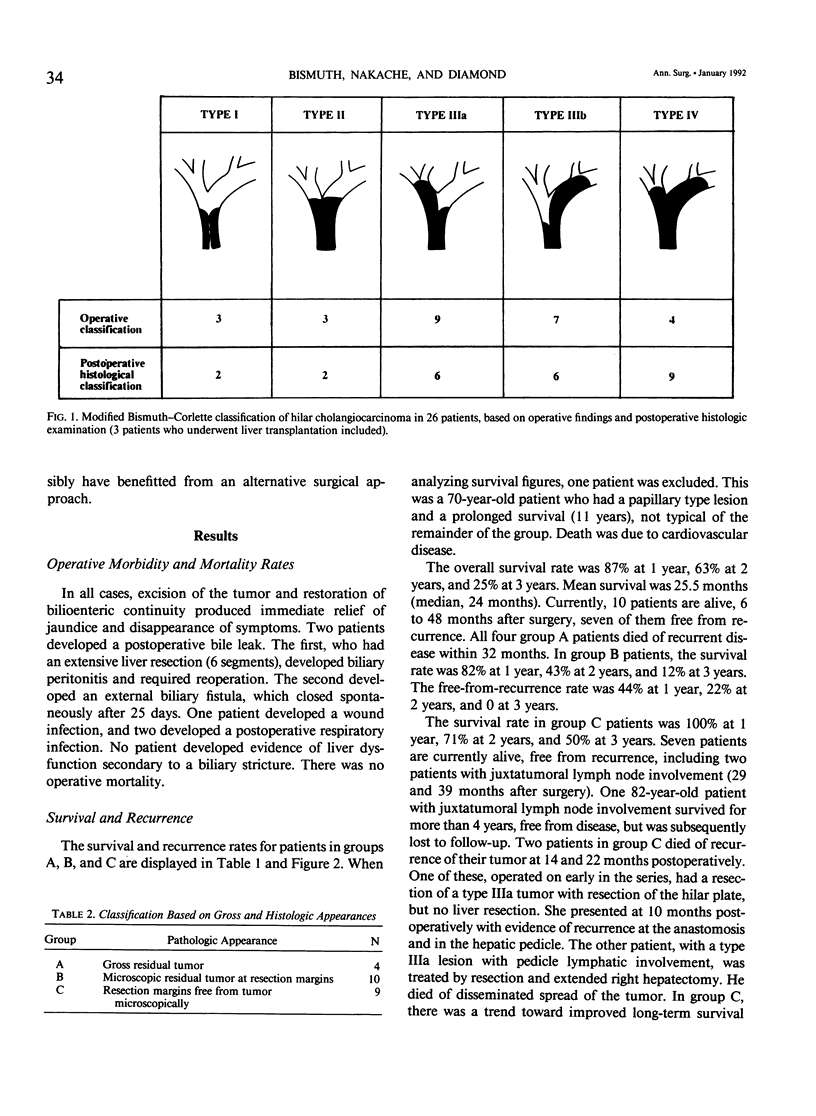
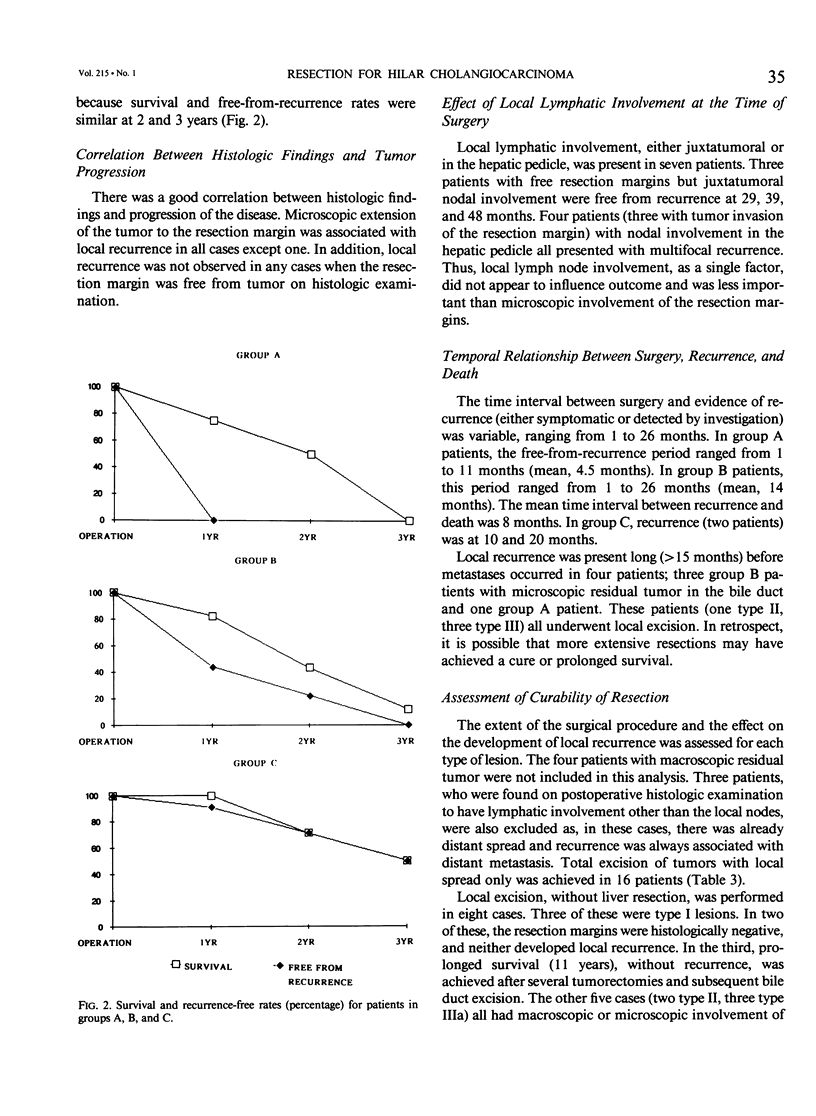
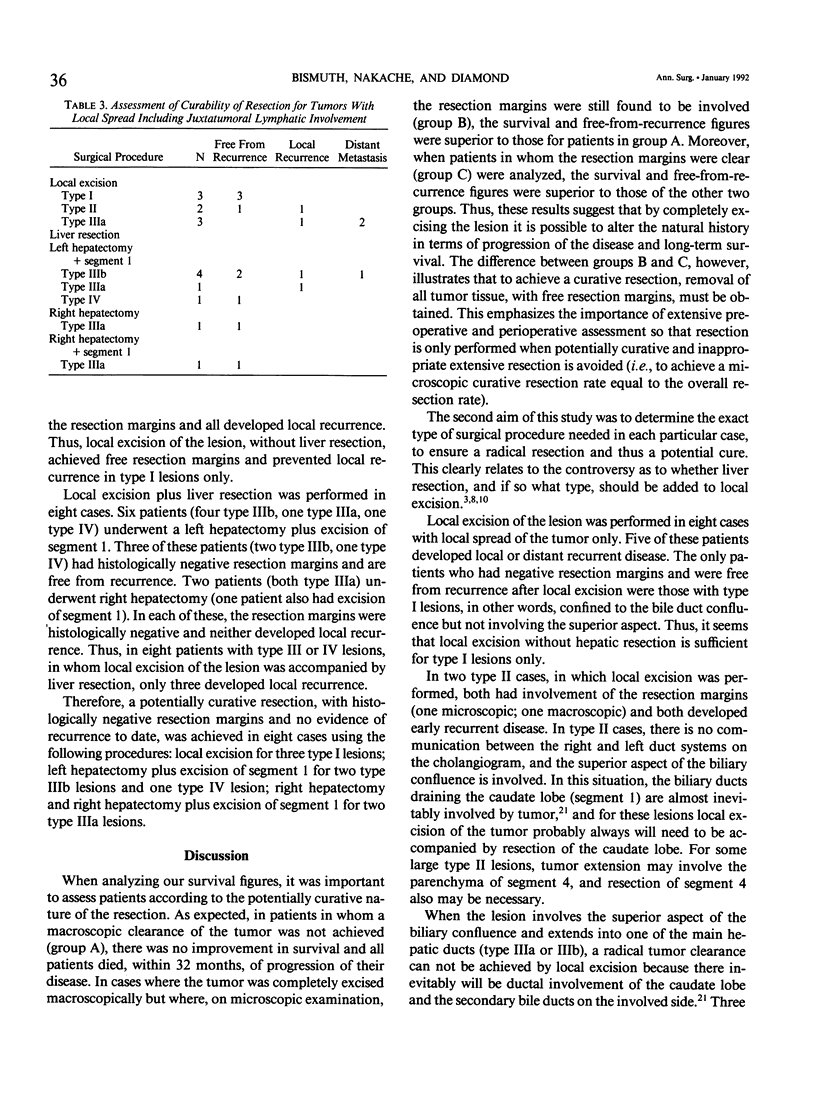
Between 1960 and 1990, resection was performed in 23 of 122 patients who underwent surgical treatment for hilar cholangiocarcinoma. Local excision of the lesion alone was performed in 10 cases (43%). Hepatic resection for tumor extending to the secondary bile ducts or hepatic parenchyma was performed in 13 cases (57%): extended right hepatectomy (3), right hepatectomy (1), extended left hepatectomy (6), left hepatectomy (2), and left lobectectomy (1). In three other cases, resection by total hepatectomy and liver transplantation was performed, but these were not included in the analysis of results for resection. Significant operative complications occurred in only two cases (8.7%), and the operative mortality rate was zero. In four cases, complete excision of the tumor could not be achieved macroscopically (macroscopic curative resection rate 19/122; 15.6%). In nine cases, the margins of the resected specimens were free from tumor on histologic examination (microscopic curative resection rate, 9/122; 7.4%). In 10 cases, the resection margins were found to contain tumor on histologic examination. The overall survival rate was 87% at 1 year, 63% at 2 years, and 25% at 3 years (median survival, 24 months). The survival and freedom from recurrence rates for patients with free resection margins was superior to that for patients with involved resection margins or residual macroscopic disease. A potentially curative resection, with histologically negative margins and no recurrence to date, was achieved in seven patients using the following procedures: local excision for two type I lesions; left hepatectomy plus excision of segment 1 for two type IIIb lesions and one type IV lesion; right hepatectomy and right hepatectomy plus excision of segment 1 for two type IIIa lesions. These results indicate that improved survival in hilar cholangiocarcinoma can be achieved by resection, with minimal morbidity and zero mortality rates, if histologically free resection margins are obtained. To achieve this, we recommend the following procedures for each type of lesion, based on our experience and on anatomic considerations: local excision for type I; local excision plus resection of segment 1 for type II; local excision, resection of segment 1, and right or left hepatectomy for types IIIa and b; hepatectomy plus liver transplantation for type IV.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ALTEMEIER W. A., GALL E. A., ZINNINGER M. M., HOXWORTH P. I. Sclerosing carcinoma of the major intrahepatic bile ducts. AMA Arch Surg. 1957 Sep;75(3):450–461. doi: 10.1001/archsurg.1957.01280150140015. [DOI] [PubMed] [Google Scholar]
- Beazley R. M., Hadjis N., Benjamin I. S., Blumgart L. H. Clinicopathological aspects of high bile duct cancer. Experience with resection and bypass surgical treatments. Ann Surg. 1984 Jun;199(6):623–636. doi: 10.1097/00000658-198406000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bengmark S., Ekberg H., Evander A., Klofver-Stahl B., Tranberg K. G. Major liver resection for hilar cholangiocarcinoma. Ann Surg. 1988 Feb;207(2):120–125. doi: 10.1097/00000658-198802000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bismuth H., Castaing D., Traynor O. Resection or palliation: priority of surgery in the treatment of hilar cancer. World J Surg. 1988 Feb;12(1):39–47. doi: 10.1007/BF01658484. [DOI] [PubMed] [Google Scholar]
- Bismuth H., Corlette M. B. Intrahepatic cholangioenteric anastomosis in carcinoma of the hilus of the liver. Surg Gynecol Obstet. 1975 Feb;140(2):170–178. [PubMed] [Google Scholar]
- Blumgart L. H., Hadjis N. S., Benjamin I. S., Beazley R. Surgical approaches to cholangiocarcinoma at confluence of hepatic ducts. Lancet. 1984 Jan 14;1(8368):66–70. doi: 10.1016/s0140-6736(84)90002-3. [DOI] [PubMed] [Google Scholar]
- Calne R. Y. Liver transplantation for liver cancer. World J Surg. 1982 Jan;6(1):76–80. doi: 10.1007/BF01656376. [DOI] [PubMed] [Google Scholar]
- Cameron J. L., Pitt H. A., Zinner M. J., Kaufman S. L., Coleman J. Management of proximal cholangiocarcinomas by surgical resection and radiotherapy. Am J Surg. 1990 Jan;159(1):91–98. doi: 10.1016/s0002-9610(05)80612-9. [DOI] [PubMed] [Google Scholar]
- Evander A., Fredlund P., Hoevels J., Ihse I., Bengmark S. Evaluation of aggressive surgery for carcinoma of the extrahepatic bile ducts. Ann Surg. 1980 Jan;191(1):23–29. doi: 10.1097/00000658-198001000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fletcher M. S., Brinkley D., Dawson J. L., Nunnerley H., Wheeler P. G., Williams R. Treatment of high bileduct carcinoma by internal radiotherapy with iridium-192 wire. Lancet. 1981 Jul 25;2(8239):172–174. doi: 10.1016/s0140-6736(81)90357-3. [DOI] [PubMed] [Google Scholar]
- Hatfield A. R., Tobias R., Terblanche J., Girdwood A. H., Fataar S., Harries-Jones R., Kernoff L., Marks I. N. Preoperative external biliary drainage in obstructive jaundice. A prospective controlled clinical trial. Lancet. 1982 Oct 23;2(8304):896–899. doi: 10.1016/s0140-6736(82)90866-2. [DOI] [PubMed] [Google Scholar]
- KLATSKIN G. ADENOCARCINOMA OF THE HEPATIC DUCT AT ITS BIFURCATION WITHIN THE PORTA HEPATIS. AN UNUSUAL TUMOR WITH DISTINCTIVE CLINICAL AND PATHOLOGICAL FEATURES. Am J Med. 1965 Feb;38:241–256. doi: 10.1016/0002-9343(65)90178-6. [DOI] [PubMed] [Google Scholar]
- Lai E. C., Tompkins R. K., Mann L. L., Roslyn J. J. Proximal bile duct cancer. Quality of survival. Ann Surg. 1987 Feb;205(2):111–118. doi: 10.1097/00000658-198702000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Launois B., Campion J. P., Brissot P., Gosselin M. Carcinoma of the hepatic hilus. Surgical management and the case for resection. Ann Surg. 1979 Aug;190(2):151–157. doi: 10.1097/00000658-197908000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nimura Y., Hayakawa N., Kamiya J., Kondo S., Shionoya S. Hepatic segmentectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg. 1990 Jul-Aug;14(4):535–544. doi: 10.1007/BF01658686. [DOI] [PubMed] [Google Scholar]
- Pichlmayr R., Ringe B., Lauchart W., Bechstein W. O., Gubernatis G., Wagner E. Radical resection and liver grafting as the two main components of surgical strategy in the treatment of proximal bile duct cancer. World J Surg. 1988 Feb;12(1):68–77. doi: 10.1007/BF01658489. [DOI] [PubMed] [Google Scholar]
- Pinson C. W., Rossi R. L. Extended right hepatic lobectomy, left hepatic lobectomy, and skeletonization resection for proximal bile duct cancer. World J Surg. 1988 Feb;12(1):52–59. doi: 10.1007/BF01658486. [DOI] [PubMed] [Google Scholar]
- Pitt H. A., Gomes A. S., Lois J. F., Mann L. L., Deutsch L. S., Longmire W. P., Jr Does preoperative percutaneous biliary drainage reduce operative risk or increase hospital cost? Ann Surg. 1985 May;201(5):545–553. doi: 10.1097/00000658-198505000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reding R., Buard J. L., Lebeau G., Launois B. Surgical management of 552 carcinomas of the extrahepatic bile ducts (gallbladder and periampullary tumors excluded). Results of the French Surgical Association Survey. Ann Surg. 1991 Mar;213(3):236–241. doi: 10.1097/00000658-199103000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suzuki M., Takahashi T., Ouchi K., Matsuno S. The development and extension of hepatohilar bile duct carcinoma. A three-dimensional tumor mapping in the intrahepatic biliary tree visualized with the aid of a graphics computer system. Cancer. 1989 Aug 1;64(3):658–666. doi: 10.1002/1097-0142(19890801)64:3<658::aid-cncr2820640316>3.0.co;2-6. [DOI] [PubMed] [Google Scholar]
- Terblanche J., Saunders S. J., Louw J. H. Prolonged palliation in carcinoma of the man hepatic duct junction. Surgery. 1972 May;71(5):720–731. [PubMed] [Google Scholar]
- Weinbren K., Mutum S. S. Pathological aspects of cholangiocarcinoma. J Pathol. 1983 Feb;139(2):217–238. doi: 10.1002/path.1711390210. [DOI] [PubMed] [Google Scholar]
- Wheeler P. G., Dawson J. L., Nunnerley H., Brinkley D., Laws J., Williams R. Newer techniques in the diagnosis and treatment of proximal bile duct carcinoma--an analysis of 41 consecutive patients. Q J Med. 1981 Summer;50(199):247–258. [PubMed] [Google Scholar]
- Whelton M. J., Petrelli M., George P., Young W. B., Sherlock S. Carcinoma at the junction of the main hepatic ducts. Q J Med. 1969 Apr;38(150):211–230. [PubMed] [Google Scholar]