

Abstract
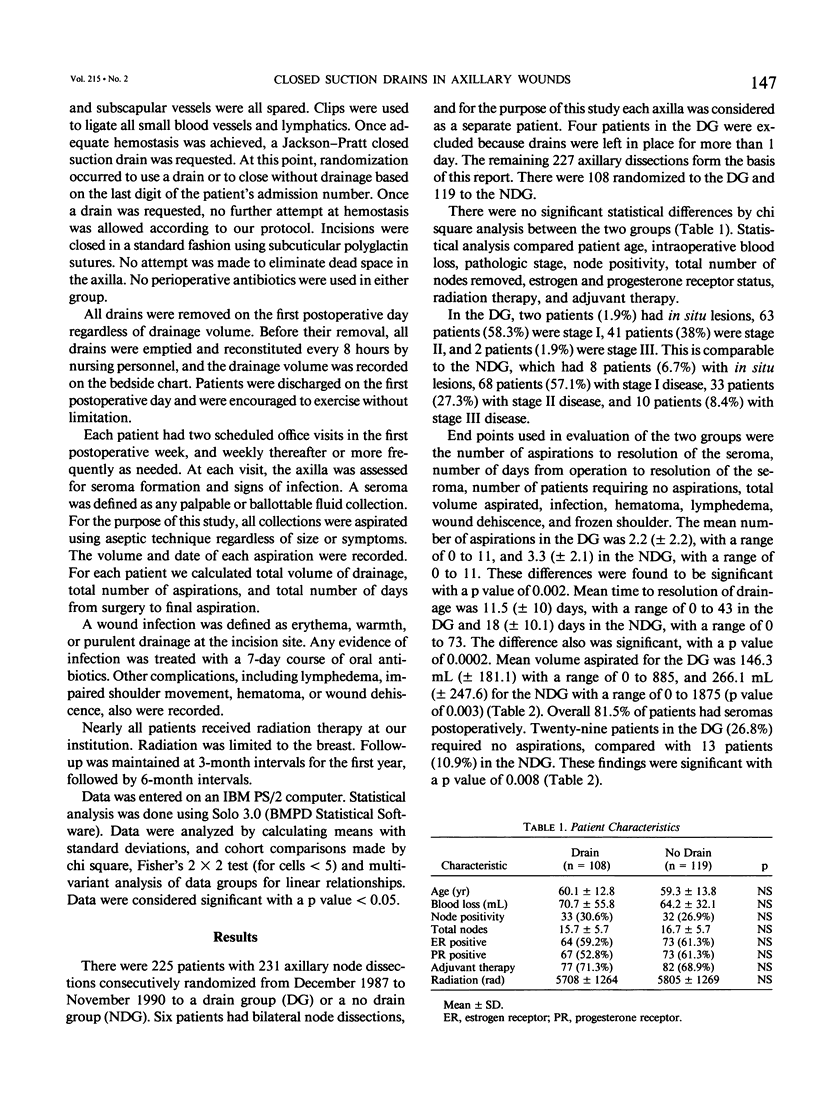
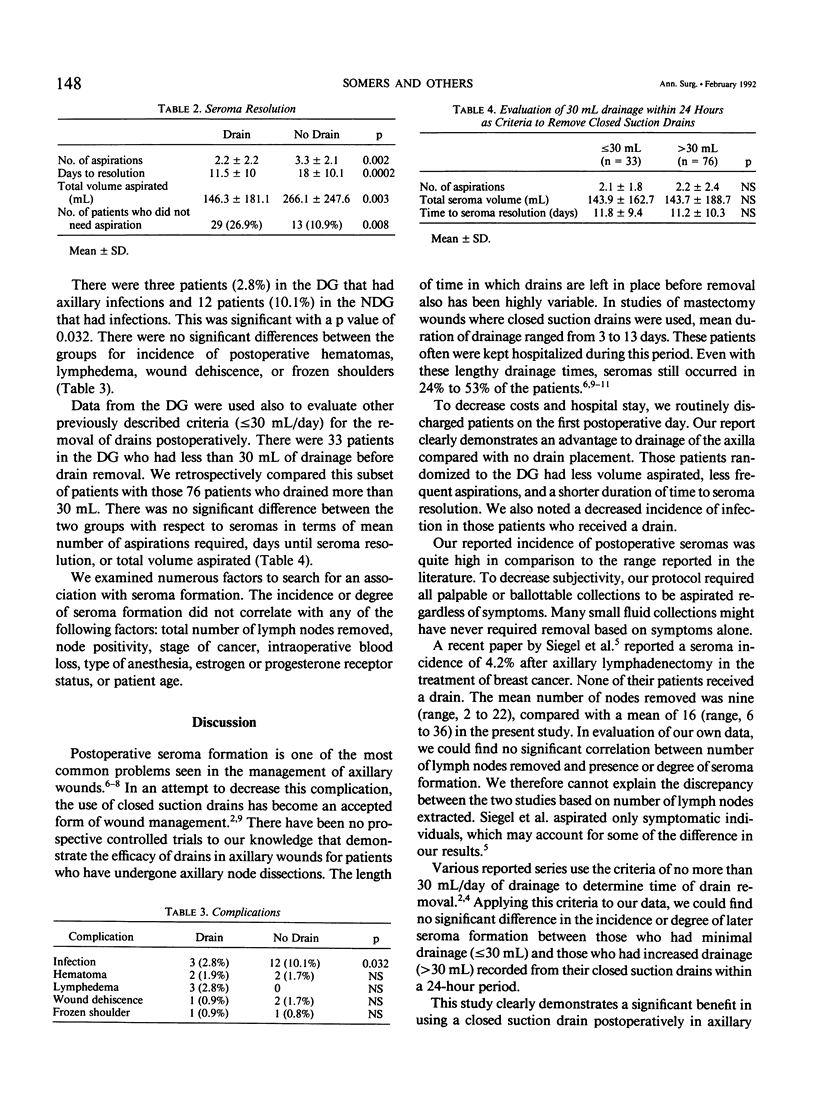
Closed suction drainage has been used to prevent seroma formation after lumpectomy and axillary node dissection for breast cancer. To study the efficacy of closed suction drains, the authors conducted a prospective randomized study from 1987 to 1990 of 227 axillary dissections. One hundred eight were randomized to a drain group (DG) and 119 to a no drain group (NDG). Drains were removed on the first postoperative day just before patient discharge. Postoperatively, all palpable axillary collections were aspirated on each follow-up visit. The volume aspirated, the number of aspirations, the time to seroma resolution, and all complications were recorded. The mean number of aspirations in the DG was significantly lower than the NDG (2.2 +/- 2.2 versus 3.3 +/- 2.1; p less than or equal to 0.002). Mean volume aspirated in the DG (146.3 +/- 181.1 mL) was less than the NDG (266.1 +/- 247.6 mL; p less than or equal to 0.003), and the time to seroma resolution was decreased in the DG as compared with the NDG (11.5 +/- 10 days versus 18 +/- 10.1 days; p less than or equal to 0.0002). Closed suction drainage after lumpectomy and axillary node dissection is advantageous in decreasing the incidence and degree of seroma formation and need not delay early hospital discharge.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aitken D. R., Hunsaker R., James A. G. Prevention of seromas following mastectomy and axillary dissection. Surg Gynecol Obstet. 1984 Apr;158(4):327–330. [PubMed] [Google Scholar]
- Cohen A. M., Schaeffer N., Chen Z. Y., Wood W. C. Early discharge after modified radical mastectomy. Am J Surg. 1986 Apr;151(4):465–466. doi: 10.1016/0002-9610(86)90104-2. [DOI] [PubMed] [Google Scholar]
- Fisher B., Redmond C., Poisson R., Margolese R., Wolmark N., Wickerham L., Fisher E., Deutsch M., Caplan R., Pilch Y. Eight-year results of a randomized clinical trial comparing total mastectomy and lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med. 1989 Mar 30;320(13):822–828. doi: 10.1056/NEJM198903303201302. [DOI] [PubMed] [Google Scholar]
- Harris M. N., Gumport S. L., Maiwandi H. Axillary lymph node dissection for melanoma. Surg Gynecol Obstet. 1972 Dec;135(6):936–940. [PubMed] [Google Scholar]
- Jansen R. F., van Geel A. N., de Groot H. G., Rottier A. B., Olthuis G. A., van Putten W. L. Immediate versus delayed shoulder exercises after axillary lymph node dissection. Am J Surg. 1990 Nov;160(5):481–484. doi: 10.1016/s0002-9610(05)81008-6. [DOI] [PubMed] [Google Scholar]
- Morris A. M. A controlled trial of closed wound suction. Br J Surg. 1973 May;60(5):357–359. doi: 10.1002/bjs.1800600509. [DOI] [PubMed] [Google Scholar]
- Moss J. P. Historical and current perspectives on surgical drainage. Surg Gynecol Obstet. 1981 Apr;152(4):517–527. [PubMed] [Google Scholar]
- Orr R. K., Ketcham A. S., Robinson D. S., Moffat F. L., Tennant N. D. Early discharge after mastectomy. A safe way of diminishing hospital costs. Am Surg. 1987 Mar;53(3):161–163. [PubMed] [Google Scholar]
- Say C. C., Donegan W. A biostatistical evaluation of complications from mastectomy. Surg Gynecol Obstet. 1974 Mar;138(3):370–376. [PubMed] [Google Scholar]
- Siegel B. M., Mayzel K. A., Love S. M. Level I and II axillary dissection in the treatment of early-stage breast cancer. An analysis of 259 consecutive patients. Arch Surg. 1990 Sep;125(9):1144–1147. doi: 10.1001/archsurg.1990.01410210070010. [DOI] [PubMed] [Google Scholar]