

Abstract
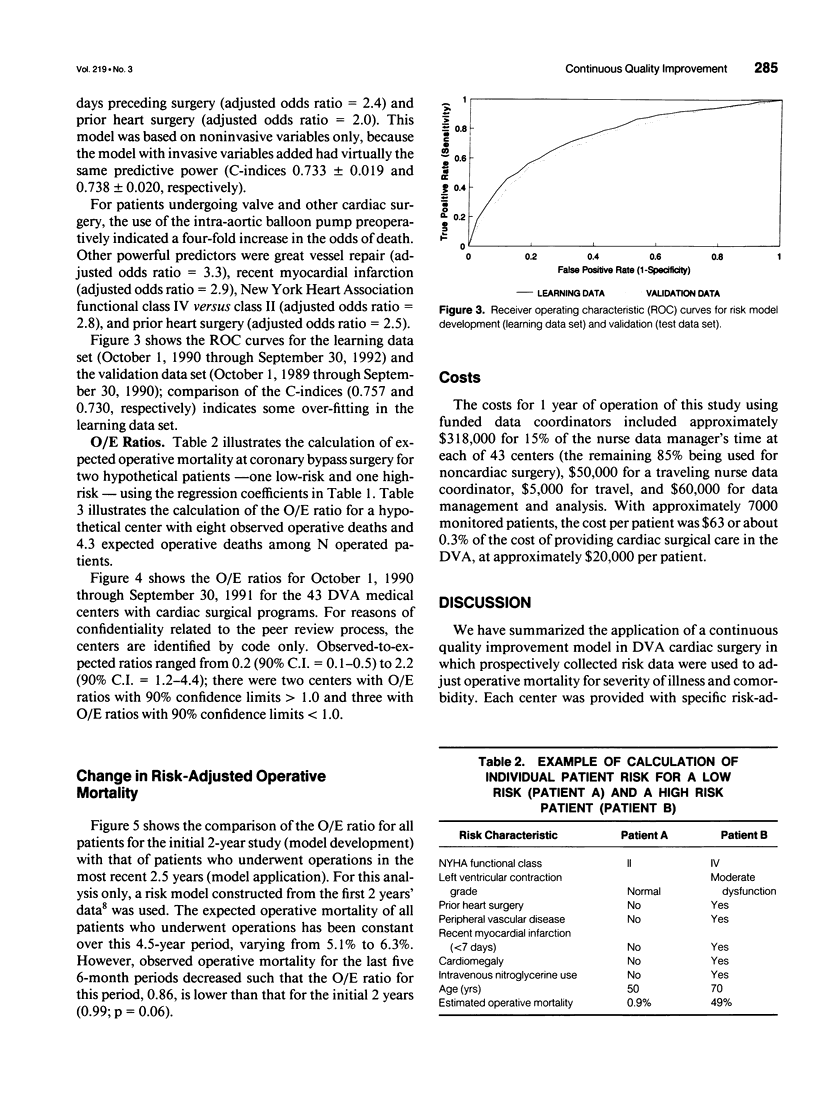
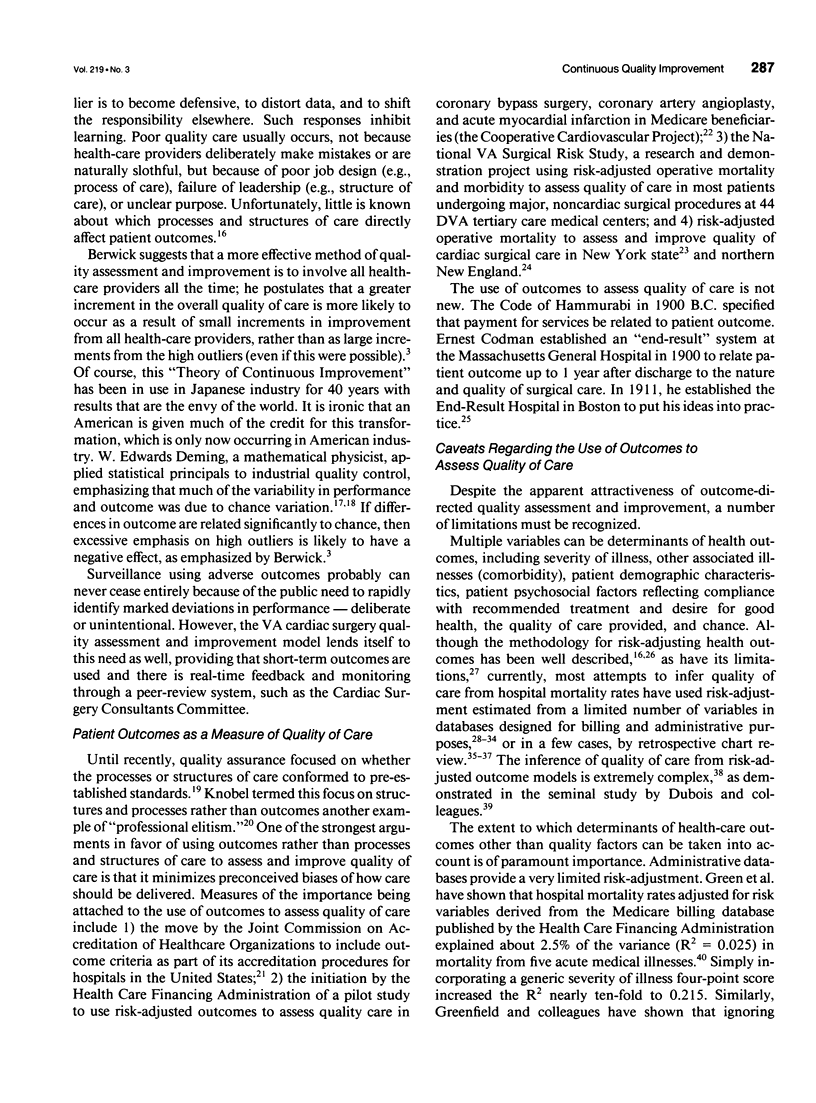
OBJECTIVE: The authors organized the Department of Veterans Affairs (VA) Continuous Improvement in Cardiac Surgery Study (CICSS) to provide risk-adjusted outcome data for the continuous assessment and improvement of quality of care for all patients undergoing cardiac surgery in the VA. BACKGROUND: The use of risk-adjusted outcomes to monitor quality of health care has the potential advantage over consensus-derived standards of being free of preconceived biases about how health care should be provided. Monitoring outcomes of all health care episodes, as opposed to review of selected cases (e.g., adverse outcomes), has the advantages of greater statistical power, the opportunity to compare processes of care between good and bad outcomes, and the positive psychology of treating all providers equally. These two concepts, together with a pre-existing peer committee (the VA Cardiac Surgery Consultants Committee) to review, interpret, and act on the risk-adjusted outcome data, form the primary design considerations for CICSS. METHODS: Patient-level risk and outcome (operative mortality and morbidity) data are collected prospectively on each of the approximately 7000 patients undergoing cardiac surgery in the VA each year. These outcomes, adjusted for patient risk using logistic regression, are provided every 6 months to each cardiac surgery program and to a national peer review committee for internal and external quality assessment and improvement. RESULTS: For the most recent 12-month period with complete data collection, observed-to-expected (O/E) ratios ranged from 0.2 to 2.2, with eight centers falling outside of the 90% confidence limits for an O/E ratio equaling 1.0. The O/E ratio for all centers has fallen by 14% over the 4.5-year period of this program (p = 0.06). CONCLUSIONS: A large-scale, low-cost program of continuous quality improvement using risk-adjusted outcome is feasible. This program has been associated with a decrease in risk-adjusted operative mortality.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Berwick D. M. Continuous improvement as an ideal in health care. N Engl J Med. 1989 Jan 5;320(1):53–56. doi: 10.1056/NEJM198901053200110. [DOI] [PubMed] [Google Scholar]
- Berwick D. M. Toward an applied technology for quality measurement in health care. Med Decis Making. 1988 Oct-Dec;8(4):253–258. doi: 10.1177/0272989X8800800405. [DOI] [PubMed] [Google Scholar]
- Blumberg M. S. Comments on HCFA hospital death rate statistical outliers. Health Care Financing Administration. Health Serv Res. 1987 Feb;21(6):715–739. [PMC free article] [PubMed] [Google Scholar]
- Blumberg M. S. Measuring surgical quality in Maryland: a model. Health Aff (Millwood) 1988 Spring;7(1):62–78. doi: 10.1377/hlthaff.7.1.62. [DOI] [PubMed] [Google Scholar]
- Blumberg M. S. Risk adjusting health care outcomes: a methodologic review. Med Care Rev. 1986 Fall;43(2):351–393. doi: 10.1177/107755878604300205. [DOI] [PubMed] [Google Scholar]
- Copeland G. P., Jones D., Walters M. POSSUM: a scoring system for surgical audit. Br J Surg. 1991 Mar;78(3):355–360. doi: 10.1002/bjs.1800780327. [DOI] [PubMed] [Google Scholar]
- Daley J., Jencks S., Draper D., Lenhart G., Thomas N., Walker J. Predicting hospital-associated mortality for Medicare patients. A method for patients with stroke, pneumonia, acute myocardial infarction, and congestive heart failure. JAMA. 1988 Dec 23;260(24):3617–3624. doi: 10.1001/jama.260.24.3617. [DOI] [PubMed] [Google Scholar]
- Diamond G. A. Future imperfect: the limitations of clinical prediction models and the limits of clinical prediction. J Am Coll Cardiol. 1989 Sep;14(3 Suppl A):12A–22A. doi: 10.1016/0735-1097(89)90157-5. [DOI] [PubMed] [Google Scholar]
- Donabedian A. Quality assessment and assurance: unity of purpose, diversity of means. Inquiry. 1988 Spring;25(1):173–192. [PubMed] [Google Scholar]
- Dubois R. W., Brook R. H., Rogers W. H. Adjusted hospital death rates: a potential screen for quality of medical care. Am J Public Health. 1987 Sep;77(9):1162–1166. doi: 10.2105/ajph.77.9.1162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dubois R. W., Rogers W. H., Moxley J. H., 3rd, Draper D., Brook R. H. Hospital inpatient mortality. Is it a predictor of quality? N Engl J Med. 1987 Dec 24;317(26):1674–1680. doi: 10.1056/NEJM198712243172626. [DOI] [PubMed] [Google Scholar]
- Duckett S. J., Kristofferson S. M. An index of hospital performance. Med Care. 1978 May;16(5):400–407. doi: 10.1097/00005650-197805000-00004. [DOI] [PubMed] [Google Scholar]
- Edwards F. H., Albus R. A., Zajtchuk R., Graeber G. M., Barry M. J., Rumisek J. D., Arishita G. Use of a Bayesian statistical model for risk assessment in coronary artery surgery. Ann Thorac Surg. 1988 Apr;45(4):437–440. doi: 10.1016/s0003-4975(98)90020-0. [DOI] [PubMed] [Google Scholar]
- Ellwood P. M. Shattuck lecture--outcomes management. A technology of patient experience. N Engl J Med. 1988 Jun 9;318(23):1549–1556. doi: 10.1056/NEJM198806093182327. [DOI] [PubMed] [Google Scholar]
- Goss M. E., Reed J. I. Evaluating the quality of hospital care through severity-adjusted death rates: some pitfalls. Med Care. 1974 Mar;12(3):202–213. doi: 10.1097/00005650-197403000-00002. [DOI] [PubMed] [Google Scholar]
- Green J., Wintfeld N., Sharkey P., Passman L. J. The importance of severity of illness in assessing hospital mortality. JAMA. 1990 Jan 12;263(2):241–246. [PubMed] [Google Scholar]
- Greenfield S., Aronow H. U., Elashoff R. M., Watanabe D. Flaws in mortality data. The hazards of ignoring comorbid disease. JAMA. 1988 Oct 21;260(15):2253–2255. [PubMed] [Google Scholar]
- Grover F. L., Hammermeister K. E., Burchfiel C. Initial report of the Veterans Administration Preoperative Risk Assessment Study for Cardiac Surgery. Ann Thorac Surg. 1990 Jul;50(1):12–28. doi: 10.1016/0003-4975(90)90073-f. [DOI] [PubMed] [Google Scholar]
- Hanley J. A., McNeil B. J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982 Apr;143(1):29–36. doi: 10.1148/radiology.143.1.7063747. [DOI] [PubMed] [Google Scholar]
- Hannan E. L., Kilburn H., Jr, O'Donnell J. F., Lukacik G., Shields E. P. Adult open heart surgery in New York State. An analysis of risk factors and hospital mortality rates. JAMA. 1990 Dec 5;264(21):2768–2774. [PubMed] [Google Scholar]
- Harrell F. E., Jr, Lee K. L., Califf R. M., Pryor D. B., Rosati R. A. Regression modelling strategies for improved prognostic prediction. Stat Med. 1984 Apr-Jun;3(2):143–152. doi: 10.1002/sim.4780030207. [DOI] [PubMed] [Google Scholar]
- Hebel J. R., Kessler I. I., Mabuchi K., McCarter R. J. Assessment of hospital performance by use of death rates. A recent case history. JAMA. 1982 Dec 17;248(23):3131–3135. [PubMed] [Google Scholar]
- Horn S. D., Horn R. A. The Computerized Severity Index. A new tool for case-mix management. J Med Syst. 1986 Feb;10(1):73–78. doi: 10.1007/BF00992953. [DOI] [PubMed] [Google Scholar]
- Jencks S. F., Daley J., Draper D., Thomas N., Lenhart G., Walker J. Interpreting hospital mortality data. The role of clinical risk adjustment. JAMA. 1988 Dec 23;260(24):3611–3616. [PubMed] [Google Scholar]
- Jencks S. F., Wilensky G. R. The health care quality improvement initiative. A new approach to quality assurance in Medicare. JAMA. 1992 Aug 19;268(7):900–903. [PubMed] [Google Scholar]
- Kahn K. L., Brook R. H., Draper D., Keeler E. B., Rubenstein L. V., Rogers W. H., Kosecoff J. Interpreting hospital mortality data. How can we proceed? JAMA. 1988 Dec 23;260(24):3625–3628. [PubMed] [Google Scholar]
- Kennedy J. W., Kaiser G. C., Fisher L. D., Maynard C., Fritz J. K., Myers W., Mudd J. G., Ryan T. J., Coggin J. Multivariate discriminant analysis of the clinical and angiographic predictors of operative mortality from the Collaborative Study in Coronary Artery Surgery (CASS). J Thorac Cardiovasc Surg. 1980 Dec;80(6):876–887. [PubMed] [Google Scholar]
- Kouchoukos N. T., Ebert P. A., Grover F. L., Lindesmith G. G. Report of the Ad Hoc Committee on Risk Factors for Coronary Artery Bypass Surgery. Ann Thorac Surg. 1988 Mar;45(3):348–349. doi: 10.1016/s0003-4975(10)62482-4. [DOI] [PubMed] [Google Scholar]
- Lohr K. N. Outcome measurement: concepts and questions. Inquiry. 1988 Spring;25(1):37–50. [PubMed] [Google Scholar]
- Lohr K. N., Schroeder S. A. A strategy for quality assurance in Medicare. N Engl J Med. 1990 Mar 8;322(10):707–712. doi: 10.1056/nejm199003083221031. [DOI] [PubMed] [Google Scholar]
- Mosteller F. Assessing quality of institutional care. Am J Public Health. 1987 Sep;77(9):1155–1156. doi: 10.2105/ajph.77.9.1155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Narain P., Rubenstein L. Z., Wieland G. D., Rosbrook B., Strome L. S., Pietruszka F., Morley J. E. Predictors of immediate and 6-month outcomes in hospitalized elderly patients. The importance of functional status. J Am Geriatr Soc. 1988 Sep;36(9):775–783. doi: 10.1111/j.1532-5415.1988.tb04259.x. [DOI] [PubMed] [Google Scholar]
- Neuhauser D. Ernest Amory Codman, M.D., and end results of medical care. Int J Technol Assess Health Care. 1990;6(2):307–325. doi: 10.1017/s0266462300000842. [DOI] [PubMed] [Google Scholar]
- Neuhauser D. The quality of medical care and the 14 points of Edward Deming. Health Matrix. 1988 Summer;6(2):7–10. [PubMed] [Google Scholar]
- O'Connor G. T., Plume S. K., Olmstead E. M., Coffin L. H., Morton J. R., Maloney C. T., Nowicki E. R., Tryzelaar J. F., Hernandez F., Adrian L. A regional prospective study of in-hospital mortality associated with coronary artery bypass grafting. The Northern New England Cardiovascular Disease Study Group. JAMA. 1991 Aug 14;266(6):803–809. [PubMed] [Google Scholar]
- O'Leary D. S. The Joint Commission looks to the future. JAMA. 1987 Aug 21;258(7):951–952. [PubMed] [Google Scholar]
- Roemer M. I., Moustafa A. T., Hopkins C. E. A proposed hospital quality index: hospital death rates adjusted for case severity. Health Serv Res. 1968 Summer;3(2):96–118. [PMC free article] [PubMed] [Google Scholar]
- Ruberman W., Weinblatt E., Goldberg J. D., Chaudhary B. S. Psychosocial influences on mortality after myocardial infarction. N Engl J Med. 1984 Aug 30;311(9):552–559. doi: 10.1056/NEJM198408303110902. [DOI] [PubMed] [Google Scholar]
- Sethi G. K., Miller D. C., Souchek J., Oprian C., Henderson W. G., Hassan Z., Folland E., Khuri S., Scott S. M., Burchfiel C. Clinical, hemodynamic, and angiographic predictors of operative mortality in patients undergoing single valve replacement. Veterans Administration Cooperative Study on Valvular Heart Disease. J Thorac Cardiovasc Surg. 1987 Jun;93(6):884–897. [PubMed] [Google Scholar]
- Takaro T., Ankeney J. L., Laning R. C., Peduzzi P. N. Quality control for cardiac surgery in the Veterans Administration. Ann Thorac Surg. 1986 Jul;42(1):37–44. doi: 10.1016/s0003-4975(10)61833-4. [DOI] [PubMed] [Google Scholar]
- Wyszewianski L. Quality of care: past achievements and future challenges. Inquiry. 1988 Spring;25(1):13–22. [PubMed] [Google Scholar]