

Abstract
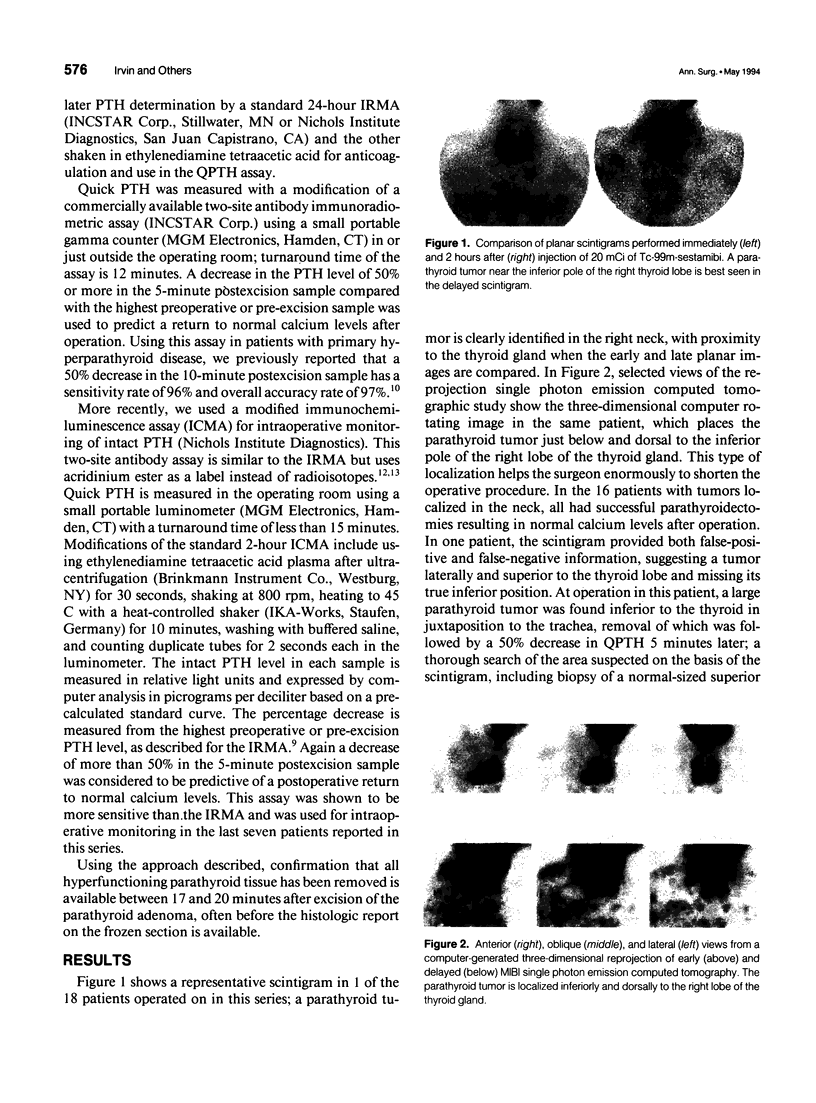
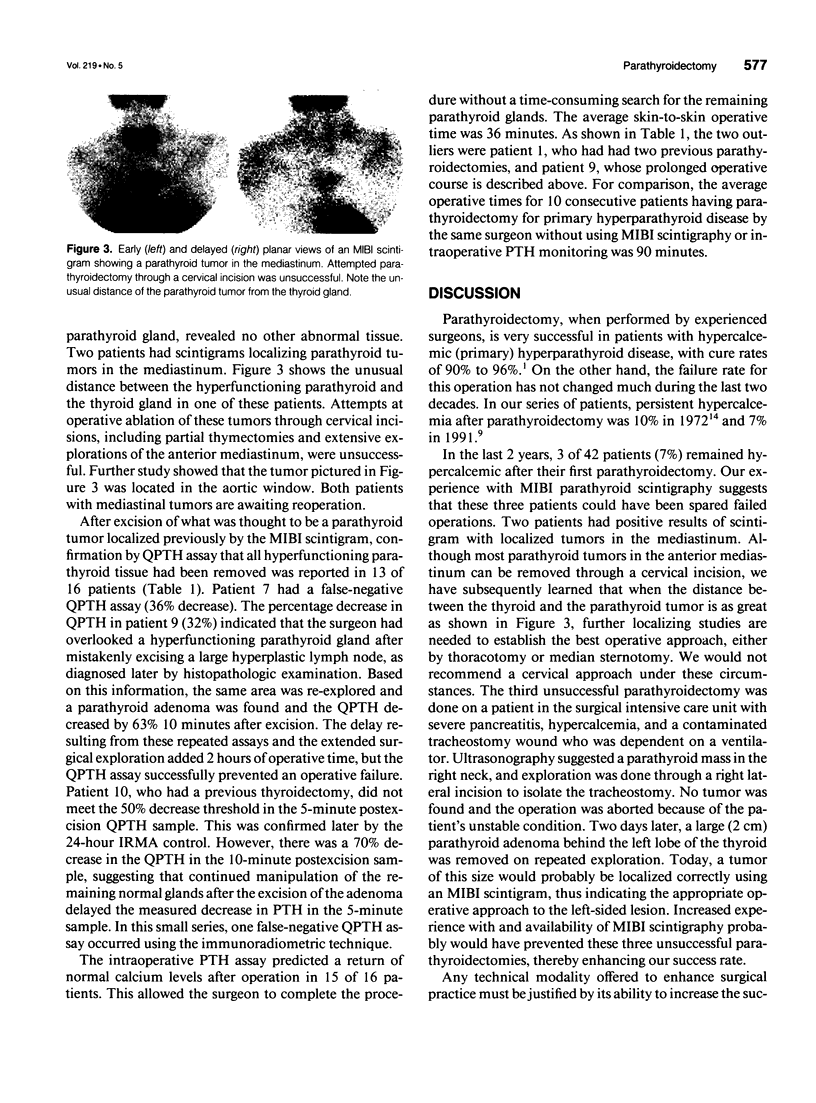
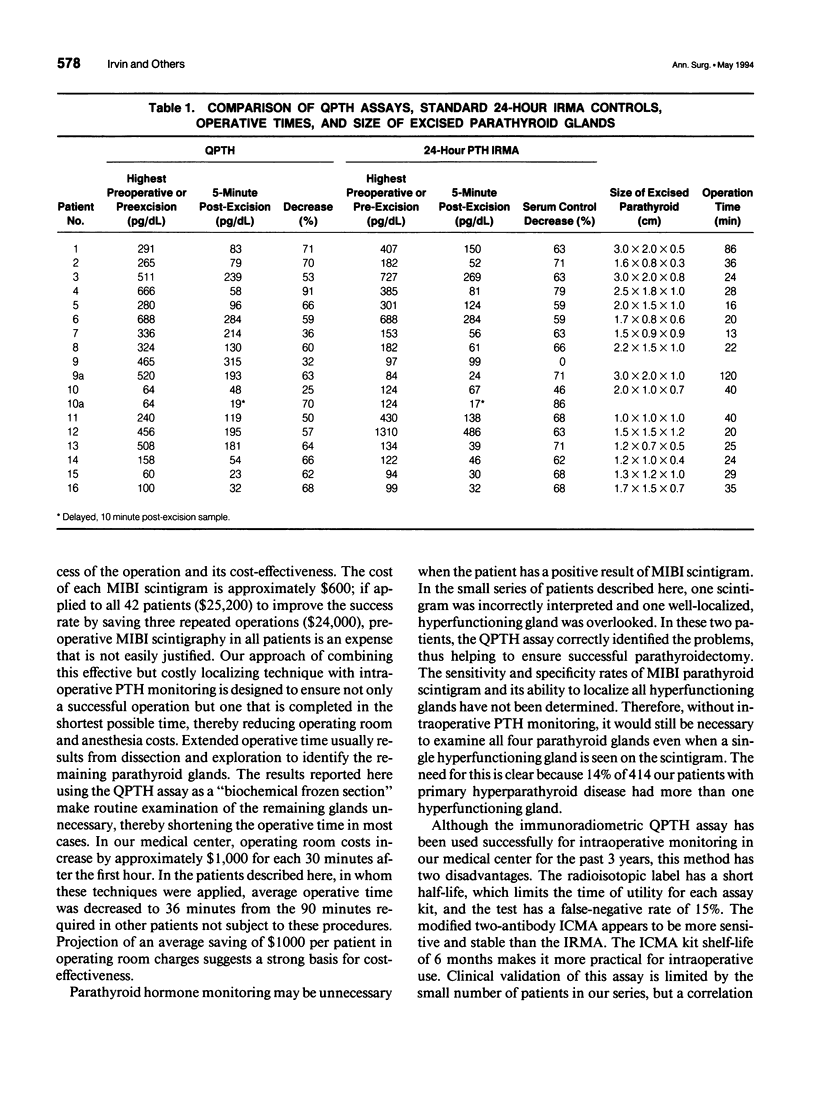
OBJECTIVE: To decrease the operative time for parathyroidectomy in patients with hypercalcemic (primary) hyperparathyroid disease, a combination of preoperative localization of a parathyroid tumor with an effective nuclear scan (scintigram) and intraoperative monitoring of parathyroid hormone (quick parathyroid hormone measurement) to ensure excision of all hyperfunctioning tissue was studied. SUMMARY BACKGROUND DATA: For many years, persistent hypercalcemia after parathyroidectomy (3% to 10%) has been constant and is usually due to the surgeon's failure to remove all hyperfunctioning glands. A marked decrease in parathormone level after excision of a single large gland predicts operative success and a return to normal calcium levels. Conversely, persistent high levels of parathyroid hormone indicate excess secretion by another gland(s) and the need for further exploration. Recently Tc-99m-sestamibi (MIBI) scintigraphy was shown to be more effective in localizing parathyroid tumors than previous methods. A combination of both techniques could be useful to the surgeon if they improve the operative success rate and are cost-effective. METHODS: Parathyroidectomy was performed on 18 patients with primary hyperparathyroid disease, with tumors localized by MIBI scintigrams. When excision of the identified parathyroid gland was accomplished, the operation was terminated and quick parathyroid hormone was measured to confirm that all hyperfunctioning tissue was removed. RESULTS: Sixteen patients with positive results of scintigram had successful parathyroidectomies confirmed by quick parathyroid hormone measurement with a cervical approach. Two patients with mediastinal tumors localized by MIBI scintigraphy could not be resected using this approach. One false-positive/false-negative scintigram was obtained. Compared with patients having parathyroidectomy without localization and hormone monitoring, the average operative time was shortened from 90 to 36 minutes. CONCLUSIONS: Localization and successful excision of parathyroid tumors with confirmation that no other hyperfunctioning glands were present by quick parathyroid hormone monitoring can predict a return to normal calcium levels and a decrease in operative time in parathyroidectomy.
Full text
PDF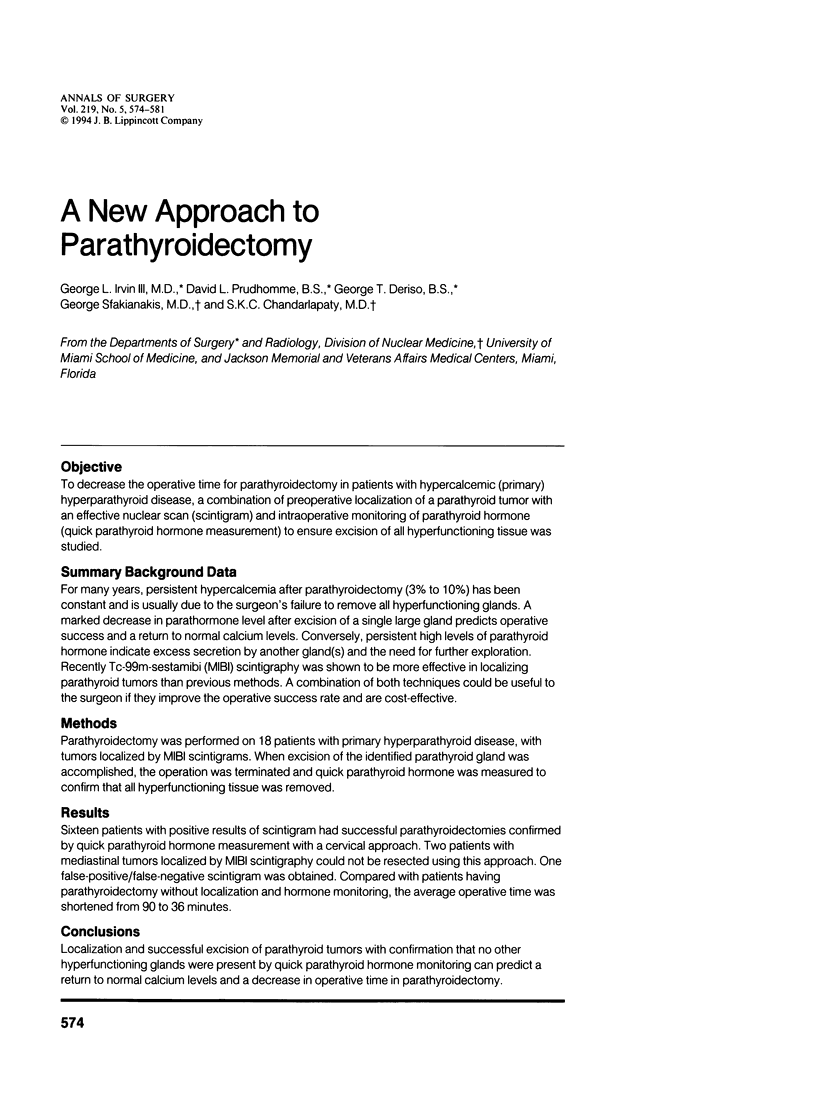

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Auguste L. J., Attie J. N., Schnaap D. Initial failure of surgical exploration in patients with primary hyperparathyroidism. Am J Surg. 1990 Oct;160(4):333–336. doi: 10.1016/s0002-9610(05)80536-7. [DOI] [PubMed] [Google Scholar]
- Bonjer H. J., Bruining H. A., Birkenhager J. C., Nishiyama R. H., Jones M. A., Bagwell C. B. Single and multigland disease in primary hyperparathyroidism: clinical follow-up, histopathology, and flow cytometric DNA analysis. World J Surg. 1992 Jul-Aug;16(4):737–744. doi: 10.1007/BF02067373. [DOI] [PubMed] [Google Scholar]
- Brown R. C., Aston J. P., Weeks I., Woodhead J. S. Circulating intact parathyroid hormone measured by a two-site immunochemiluminometric assay. J Clin Endocrinol Metab. 1987 Sep;65(3):407–414. doi: 10.1210/jcem-65-3-407. [DOI] [PubMed] [Google Scholar]
- Coakley A. J., Kettle A. G., Wells C. P., O'Doherty M. J., Collins R. E. 99Tcm sestamibi--a new agent for parathyroid imaging. Nucl Med Commun. 1989 Nov;10(11):791–794. doi: 10.1097/00006231-198911000-00003. [DOI] [PubMed] [Google Scholar]
- Hage D. S., Kao P. C. High-performance immunoaffinity chromatography and chemiluminescent detection in the automation of a parathyroid hormone sandwich immunoassay. Anal Chem. 1991 Mar 15;63(6):586–595. doi: 10.1021/ac00006a008. [DOI] [PubMed] [Google Scholar]
- Irvin G. L., 3rd, Cohen M. S., Moebus R., Mintz D. H. Primary hyperparathyroidism. Current diagnosis, treatment, and results. Arch Surg. 1972 Nov;105(5):738–740. doi: 10.1001/archsurg.1972.04180110061015. [DOI] [PubMed] [Google Scholar]
- Irvin G. L., 3rd, Dembrow V. D., Prudhomme D. L. Clinical usefulness of an intraoperative "quick parathyroid hormone" assay. Surgery. 1993 Dec;114(6):1019–1023. [PubMed] [Google Scholar]
- Irvin G. L., 3rd, Dembrow V. D., Prudhomme D. L. Operative monitoring of parathyroid gland hyperfunction. Am J Surg. 1991 Oct;162(4):299–302. doi: 10.1016/0002-9610(91)90135-z. [DOI] [PubMed] [Google Scholar]
- Irvin G. L., 3rd, Newell D. J., Morgan S. D. Parathyroid metabolism after operative treatment of hypercalcemic (primary) hyperparathyroidism. Surgery. 1987 Dec;102(6):898–902. [PubMed] [Google Scholar]
- Proye C. A., Carnaille B., Bizard J. P., Quievreux J. L., Lecomte-Houcke M. Multiglandular disease in seemingly sporadic primary hyperparathyroidism revisited: where are we in the early 1990s? A plea against unilateral parathyroid exploration. Surgery. 1992 Dec;112(6):1118–1122. [PubMed] [Google Scholar]
- Shaha A. R., Jaffe B. M. Cervical exploration for primary hyperparathyroidism. J Surg Oncol. 1993 Jan;52(1):14–17. doi: 10.1002/jso.2930520105. [DOI] [PubMed] [Google Scholar]
- Taillefer R., Boucher Y., Potvin C., Lambert R. Detection and localization of parathyroid adenomas in patients with hyperparathyroidism using a single radionuclide imaging procedure with technetium-99m-sestamibi (double-phase study) J Nucl Med. 1992 Oct;33(10):1801–1807. [PubMed] [Google Scholar]
- Wei J. P., Burke G. J., Mansberger A. R., Jr Prospective evaluation of the efficacy of technetium 99m sestamibi and iodine 123 radionuclide imaging of abnormal parathyroid glands. Surgery. 1992 Dec;112(6):1111–1117. [PubMed] [Google Scholar]