

Abstract
We report herein a rare case of complete congenital sternal cleft (absent sternum) and anterior pericardial defect in association with pectus excavatum. In neonates with absent sternum, the sternal bars can be easily approximated by simple suture, due to the flexibility of the cartilaginous thorax. There is also little danger of cardiac compression when the repair is performed early in life.
If reconstruction is delayed, the increased rigidity of the chest wall and the physiologic accommodation of the thoracic organs to the circumference of the chest render simple approximation impossible, without serious compromise of the heart and lungs.
Our patient was a 13-year-old girl, whose case was particularly unusual because of the association of sternal cleft with pectus excavatum. After surgical correction of the pectus excavatum, we were able to construct a sternum by incising the lateral border of each sternal bar, thereby creating flaps that we sutured together at midline. The sternal bars were then approximated by loops of nonabsorbable suture around their circumference.
The patient had an uncomplicated course, and at the 12-month follow-up visit, her sternal appearance was normal. (Tex Heart Inst J 2002;29:206–9)
Key words: Funnel chest, pericardium/abnormalities, sternum/abnormalities, sternum/surgery
Complete congenital sternal cleft (absent sternum) is a very rare anomaly: only 23 cases were summarized by Shamberger and Welch 1 in 1990. In this condition, there is no bone present between the hyoid and the pubis. Absent sternum may be associated with abnormalities of midline fusion other than congenital sternal cleft. 2,3 We report a rare case of complete congenital sternal cleft and anterior pericardial defect in association with pectus excavatum.
Case Report
In December 1999, a 13-year-old girl presented with a complete sternal cleft associated with pectus excavatum, a congenital condition. In addition to the cosmetic concern, there was constant fear of trauma. Physical examination revealed a gap at the site of the sternum (absent sternum) and pectus excavatum (Fig. 1). Pulsations of the heart and great vessels could be seen easily through the defect, which was covered only by a layer of skin. During Valsalva's maneuver, the sternal defect became wider and the bulge of the heart became dramatically more prominent. Band-like scars extended from the umbilicus to the inferior aspect of the sternal defect. Chest radiography and spiral computed tomography (Fig. 2) confirmed the findings of the physical examination. Other intrathoracic structures were reported to be normal.
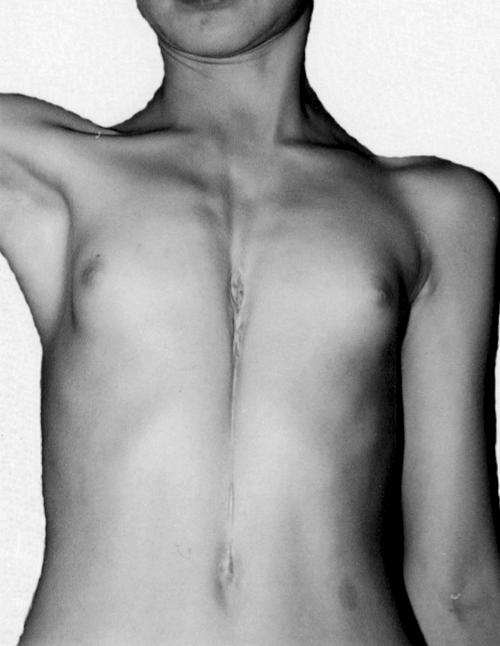
Fig. 1 Preoperative photograph of the patient's anterior chest wall shows complete sternal cleft.

Fig. 2 Spiral computed tomographic scan of the chest, with 3-dimensional reconstruction, shows the complete sternal cleft.
At surgery, the skin overlying the sternal defect was incised along the midline. The pericardium was found to be absent anteriorly, in a line corresponding with the length of the defect. The heart and great vessels were normal. The pericardium was refashioned and closed directly, at the midline.
The pectoralis muscles were incised only over the cartilage excisions. There were 5 abnormal cartilages on each side of the rib cage, fragments of which were excised bilaterally, beneath the perichondrium (Figs. 3A and 3B). After the pectus excavatum deformity was in that manner corrected, the periosteum of each sternal bar was incised on its lateral border (Fig. 3A). Both of the flaps so created were then turned upside down and sutured together in the midline with 3-0 absorbable sutures (Fig. 3B). The 2 sternal bars were then approximated with 5 interrupted 1-0 nonabsorbable sutures (Fig. 3C). The closure was completed with the approximation of the 2 major pectoralis muscles at the midline. Because of the extensive resection of deformed cartilage, the 2 sternal bars were approximated easily, without the interposition of costal cartilage. Finally, we closed tightly the perichondrium of the abnormal cartilages. We didn't need to perform additional internal or external fixation of the sternum to prevent paradoxical respiration. Closed suction drains were placed above and below the pectoralis muscle flaps. The overlying fasciocutaneous flaps were advanced to achieve primary skin closure.
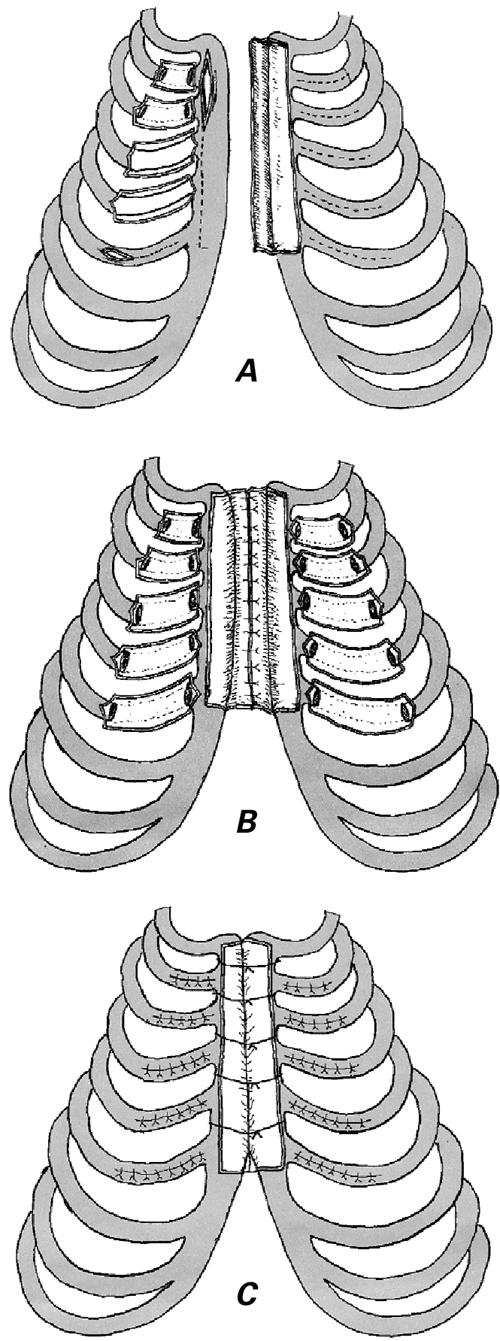
Fig. 3 A and B) To correct the pectus excavatum deformity, the abnormal cartilages were excised bilaterally, beneath the perichondrium. The periosteum of the each sternal bar was then incised on its lateral border, creating flaps that were sutured together in the midline with absorbable sutures. C) The 2 sternal bars were approximated with nonabsorbable sutures.
The patient had an uncomplicated postoperative course and was discharged 4 days after surgery. Chest radiography and computed tomographic scanning performed during the 12th postoperative month showed a healthy closure of the defect (Fig. 4).
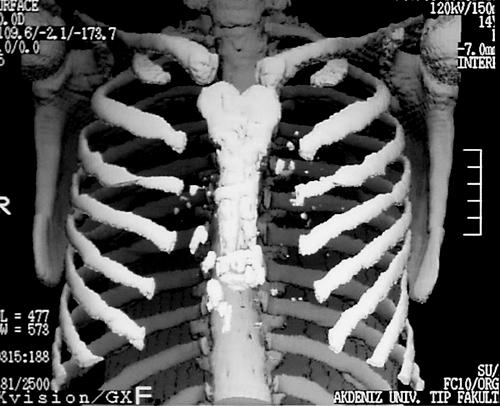
Fig. 4 Postoperative spiral computed tomographic scan of the thorax, with 3-dimensional reconstruction, shows the successful result.
Discussion
In embryonic life, the sternum has its origin in the lateral plate mesoderm. Cells from 2 bands of mesoderm on either side of the anterior chest wall migrate toward the midline and become fused by the 10th week, thus forming the sternum. The manubrium is formed by primordia between the ventral ends of the developing clavicles. Very rarely, the sternal bars fail to join in the midline, which results in a complete sternal cleft. 3
In this challenging anomaly, the underlying mediastinal structures (most especially the heart and great vessels) may easily be injured by external trauma. In addition, the deformity is cosmetically unpleasant and quite alarming to the young patient and his or her family. 4
Congenital sternal cleft is classified as complete or incomplete, 5 with complete cleft the rarer form. 1 Incomplete clefts are subdivided into superior and inferior ones. Inferior incomplete cleft may occur as an isolated entity, although it is usually associated with other developmental defects of the anterior chest wall such as ectopia cordis, or, in Cantrell's pentalogy, with a combination of defects involving the abdominal wall, sternum, diaphragm, pericardium, and heart. 4
The association of sternal cleft with pectus excavatum is rare. The currently accepted cause of pectus excavatum is rapid, misdirected growth of the lower costal cartilages, which form congenitally in a concave manner and create a depressed sternum. 3 When these 2 anomalies occur together, repair of pectus excavatum actually facilitates approximation of the sternal bars.
A number of methods for repair of cleft sternum have been reported, including primary approximation, sliding or rotating chondrotomies, and the use of prosthetic grafts or of flaps of bone, cartilage, autogenous tissue, or pectoralis major muscle. 2,6
In neonates, the sternal bars can be easily approximated by simple suture, due to the flexibility of the cartilaginous thorax. This also enables approximation of the sternal bars with less danger of cardiac compression. 4
Patients who have not undergone repair during this early period will probably require reconstruction later. The increasing rigidity of the chest wall and the physiologic accommodation of the thoracic organs to an accustomed circumference of the chest render simple approximation impossible, without serious compromise of the heart and lungs. This difficulty distinguishes these older patients from newborns.
In our patient, the transverse width of the sternal cleft was greatest at the upper part, measuring 3 cm upon expiration and 5 cm upon inspiration. Because of the extensive resection of deformed cartilage, the 2 sternal bars could be easily approximated, without resorting to other methods.
The 3rd abnormality of midline fusion in our patient was a pericardial defect. Anterior pericardial defect commonly occurs with sternal cleft, but it is no problem to treat.
In conclusion, this case is especially unusual because of the association of complete sternal cleft with pectus excavatum. In the combined repair of these 2 anomalies, the sternal bars can quite possibly be approximated by simple sutures, with no danger of cardiac compression. Yet the surgical procedure needs to be tailored, particularly among adults, to the individual defect.
Footnotes
Address for reprints: Alpay Sarper, MD, Akdeniz Universitesi Tip Fakultesi, Gogus Cerrahisi Anabilim Dali, Antalya, Turkey 07070
References
- 1.Shamberger RC, Welch KJ. Sternal defects. Pediatr Surg Int 1990;5:156–64.
- 2.Suri RK, Sharma RK, Jha NK, Sharma BK. Complete congenital sternal cleft in an adult: repair by autogenous tissues. Ann Thorac Surg 1996;62:573–5. [PubMed]
- 3.Ravitch MM. Disorders of the sternum and the thoracic wall. In: Sabiston DC Jr, Spencer FC, editors. Gibbon's surgery of the chest. 4th ed. Philadelphia: WB Saunders; 1983. p. 318–60.
- 4.de Campos JR, Filomeno LT, Fernandez A, Ruiz RL, Minamoto H, Werebe Ede C, Jatene FB. Repair of congenital sternal cleft in infants and adolescents. Ann Thorac Surg 1998;66:1151–4. [DOI] [PubMed]
- 5.Samarrai AA, Charmockly HA, Attra AA. Complete cleft sternum: classification and surgical repair. Int Surg 1985;70:71–3. [PubMed]
- 6.Snyder BJ, Robbins RC, Ramos D. Primary repair of complete sternal cleft with pectoralis major muscle flaps. Ann Thorac Surg 1996;61:983–4. [DOI] [PubMed]