

Abstract
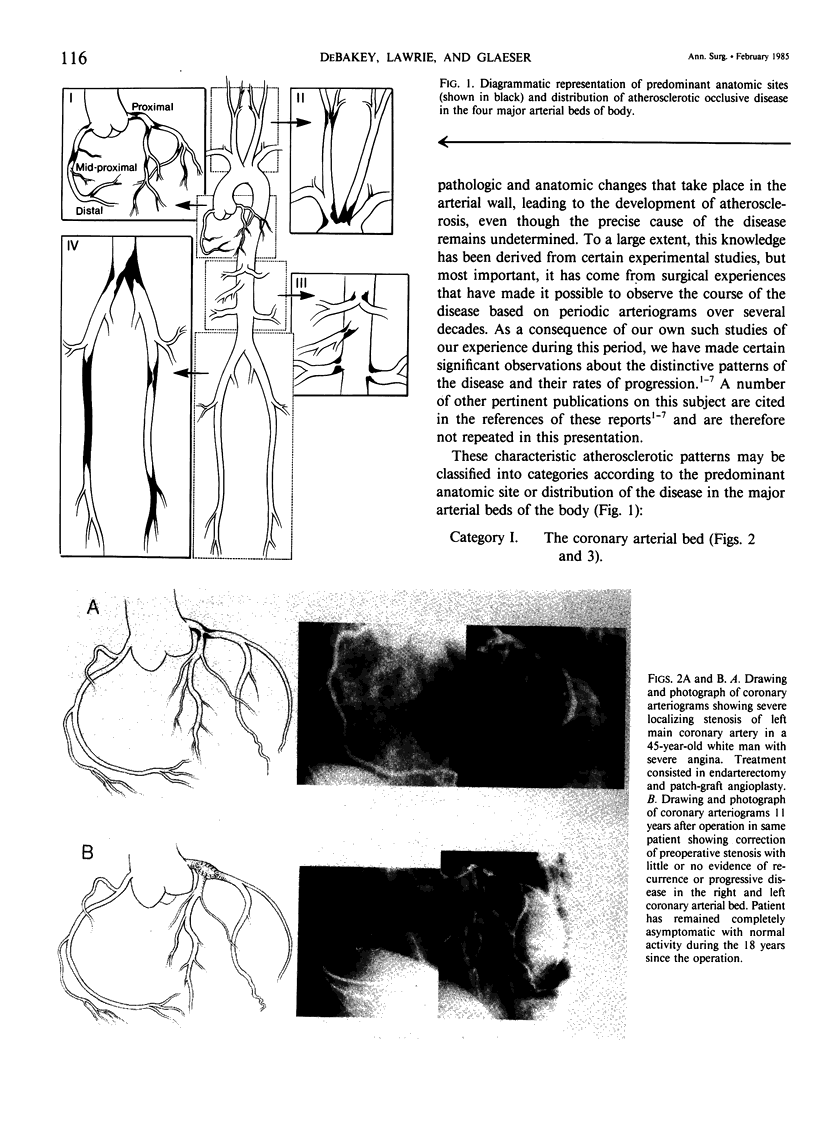
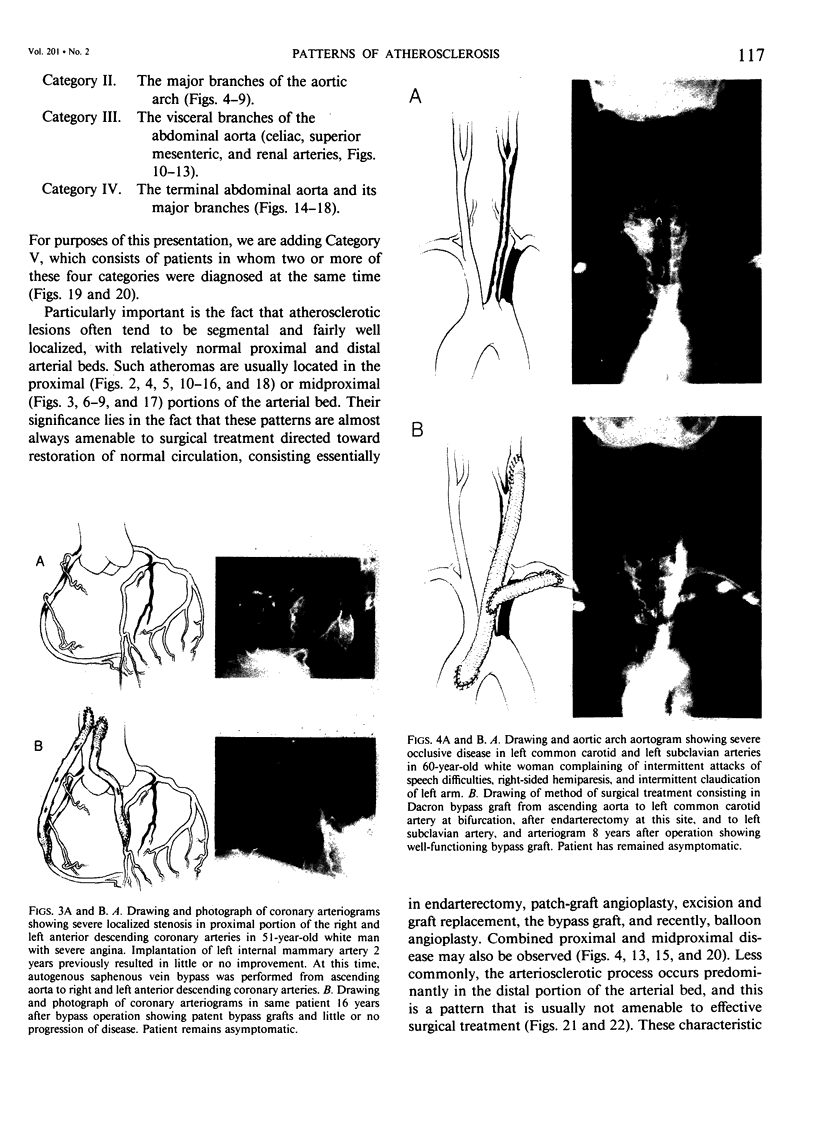
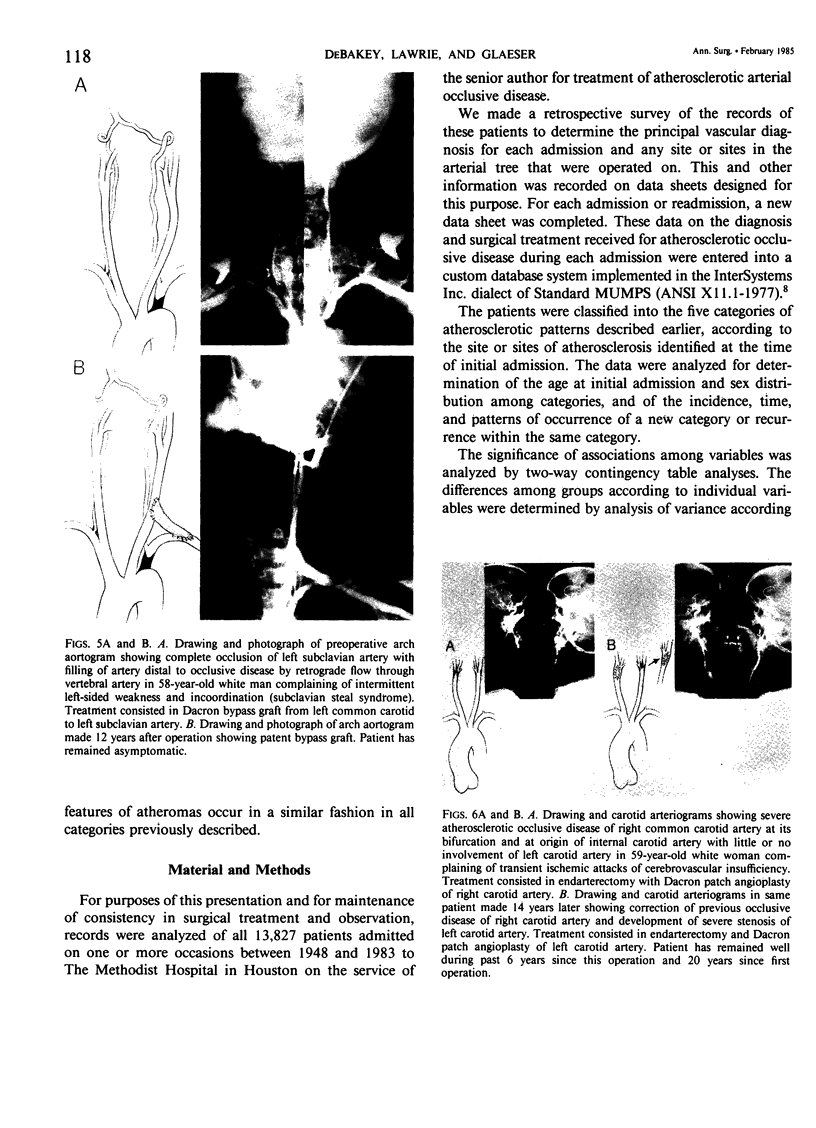
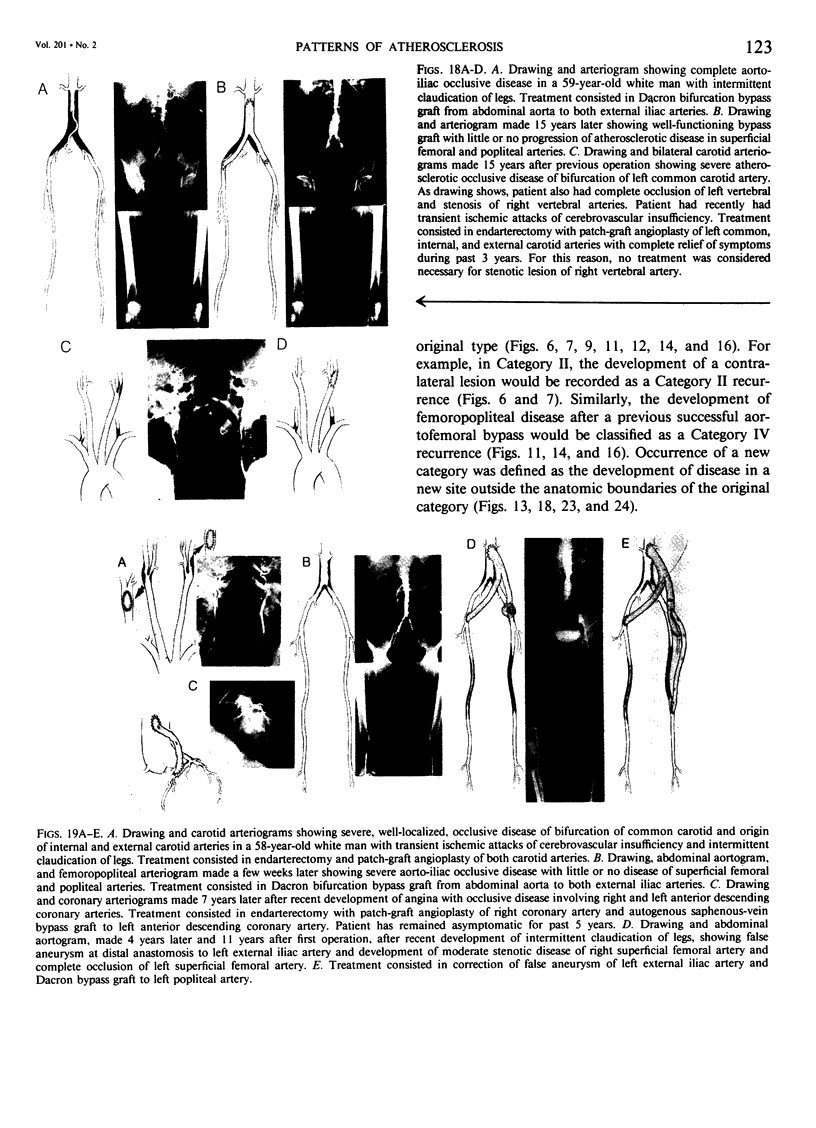
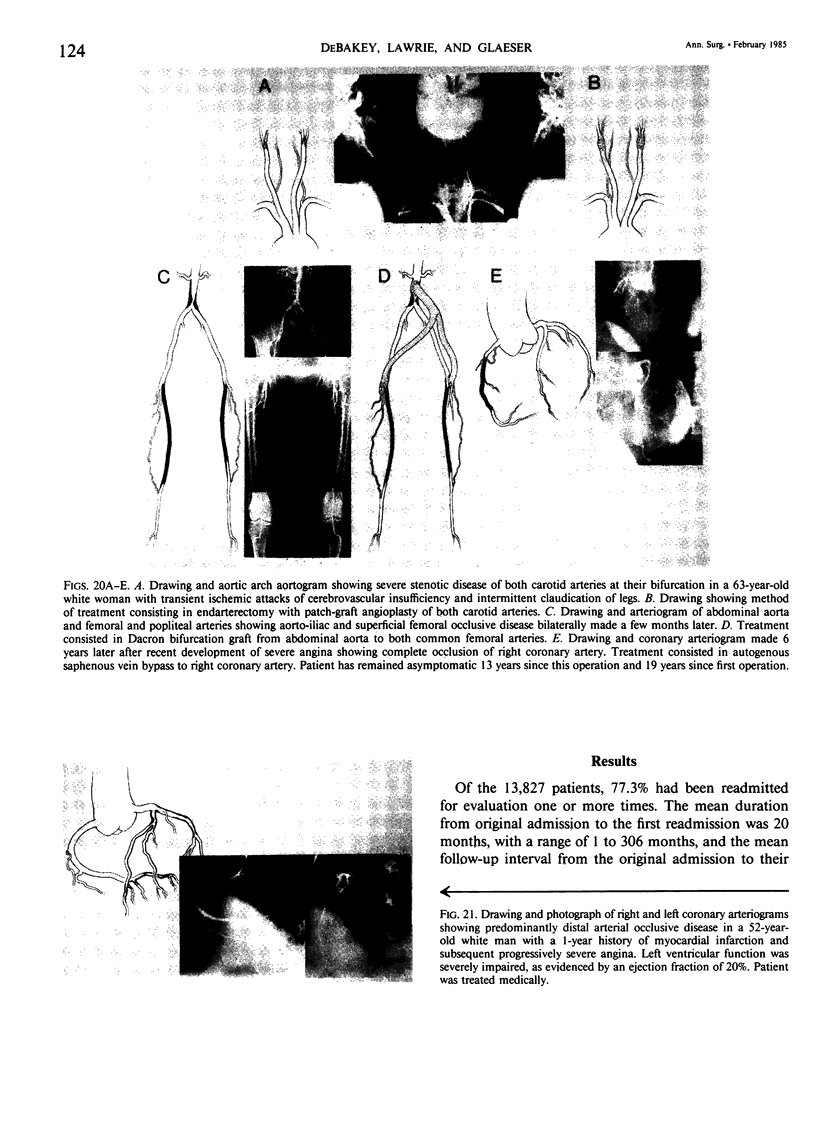
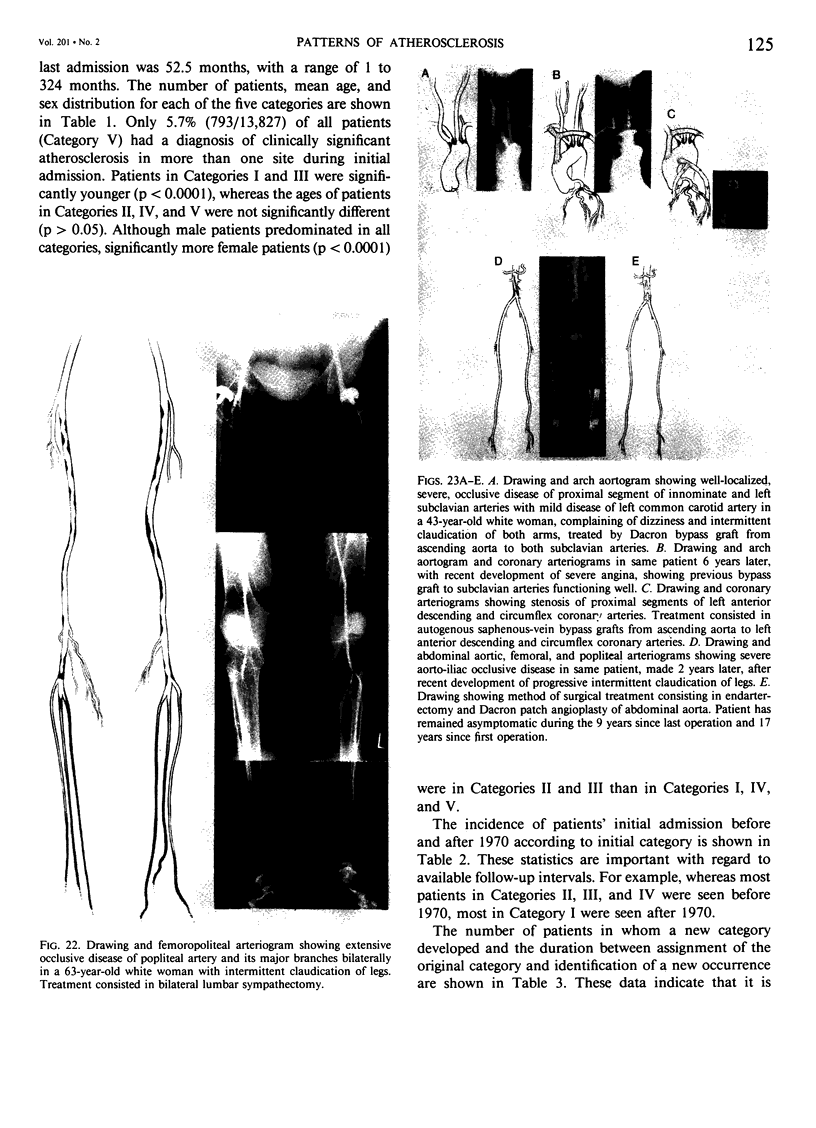
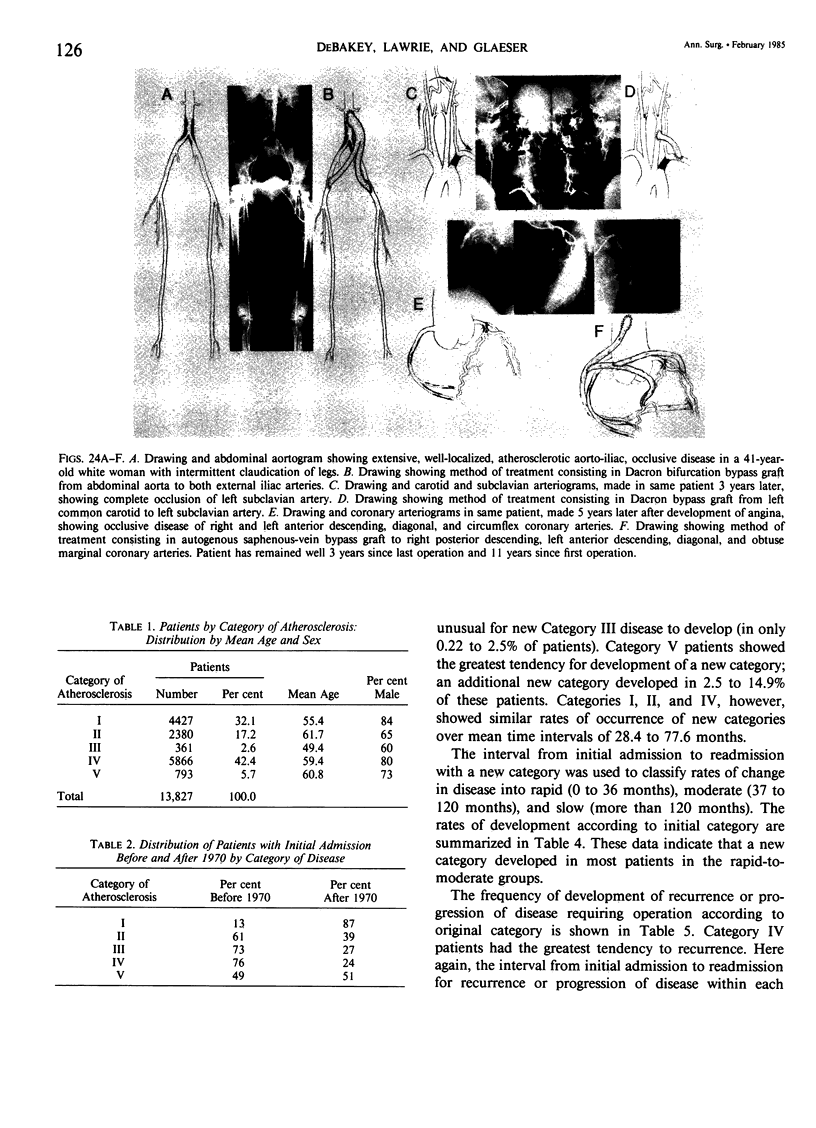
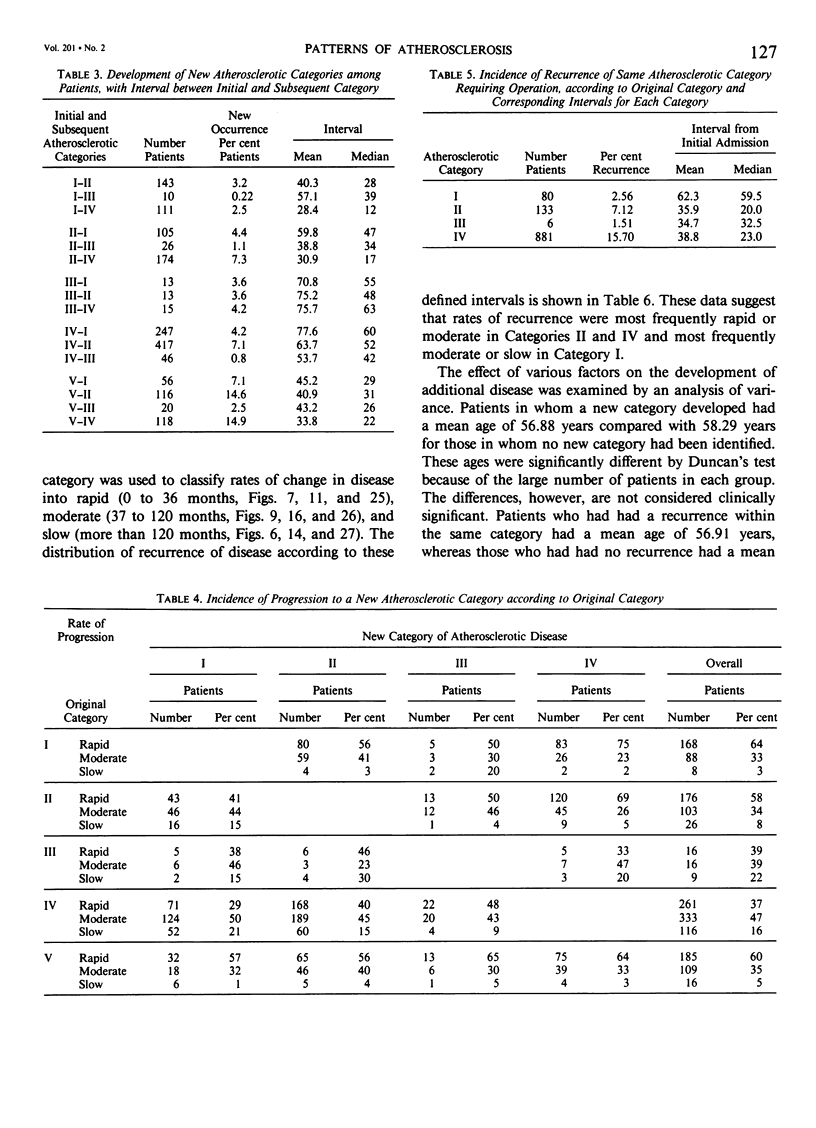
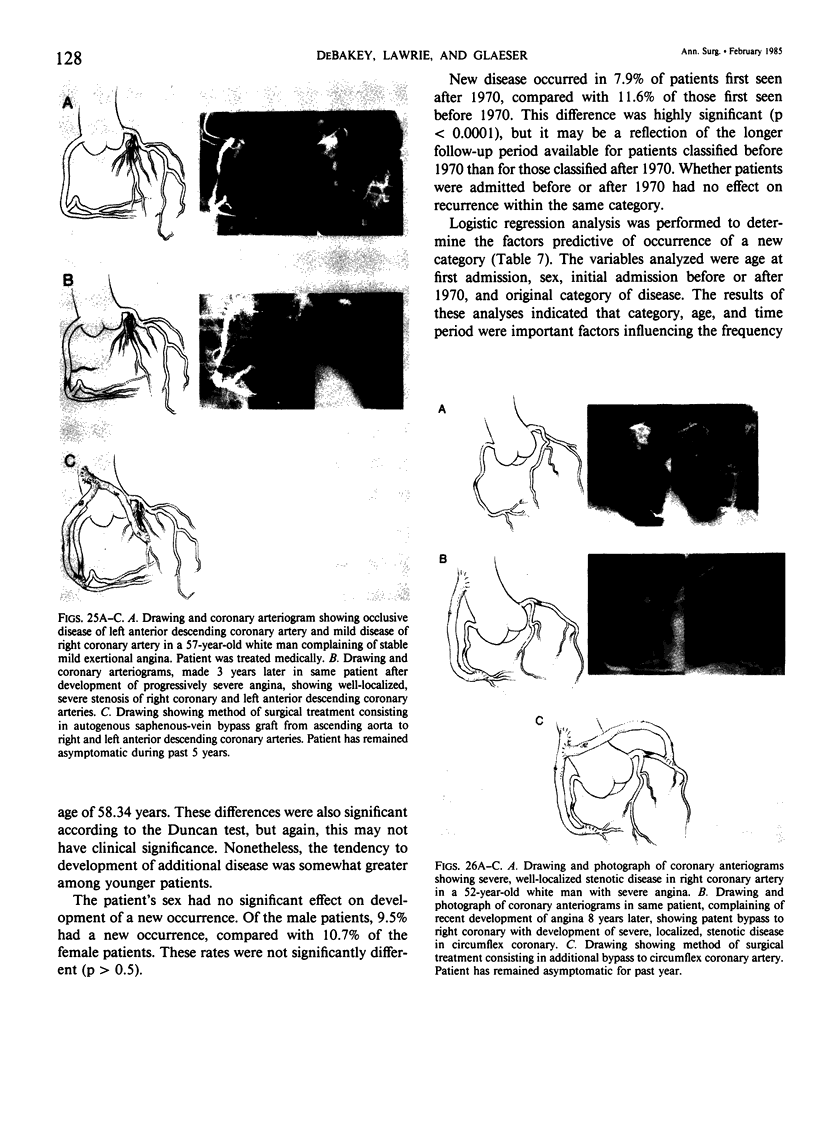
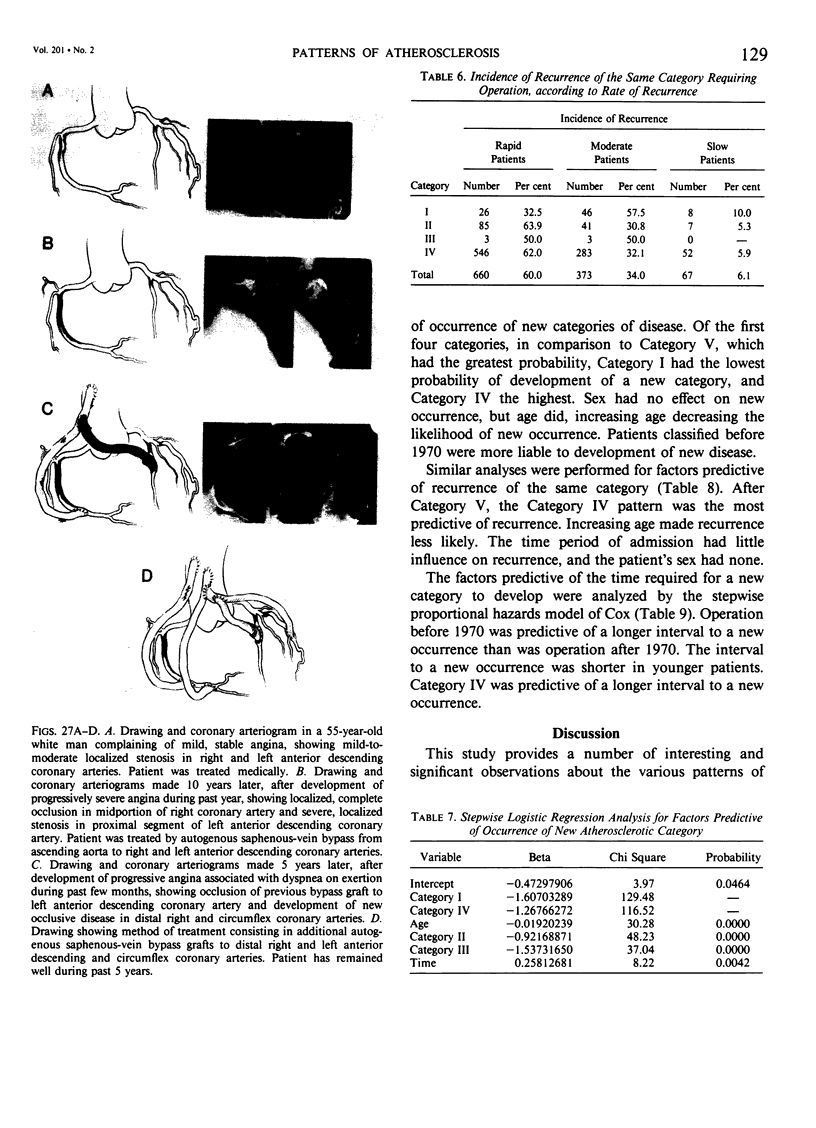
The records of 13,827 patients admitted on one or more occasions to The Methodist Hospital in Houston on the service of the senior author for the treatment of arterial atherosclerotic occlusive disease from 1948 to 1983 were analyzed. The data derived from this analysis are believed to support the concept that atherosclerotic occlusive disease tends to assume characteristic patterns that may be classified, by predominant site or distribution of the disease, into five major categories: (I) the coronary arterial bed, (II) the major branches of the aortic arch, (III) the visceral arterial branches of the abdominal aorta, (IV) the terminal abdominal aorta and its major branches, and (V) a combination of two or more of these categories occurring simultaneously. Category IV had the highest proportion of patients (about two-fifths), Category I the second highest (almost one-third), and Category III had the lowest percentage (3%). Atherosclerotic occlusive disease in all categories tends to be well localized and usually occurs in the proximal or midproximal portions of the arterial bed. Such lesions are amenable to effective surgical treatment directed toward restoration of normal circulation. Less commonly, however, the occlusive disease in all categories occurs predominantly in the distal portions of the arterial bed, and such lesions are usually not amenable to effective surgical treatment. Patients in Categories I and III were significantly younger than those in the other categories and, although males predominated in all categories, Categories II and III contained significantly more female patients than did the other categories. In general, however, female patients behaved like male patients in virtually all aspects of the study. The rates of progression of the disease may be classified into: rapid (0 to 36 months), moderate (37 to 120 months), and slow (more than 120 months). The rapid and moderate rates of progression occurred most frequently in Categories II and IV, and the moderate and slow rates occurred most frequently in Category I. The possibility for development of recurrence or progression of disease in the same category and in a new category was significantly greater in younger patients. The patient's sex had no significant influence in this regard. Among the various categories, patients in Category IV had the highest incidence of development of disease in a new category, and Category I had the lowest incidence. Patients originally in Category II had a somewhat greater tendency to development of disease in Category IV, and patients originally in Category IV, for development of disease in Category II.(ABSTRACT TRUNCATED AT 400 WORDS)
Full text
PDF

Images in this article







Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- DE BAKEY M. E. Changing concepts in vascular surgery. J Cardiovasc Surg (Torino) 1960 Jul;1:3–44. [PubMed] [Google Scholar]
- DEBAKEY M. E. BASIC CONCEPTS OF THERAPY IN ARTERIAL DISEASE. Bull N Y Acad Med. 1963 Nov;39:707–749. [PMC free article] [PubMed] [Google Scholar]
- DeBakey M. E. Developments in cardiovascular surgery. Cardiovasc Res Cent Bull. 1980 Jul-Sep;19(1):5–32. [PubMed] [Google Scholar]
- DeBakey M. E. Research related to surgical treatment of aortic and peripheral vascular disease. Circulation. 1979 Dec;60(7):1619–1635. doi: 10.1161/01.cir.60.7.1619. [DOI] [PubMed] [Google Scholar]
- DeBakey M. E. The development of vascular surgery. Am J Surg. 1979 Jun;137(6):697–738. doi: 10.1016/0002-9610(79)90083-7. [DOI] [PubMed] [Google Scholar]