

Abstract
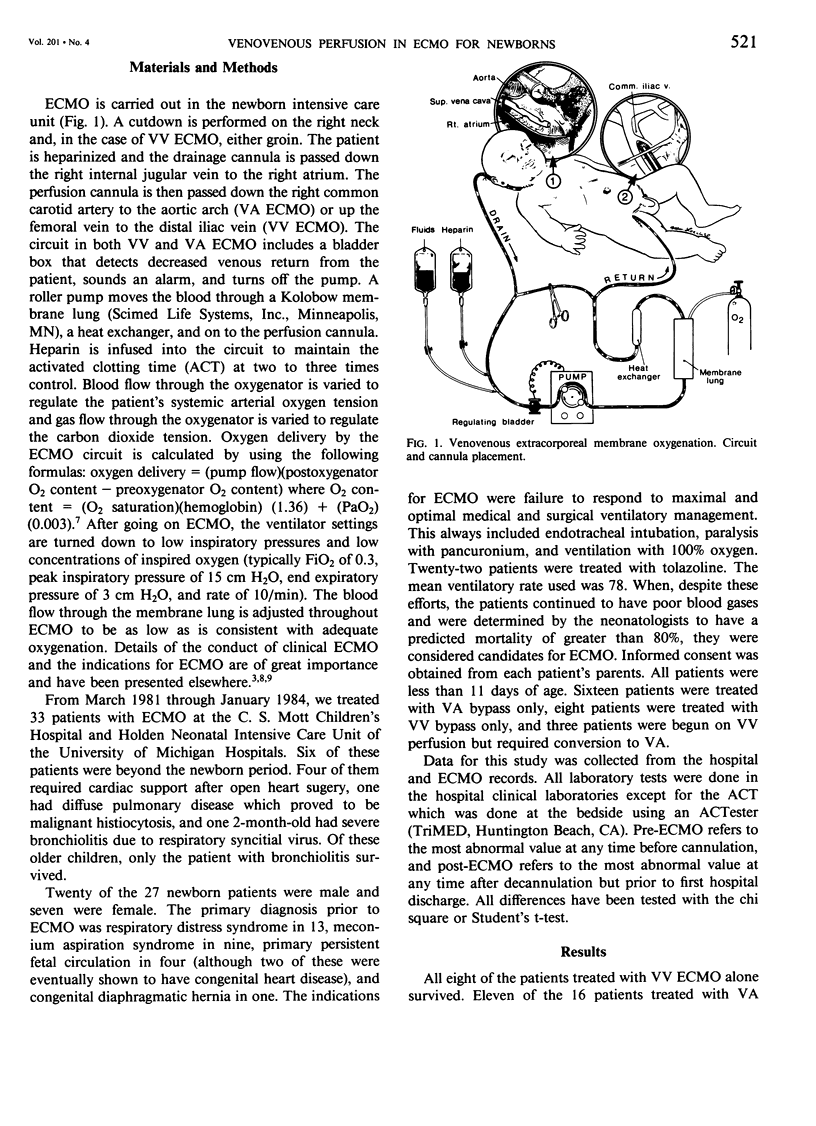
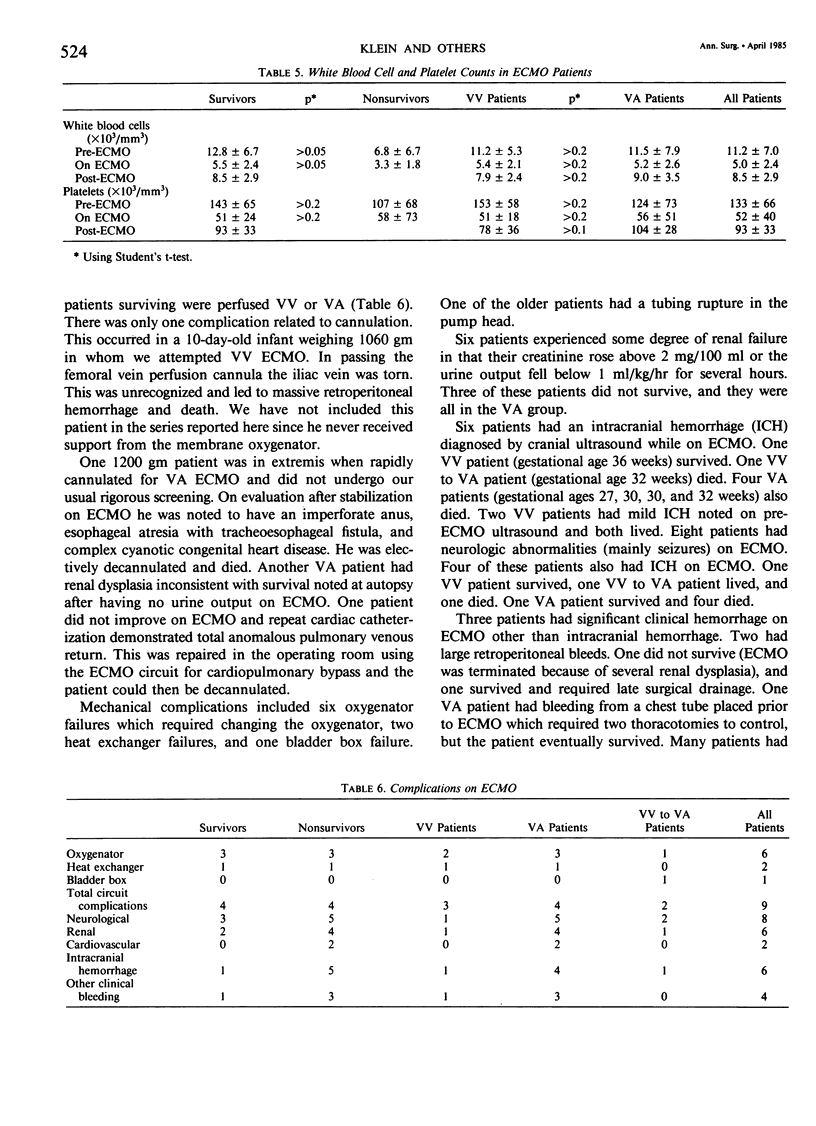
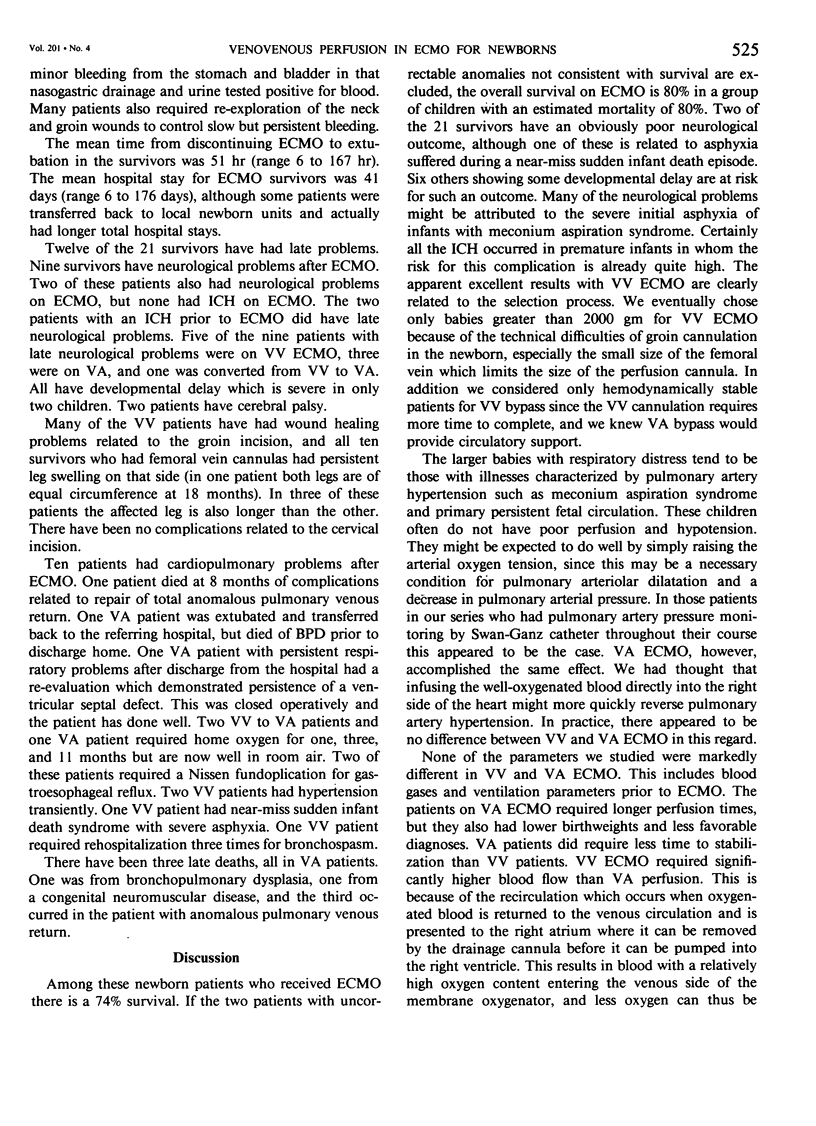
Venoarterial (VA) extracorporeal membrane oxygenation (ECMO) has been successful in the treatment of newborns less than 1 week of age and greater than 2000 gm birthweight with respiratory failure resistant to current medical and surgical management. While VA ECMO supports the heart as well as the lungs, it has the disadvantage of requiring carotid artery ligation and the possibility of perfusing air bubbles or particles into the arterial tree. We have treated 11 newborns with respiratory failure with venovenous (VV) ECMO returning the oxygenated blood to a cannula in the distal iliac vein. We compared these patients with 16 patients treated during the same period of time with VA ECMO. Three of the 11 VV patients required conversion to VA ECMO because of inadequate oxygenation and unstable hemodynamic situations. Ten of the 11 VV patients survived. Eleven of the 16 VA patients survived. The better survival in these patients treated with VV ECMO is attributed to their more favorable initial condition compared to patients treated with VA ECMO. The disadvantages of VV ECMO include a longer operative time to place the cannulas, groin wound problems, and persistent leg swelling along with the necessity to convert some patients to VA ECMO. Although this experience demonstrates that newborns with severe respiratory failure can be supported with VV ECMO, the complications and lack of practical advantages over VA lead us to recommend VA ECMO for routine clinical use at present.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Andrews A. F., Klein M. D., Toomasian J. M., Roloff D. W., Bartlett R. H. Venovenous extracorporeal membrane oxygenation in neonates with respiratory failure. J Pediatr Surg. 1983 Aug;18(4):339–346. doi: 10.1016/s0022-3468(83)80178-x. [DOI] [PubMed] [Google Scholar]
- Andrews A. F., Toomasian J., Oram A., Bartlett R. H. Total respiratory support with venovenous (VV) ECMO. Trans Am Soc Artif Intern Organs. 1982;28:350–353. [PubMed] [Google Scholar]
- Bartlett R. H., Andrews A. F., Toomasian J. M., Haiduc N. J., Gazzaniga A. B. Extracorporeal membrane oxygenation for newborn respiratory failure: forty-five cases. Surgery. 1982 Aug;92(2):425–433. [PubMed] [Google Scholar]
- Bartlett R. H., Gazzaniga A. B. Extracorporeal circulation for cardiopulmonary failure. Curr Probl Surg. 1978 May;15(5):1–96. doi: 10.1016/s0011-3840(78)80008-2. [DOI] [PubMed] [Google Scholar]
- Hardesty R. L., Griffith B. P., Debski R. F., Jeffries M. R., Borovetz H. S. Extracorporeal membrane oxygenation. Successful treatment of persistent fetal circulation following repair of congenital diaphragmatic hernia. J Thorac Cardiovasc Surg. 1981 Apr;81(4):556–563. [PubMed] [Google Scholar]
- Kirkpatrick B. V., Krummel T. M., Mueller D. G., Ormazabal M. A., Greenfield L. J., Salzberg A. M. Use of extracorporeal membrane oxygenation for respiratory failure in term infants. Pediatrics. 1983 Dec;72(6):872–876. [PubMed] [Google Scholar]
- Krummel T. M., Greenfield L. J., Kirkpatrick B. V., Mueller D. G., Ormazabal M., Salzberg A. M. Clinical use of an extracorporeal membrane oxygenator in neonatal pulmonary failure. J Pediatr Surg. 1982 Oct;17(5):525–531. doi: 10.1016/s0022-3468(82)80102-4. [DOI] [PubMed] [Google Scholar]