

Abstract
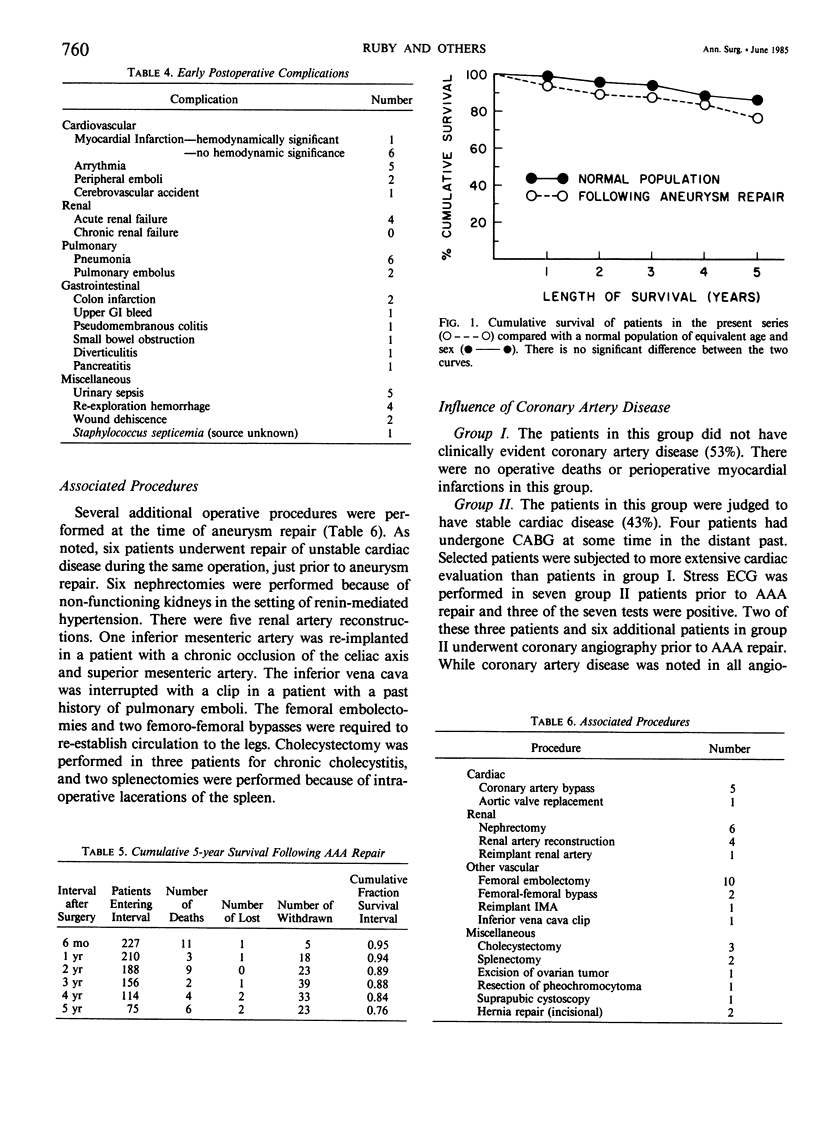
The chief cause of operative mortality after abdominal aortic aneurysm (AAA) repair is myocardial infarction. For this reason, routine coronary angiography followed by prophylactic coronary artery bypass grafting (CABG) prior to AAA repair has been recommended by some surgeons. We report here the results of the selective use of a combined operation. Two hundred twenty-seven patients had elective or emergency repair of nonruptured AAA on our service from 1972 to 1983. Prior to surgery, all patients underwent careful clinical evaluation for the presence of coronary artery disease (CAD) and were classified into the following: group I (n = 121), no clinical evidence of CAD, 53%; group II (n = 96), clinical evidence of stable CAD, symptomatic or asymptomatic, 42%; group III (n = 10), unstable CAD, five per cent; Group IIIa (n = 4), asymptomatic AAA; and group IIIb (n = 6), symptomatic AAA. Seven patients ultimately assigned to group II underwent stress electrocardiogram (ECG) and eight group II patients had coronary angiography before surgery. All patients in groups I and II underwent elective or urgent repair of their AAA without CABG. Prior to surgery, these patients were managed with placement of a pulmonary artery catheter and incremental volume loading to construct a left ventricular performance curve as a guide to surgical fluid replacement. All were carefully monitored for at least 48 hours after surgery in an intensive care unit. Four patients (group IIIa) with unstable CAD and asymptomatic AAA underwent CABG followed by elective AAA repair within six months. Six patients (group IIIb) with unstable CAD and symptomatic AAA underwent combined open heart surgery (CABG and, in one patient, valve replacement) and AAA repair as a single operation. There was no operative mortality in group III patients. Thirty-day operative mortality for the entire group of 227 patients was 1.3% (three deaths), with only one death from a myocardial infarction (0.4%). While there is clearly a high incidence of CAD in patients with AAA, the present results indicate that these individuals can be managed with low risk by a selective approach based upon clinical assessment of their CAD. Our experience further demonstrates that patients with unstable CAD and symptomatic AAA may have both lesions safely repaired as a single operative procedure.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Attia R. R., Murphy J. D., Snider M., Lappas D. G., Darling R. C., Lowenstein E. Myocardial ischemia due to infrarenal aortic cross-clamping during aortic surgery in patients with severe coronary artery disease. Circulation. 1976 Jun;53(6):961–965. doi: 10.1161/01.cir.53.6.961. [DOI] [PubMed] [Google Scholar]
- Bush H. L., Jr, LoGerfo F. W., Weisel R. D., Mannick J. A., Hechtman H. B. Assessment of myocardial performance and optimal volume loading during elective abdominal aortic aneurysm resection. Arch Surg. 1977 Nov;112(11):1301–1305. doi: 10.1001/archsurg.1977.01370110035003. [DOI] [PubMed] [Google Scholar]
- CUTLER S. J., EDERER F. Maximum utilization of the life table method in analyzing survival. J Chronic Dis. 1958 Dec;8(6):699–712. doi: 10.1016/0021-9681(58)90126-7. [DOI] [PubMed] [Google Scholar]
- Cooperman M., Pflug B., Martin E. W., Jr, Evans W. E. Cardiovascular risk factors in patients with peripheral vascular disease. Surgery. 1978 Oct;84(4):505–509. [PubMed] [Google Scholar]
- Couch N. P., Lane F. C., Crane C. Management and mortality in resection of abdominal aortic aneurysms. A study of 114 cases. Am J Surg. 1970 Apr;119(4):408–416. doi: 10.1016/0002-9610(70)90142-x. [DOI] [PubMed] [Google Scholar]
- Crawford E. S., Saleh S. A., Babb J. W., 3rd, Glaeser D. H., Vaccaro P. S., Silvers A. Infrarenal abdominal aortic aneurysm: factors influencing survival after operation performed over a 25-year period. Ann Surg. 1981 Jun;193(6):699–709. doi: 10.1097/00000658-198106000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Creech O., Jr Endo-aneurysmorrhaphy and treatment of aortic aneurysm. Ann Surg. 1966 Dec;164(6):935–946. doi: 10.1097/00000658-196612000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Creech O., Jr Endo-aneurysmorrhaphy and treatment of aortic aneurysm. Ann Surg. 1966 Dec;164(6):935–946. doi: 10.1097/00000658-196612000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edwards W. H., Mulherin J. L., Jr, Walker W. E. Vascular reconstructive surgery following myocardial revascularization. Ann Surg. 1978 Jun;187(6):653–657. doi: 10.1097/00000658-197806000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gage A. A., Bhayana J. N., Balu V., Hook N. Assessment of cardiac risk in surgical patients. Arch Surg. 1977 Dec;112(12):1488–1492. doi: 10.1001/archsurg.1977.01370120078009. [DOI] [PubMed] [Google Scholar]
- Goldman L., Cook E. F., Mitchell N., Flatley M., Sherman H., Rosati R., Harrell F., Lee K., Cohn P. F. Incremental value of the exercise test for diagnosing the presence or absence of coronary artery disease. Circulation. 1982 Nov;66(5):945–953. doi: 10.1161/01.cir.66.5.945. [DOI] [PubMed] [Google Scholar]
- Hertzer N. R., Beven E. G., Young J. R., O'Hara P. J., Ruschhaupt W. F., 3rd, Graor R. A., Dewolfe V. G., Maljovec L. C. Coronary artery disease in peripheral vascular patients. A classification of 1000 coronary angiograms and results of surgical management. Ann Surg. 1984 Feb;199(2):223–233. doi: 10.1097/00000658-198402000-00016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hertzer N. R. Fatal myocardial infarction following abdominal aortic aneurysm resection. Three hundred forty-three patients followed 6--11 years postoperatively. Ann Surg. 1980 Nov;192(5):667–673. doi: 10.1097/00000658-198019250-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hertzer N. R., Young J. R., Kramer J. R., Phillips D. F., deWolfe V. G., Ruschhaupt W. F., 3rd, Beven E. G. Routine coronary angiography prior to elective aortic reconstruction: results of selective myocardial revascularization in patients with peripheral vascular disease. Arch Surg. 1979 Nov;114(11):1336–1344. doi: 10.1001/archsurg.1979.01370350138018. [DOI] [PubMed] [Google Scholar]
- Hollier L. H., Plate G., O'Brien P. C., Kazmier F. J., Gloviczki P., Pairolero P. C., Cherry K. J. Late survival after abdominal aortic aneurysm repair: influence of coronary artery disease. J Vasc Surg. 1984 Mar;1(2):290–299. [PubMed] [Google Scholar]
- Mahar L. J., Steen P. A., Tinker J. H., Vlietstra R. E., Smith H. C., Pluth J. R. Perioperative myocardial infarction in patients with coronary artery disease with and without aorta--coronary artery bypass grafts. J Thorac Cardiovasc Surg. 1978 Oct;76(4):533–537. [PubMed] [Google Scholar]
- McCollum C. H., Garcia-Rinaldi R., Graham J. M., DeBakey M. E. Myocardial revascularization prior to subsequent major surgery in patients with coronary artery disease. Surgery. 1977 Mar;81(3):302–304. [PubMed] [Google Scholar]
- Whittemore A. D., Clowes A. W., Hechtman H. B., Mannick J. A. Aortic aneurysm repair. Reduced operative mortality associated with maintenance of optimal cardiac performance. Ann Surg. 1980 Sep;192(3):414–421. doi: 10.1097/00000658-198009000-00017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Young A. E., Sandberg G. W., Couch N. P. The reduction of mortality of abdominal aortic aneurysm resection. Am J Surg. 1977 Nov;134(5):585–590. doi: 10.1016/0002-9610(77)90440-8. [DOI] [PubMed] [Google Scholar]