

Abstract
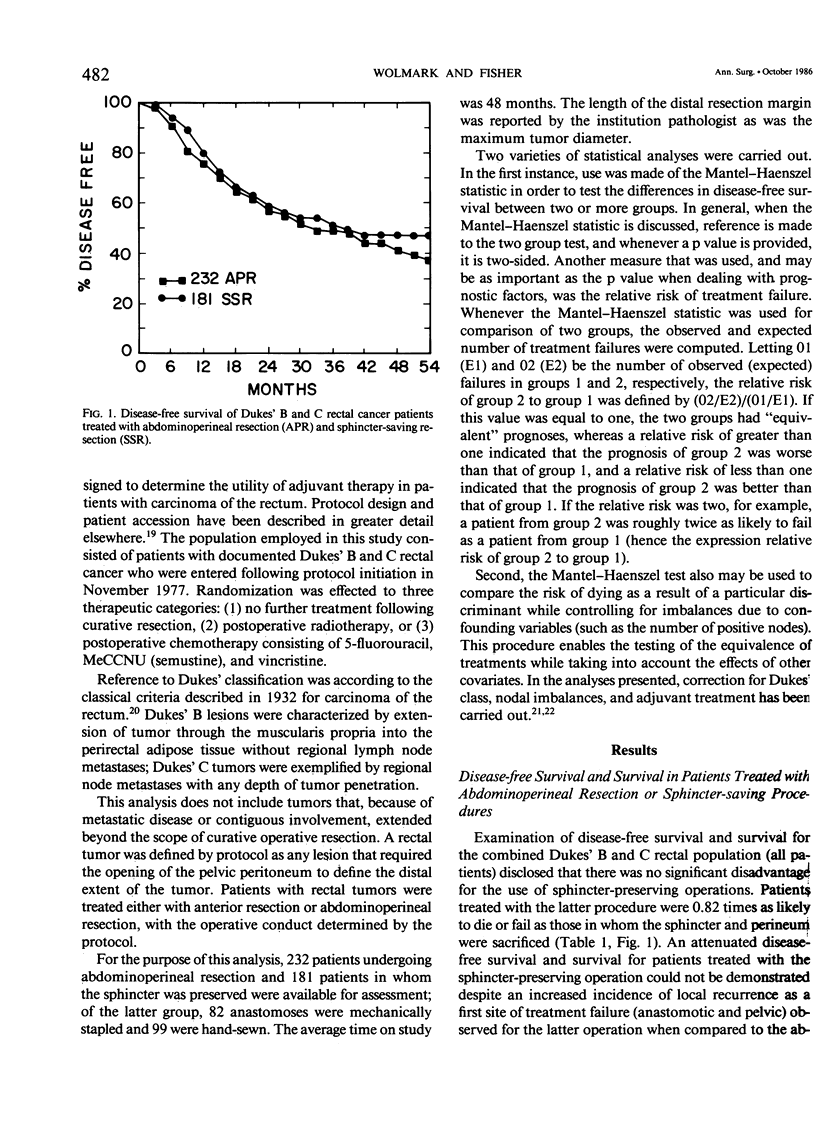
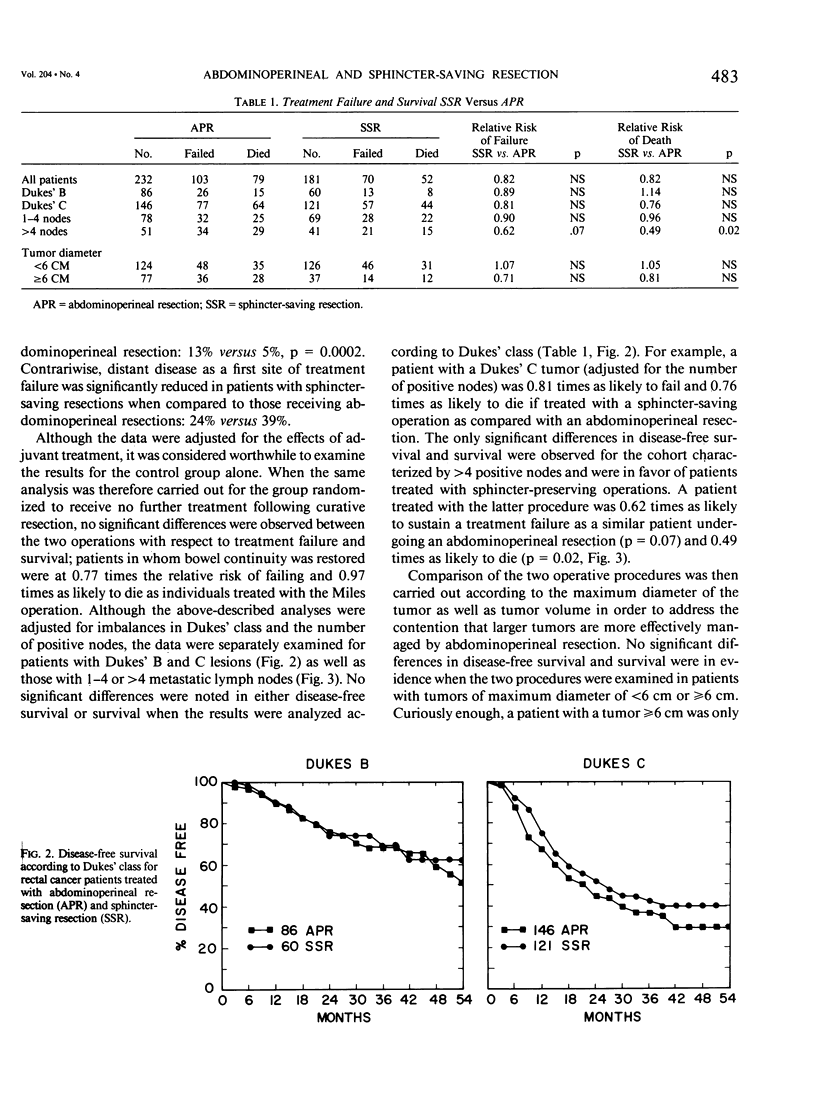
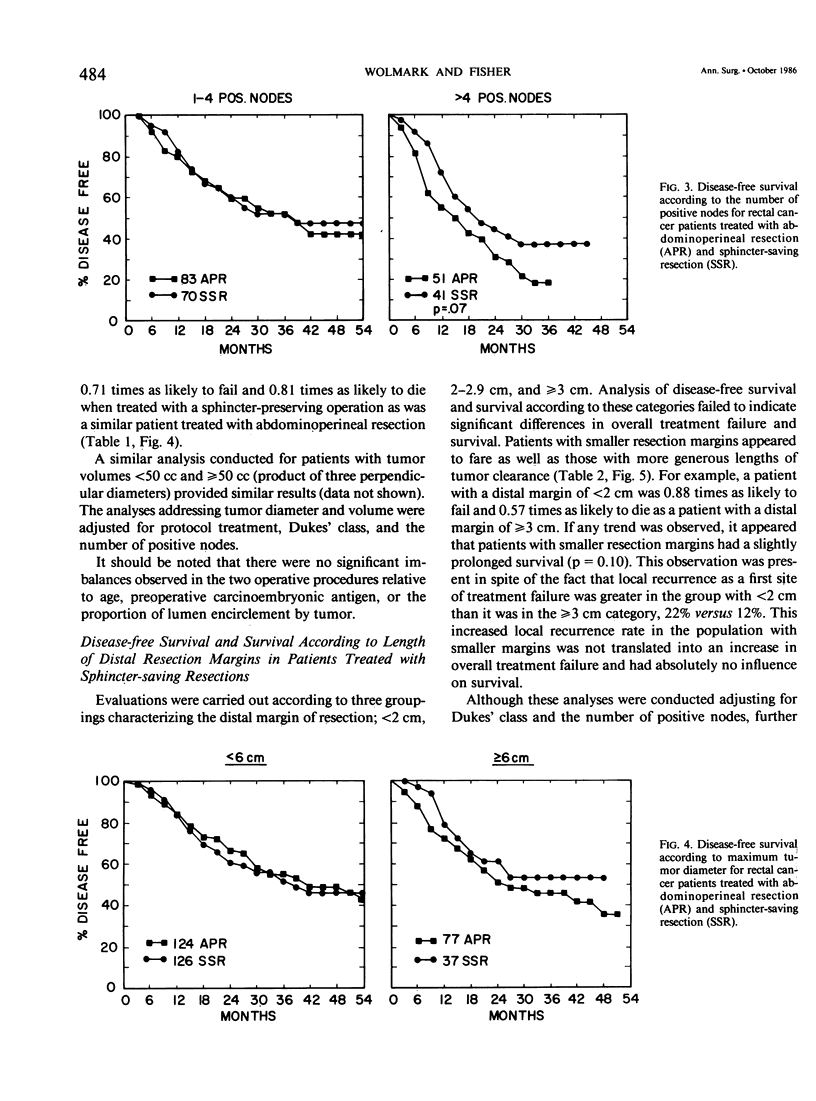
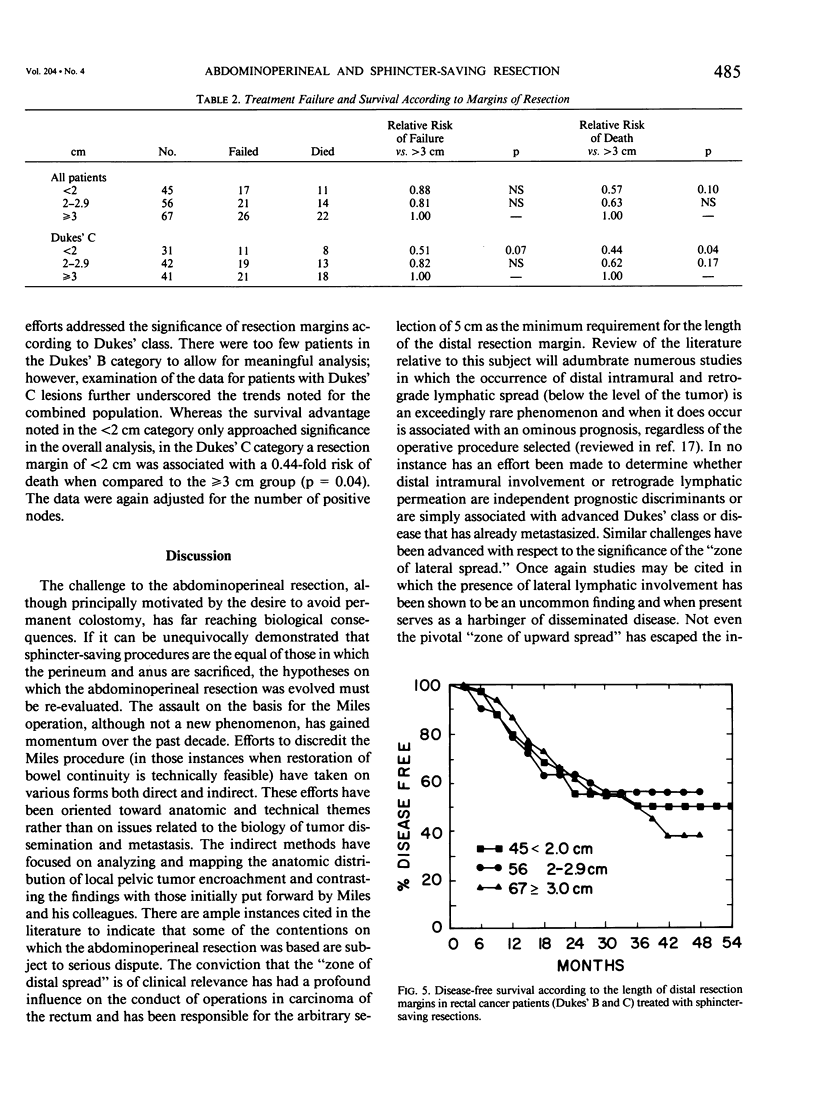
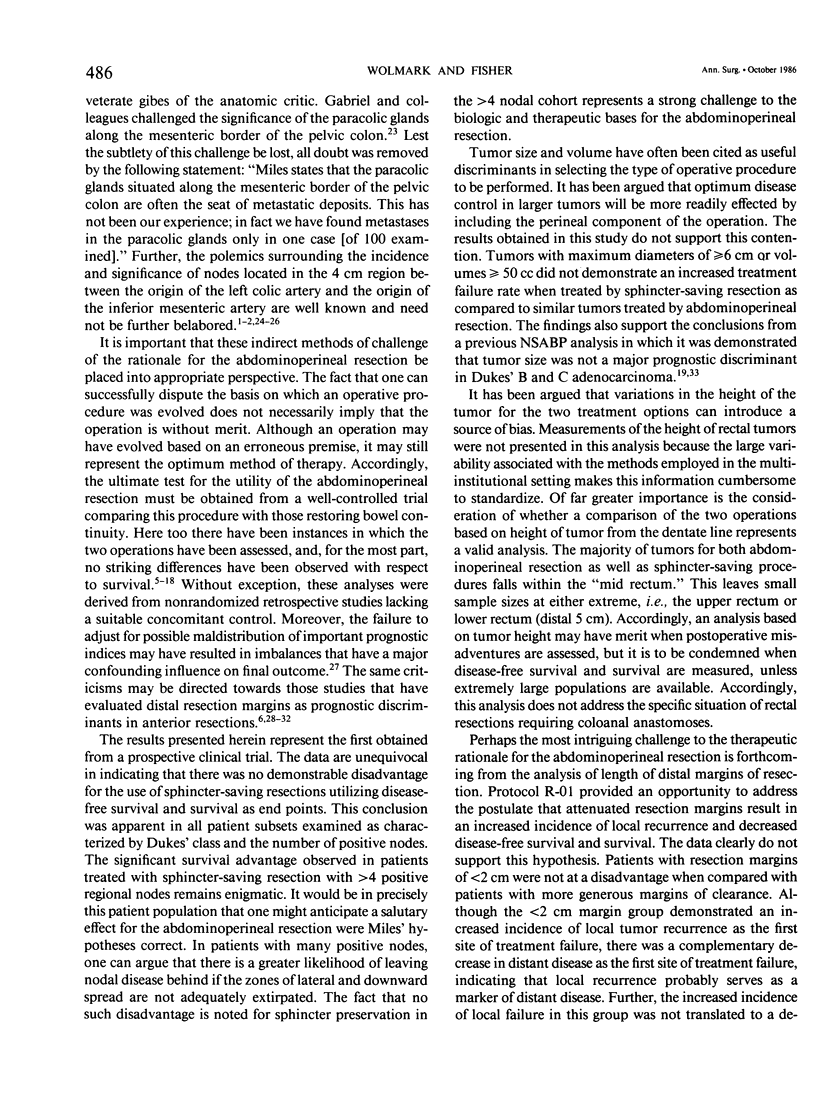
Abdominoperineal resections for rectal carcinoma are being performed with decreasing frequency in favor of sphincter-saving resections. It remains, however, to be unequivocally demonstrated that sphincter preservation has not resulted in compromised local disease control, disease-free survival, and survival. Accordingly, it is the specific aim of this endeavor to compare local recurrence, disease-free survival, and survival in patients with Dukes' B and C rectal cancer undergoing curative abdominoperineal resection or sphincter-saving resection. For the purpose of this study, 232 patients undergoing abdominoperineal resection and 181 subjected to sphincter-saving resections were available for analysis from an NSABP randomized prospective clinical trial designed to ascertain the efficacy of adjuvant therapy in rectal carcinoma (protocol R-01). The mean time on study was 48 months. Analyses were carried out comparing the two operations according to Dukes' class, the number of positive nodes, and tumor size. The only significant differences in disease-free survival and survival were observed for the cohort characterized by greater than 4 positive nodes and were in favor of patients treated with sphincter-saving resections. A patient undergoing sphincter-saving resection was 0.62 times as likely to sustain a treatment failure as a similar patient undergoing abdominoperineal resection (p = 0.07) and 0.49 times as likely to die (p = 0.02). The inability to demonstrate an attenuated disease-free survival and survival for patients treated with sphincter-saving resection was in spite of an increased incidence of local recurrence (anastomotic and pelvic) observed for the latter operation when compared to abdominoperineal resection (13% vs. 5%). A similar analysis evaluating the length of margins of resection in patients undergoing sphincter-preserving operations indicated that treatment failure and survival were not significantly different in patients whose distal resection margins were less than 2 cm, 2-2.9 cm, or greater than or equal to 3 cm. If any trend was observed, it appeared that patients with smaller resection margins had a slightly prolonged survival (p = 0.10). This observation was present in spite of the fact that local recurrence as a first site of treatment failure was greater in the group with less than 2 cm that it was in the greater than or equal to 3 cm category, 22% versus 12%. This increased local recurrence rate in the population with smaller margins was not translated into an in crease in overall treatment failure and had absolutely no influence on survival. It is suggested that local recurrence serves as a marker of distant disease.(ABSTRACT TRUNCATED AT 400 WORDS)
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Copeland E. M., Miller L. D., Jones R. S. Prognostic factors in carcinoma of the colon and rectum. Am J Surg. 1968 Dec;116(6):875–881. doi: 10.1016/0002-9610(68)90458-3. [DOI] [PubMed] [Google Scholar]
- DEDDISH M. R., STEARNS M. W., Jr Anterior resection for carcinoma of the rectum and rectosigmoid area. Ann Surg. 1961 Dec;154:961–966. [PMC free article] [PubMed] [Google Scholar]
- Dixon C. F. Anterior Resection for Malignant Lesions of the Upper Part of the Rectum and Lower Part of the Sigmoid. Ann Surg. 1948 Sep;128(3):425–442. doi: 10.1097/00000658-194809000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GOLIGHER J. C. The blood-supply to the sigmoid colon and rectum with reference to the technique of rectal resection with restoration of continuity. Br J Surg. 1949 Oct;37(146):157–162. doi: 10.1002/bjs.18003714604. [DOI] [PubMed] [Google Scholar]
- GRINNELL R. S. RESULTS OF LIGATION OF INFERIOR MESENTERIC ARTERY AT THE AORTA IN RESECTIONS OF CARCINOMA OF THE DESCENDING AND SIGMOID COLON AND RECTUM. Surg Gynecol Obstet. 1965 May;120:1031–1036. [PubMed] [Google Scholar]
- Jones P. F., Thomson H. J. Long term results of a consistent policy of sphincter preservation in the treatment of carcinoma of the rectum. Br J Surg. 1982 Oct;69(10):564–568. doi: 10.1002/bjs.1800691003. [DOI] [PubMed] [Google Scholar]
- MAYO C. W., LABERGE M. Y., HARDY W. M. Five year survival after anterior resection for carcinoma of the rectum and rectosigmoid. Surg Gynecol Obstet. 1958 Jun;106(6):695–698. [PubMed] [Google Scholar]
- Manson P. N., Corman M. L., Coller J. A., Veidenheimer M. C. Anterior resection for adenocarcinoma. Lahey Clinic experience from 1963 through 1969. Am J Surg. 1976 Apr;131(4):434–441. doi: 10.1016/0002-9610(76)90153-7. [DOI] [PubMed] [Google Scholar]
- McDermott F., Hughes E., Pihl E., Milne B. J., Price A. Long term results of restorative resection and total excision for carcinoma of the middle third of the rectum. Surg Gynecol Obstet. 1982 Jun;154(6):833–837. [PubMed] [Google Scholar]
- Nicholls R. J., Ritchie J. K., Wadsworth J., Parks A. G. Total excision or restorative resection for carcinoma of the middle third of the rectum. Br J Surg. 1979 Sep;66(9):625–627. doi: 10.1002/bjs.1800660908. [DOI] [PubMed] [Google Scholar]
- Patel S. C., Tovee E. B., Langer B. Twenty-five years of experience with radical surgical treatment of carcinoma of the extraperitoneal rectum. Surgery. 1977 Oct;82(4):460–465. [PubMed] [Google Scholar]
- Pollett W. G., Nicholls R. J. The relationship between the extent of distal clearance and survival and local recurrence rates after curative anterior resection for carcinoma of the rectum. Ann Surg. 1983 Aug;198(2):159–163. doi: 10.1097/00000658-198308000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slanetz C. A., Jr, Herter F. P., Grinnell R. S. Anterior resection versus abdominoperineal resection for cancer of the rectum and rectosigmoid. An analysis of 524 cases. Am J Surg. 1972 Jan;123(1):110–117. doi: 10.1016/0002-9610(72)90318-2. [DOI] [PubMed] [Google Scholar]
- Stearns M. W., Jr The choice among anterior resection, the pull-through, and abdominoperineal resection of the rectum. Cancer. 1974 Sep;34(3):suppl–suppl:971. doi: 10.1002/1097-0142(197409)34:3+<969::aid-cncr2820340728>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- Strauss R. J., Friedman M., Platt N., Wise L. Surgical treatment of rectal carcinoma: results of anterior resection vs. abdominoperineal resection at a community hospital. Dis Colon Rectum. 1978 May-Jun;21(4):269–276. doi: 10.1007/BF02586702. [DOI] [PubMed] [Google Scholar]
- Williams N. S., Dixon M. F., Johnston D. Reappraisal of the 5 centimetre rule of distal excision for carcinoma of the rectum: a study of distal intramural spread and of patients' survival. Br J Surg. 1983 Mar;70(3):150–154. doi: 10.1002/bjs.1800700305. [DOI] [PubMed] [Google Scholar]
- Williams N. S., Durdey P., Johnston D. The outcome following sphincter-saving resection and abdominoperineal resection for low rectal cancer. Br J Surg. 1985 Aug;72(8):595–598. doi: 10.1002/bjs.1800720804. [DOI] [PubMed] [Google Scholar]
- Williams N. S., Johnston D. Survival and recurrence after sphincter saving resection and abdominoperineal resection for carcinoma of the middle third of the rectum. Br J Surg. 1984 Apr;71(4):278–282. doi: 10.1002/bjs.1800710409. [DOI] [PubMed] [Google Scholar]
- Williams N. S. The rationale for preservation of the anal sphincter in patients with low rectal cancer. Br J Surg. 1984 Aug;71(8):575–581. doi: 10.1002/bjs.1800710802. [DOI] [PubMed] [Google Scholar]
- Wilson S. M., Beahrs O. H. The curative treatment of carcinoma of the sigmoid, rectosigmoid, and rectum. Ann Surg. 1976 May;183(5):556–565. doi: 10.1097/00000658-197605000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolmark N., Cruz I., Redmond C. K., Fisher B., Fisher E. R. Tumor size and regional lymph node metastasis in colorectal cancer. A preliminary analysis from the NSABP clinical trials. Cancer. 1983 Apr 1;51(7):1315–1322. doi: 10.1002/1097-0142(19830401)51:7<1315::aid-cncr2820510723>3.0.co;2-0. [DOI] [PubMed] [Google Scholar]
- Wolmark N., Fisher B., Wieand H. S. The prognostic value of the modifications of the Dukes' C class of colorectal cancer. An analysis of the NSABP clinical trials. Ann Surg. 1986 Feb;203(2):115–122. doi: 10.1097/00000658-198602000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolmark N., Fisher E. R., Wieand H. S., Fisher B. The relationship of depth of penetration and tumor size to the number of positive nodes in Dukes C colorectal cancer. Cancer. 1984 Jun 15;53(12):2707–2712. doi: 10.1002/1097-0142(19840615)53:12<2707::aid-cncr2820531225>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- Wolmark N., Gordon P. H., Fisher B., Weiand S., Lerner H., Lawrence W., Shibata H. A comparison of stapled and handsewn anastomoses in patients undergoing resection for Dukes' B and C colorectal cancer. An analysis of disease-free survival and survival from the NSABP prospective clinical trials. Dis Colon Rectum. 1986 May;29(5):344–350. doi: 10.1007/BF02554128. [DOI] [PubMed] [Google Scholar]
- Zollinger R. M., Sheppard M. H. Carcinoma of the rectum and the rectosigmoid. A review of 729 cases. Arch Surg. 1971 Apr;102(4):335–338. doi: 10.1001/archsurg.1971.01350040097019. [DOI] [PubMed] [Google Scholar]