

Abstract
Rhabdomyosarcoma (RMS) comprises approximately 5% of all pediatric malignancies, and the biliary system is considered one of the rarest RMS locations. Awareness, knowledge, and early recognition of the disease are essential for accurate diagnosis and proper treatment of biliary RMS in a child with obstructive jaundice and suspicious radiological findings. We present two pediatric biliary RMS cases requiring different managements because of their primary evaluations at their referring facilities. A four-and-a-half-year-old boy was referred to our institution for liver transplantation following neoadjuvant chemotherapy for centrally located unresectable biliary RMS. The patient received a left lateral segment graft from a living donor with no complications during the post-transplant period. The second patient was a seven-year-old foreign boy with obstructive jaundice and a history of choledochal cyst resection. A tumoral mass was revealed during exploration, and macroscopic total resection of the lesion was performed. The final pathology result of the resected material was biliary RMS with microscopic residue on the bile duct margin and lymph node involvement. The patient was transferred to the Pediatric Oncology Division for systemic treatment following surgical recovery. Biliary RMS presents distinct challenges in terms of accurate diagnosis and successful management. A multidisciplinary approach is indispensable for effective treatment. Complete surgical resection has been proven to be the mainstay strategy in feasible cases. Contributions of pre- and postoperative chemotherapy and radiotherapy are crucial in extensive disease. Liver transplantation should be considered, with reasonable success rates, in persistent unresectable and non-metastatic cases.
Keywords: Biliary rhabdomyosarcoma, children, liver transplantation
Introduction
The liver and biliary tract are considered very rare locations, comprising 0.5–1.5% of RMS cases. Several combinations of chemotherapy, surgery, and radiotherapy have been practiced for the treatment of biliary RMS; nevertheless, there has been no common global treatment protocol. Survival rates have been reported at approximately 50–85% at the 5-year period, depending on disease stage and histologic subtype.[1–3]
Unfortunately, 30–40% of cases present with metastatic disease at the time of biliary RMS identification due to preliminary misdiagnosis. Initial symptoms and findings—including obstructive jaundice with a suspicious liver/biliary system lesion containing cystic components—require careful workup.[3]
Here, we present two pediatric biliary RMS cases who underwent definitive surgeries at Inonu University Liver Transplantation Institute, requiring different managements because of their primary evaluations at their referring facilities.
Patients and Methods
The hospital records of two patients who were diagnosed with biliary RMS were evaluated retrospectively. This study was approved by the Institutional Review Board of Inonu University (approval no. 2025/8227).
Case Reports
Case 1 – A four-and-a-half-year-old boy with biliary RMS was referred to our institution for liver transplantation (LTx). He had initially presented to a university hospital with abdominal pain, pruritus, and diarrhea at the age of three years. Laboratory results were consistent with obstructive jaundice, and imaging studies showed a centrally located liver mass. Embryonal RMS was diagnosed following liver biopsy, and the patient received 13 cycles of chemotherapy. Control imaging showed an unresectable lesion (Fig. 1), and the patient underwent LTx as part of the first 7-way liver paired exchange (LPE) LTx in the world, 17 months after RMS diagnosis. The post-transplant period was uncomplicated, and the patient was discharged on day 18. Pathological examination of the explanted liver and surrounding lymph nodes revealed 10–15% viable periductular tumor. No recurrence has been reported according to imaging studies, with a well-functioning allograft at one year post-transplant.
Figure 1.

The MRI images of centrally located unresectable biliary RMS prior to and after the neoadjuvant chemotherapy.
Case 2 – A seven-year-old foreign boy was referred to our institution with obstructive jaundice. According to limited information obtained from his family, he had undergone surgery in his country because of jaundice and bile duct strictures. The family affirmed that he had some relief for two months, but he had been suffering from severe icterus and itching for the last month. He was transferred to Turkiye. MRI and MRCP images were evaluated as changes secondary to strictured hepatico-jejunostomy anastomosis (Fig. 2). Biliary catheters were placed after dilatation of the anastomosis, and a biopsy was taken from a suspicious lesion. True-cut biopsy revealed no tumor but obstructive-type cholestasis, and hepatico-jejunostomy revision was planned.
Figure 2.
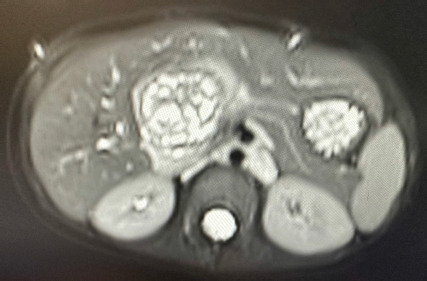
The MRI image of the lesion with cystic and solid components.
Surgical exploration revealed suspicion of a bile duct tumor. The hepatico-jejunostomy line was totally embedded in a tumoral mass with cystic and solid components. Frozen biopsy was consistent with a sarcomal tumor. The common bile duct was totally resected, and biliary ducts were closed distally. The initial frozen pathology result was reported as RMS.
Postoperatively, bile leak was prominent from the repair area surrounding the bile ducts. A second operation was necessary to control the bile leak, and total resection of the tumor was macroscopically achieved with extended right hepatectomy during that surgery (Fig. 3). Bile duct margins were microscopically positive for botryoid-type biliary RMS, and metastatic lymph nodes were present in the final pathology report. The postoperative period was uncomplicated, and the patient was discharged on day 15 and referred to the Pediatric Oncology Division. There were no surgery-related complications, and the patient has been receiving systemic chemotherapy for the last six months.
Figure 3.

The picture of the extended right hepatectomy material.
Discussion
Rhabdomyosarcoma comprises approximately 5% of all pediatric malignancies, and the biliary system is one of the rarest locations. Biliary RMS presents distinct challenges in terms of accurate diagnosis and successful management. According to the literature, biliary tract RMS is typically a disease of early childhood and is most often diagnosed around 3 years of age, with boys showing a higher prevalence.[3,4] Both of our cases were boys diagnosed at approximately 4 and 7 years of age.
Patient age >10 years, alveolar histology, initial tumor size >5 cm, lymph node involvement, and distant metastasis have been reported as unfavorable features.[3–7] Reports have been controversial regarding whether the biliary system represents a favorable origin. Recent studies have drawn attention to reconsidering biliary origin as unfavorable or intermediate risk, in light of low survival and high mortality rates, especially when relapse occurs.[1,4,7–9]
We performed extended surgeries for both patients with the aim of total resection. Extended surgery in biliary RMS has been reported as ineffective in some trials.[4–6] However, if we consider the success rates of surgical resections in those studies as below standard, more acceptable outcomes in reports from Guerin et al.[1] and Fuchs et al.[7] may be more reasonable to acknowledge in the current era. We believe the importance of surgical approach is crucial in biliary RMS treatment if complete resection is feasible.
There have been reports of total remission following neoadjuvant chemotherapy. Conversely, treatment without surgery has been shown as an independent risk factor for mortality, with survival dropping to 0–17% in cases of recurrence. Some studies have presented better 5-year patient survival with extended surgical approaches compared to limited surgery. Similarly, tumor-free surgical margins have been achieved at higher rates in patients undergoing extended resection following neoadjuvant chemotherapy.[1,2,7–10]
The decision for transplantation or surgical resection in our patients was based on the possibility of total resection of the tumoral masses. Unresectable biliary RMS following neoadjuvant chemotherapy without metastasis compelled us to conclude with LTx for the first patient, mainly due to the tumor’s central location. Although transplantation may be regarded as an aggressive treatment for a chemo-responsive tumor like RMS, successful reports exist of LTx for unresectable biliary RMS with no distant metastasis following neoadjuvant chemotherapy. Remarkably, most failed transplantations in the literature involved recurrent cases with extensive extrahepatic invasion, resulting in incomplete tumor resection during hepatectomy. Unfortunately, indications for resection versus LTx have not been well defined worldwide.[2,3,7]
In the second case, hepatico-jejunostomy revision was planned under conditions of uncontrolled obstructive jaundice and deteriorating liver function. Intraoperative findings were suspicious for a biliary tumor with parenchymal invasion at the previous operation site. Frozen pathology revealed a sarcoma within the resected common bile duct. Following limited resection, bile leak from fragile tissue around the resection site necessitated a second surgery to control the leak. Chemotherapy was considered too risky due to the prominent leak. Extended right hepatectomy achieved macroscopic complete resection, but final pathology revealed microscopic tumor residue at the reconstruction site with metastatic lymph nodes. Probably, the primary complete resection might have been achievable following a proper neoadjuvant chemotherapy administration in this patient. Unfortunately, absence of early imaging, operative, and pathology data, as well as distorted lesion depiction due to prior surgery and inflammation, misled the diagnosis and resulted in an additional surgical step, eliminating the chance for neoadjuvant chemotherapy before the second surgery.
Struggles in establishing the correct diagnosis have been repeatedly reported as one of the critical pitfalls in biliary RMS management.[1–5,7,8] Obstructive jaundice is a common symptom in several pathologies, including cholangitis, choledocholithiasis, choledochal malformations, pancreatic malformations, and tumors. Moreover, the radiological appearance of non-invasive biliary RMS may resemble a congenital choledochal cyst. MRCP and biopsy are especially used to differentiate obstructive benign strictures or cystic lesions from intraluminal neoplasms, but they were not beneficial in our case.[4-8]
According to the current literature, complete surgical resection remains critical whenever feasible, to minimize recurrence and mortality. However, primary total resection is not often possible due to the tumor’s common location at the portal triad, necessitating chemotherapy and radiotherapy as adjunctive therapies. Neoadjuvant chemotherapy can enable tumor shrinkage to make unresectable lesions resectable, and adjuvant chemotherapy and/or radiotherapy for residual disease highlight the importance of a multimodal treatment approach to achieve tumor-free survival.[1-3,7–10]
Conclusion
Awareness, knowledge, and early recognition of the disease are essential for accurate diagnosis and proper treatment of biliary RMS in a child presenting with obstructive jaundice and suspicious radiological findings of the liver and biliary system. A multidisciplinary approach is indispensable in disease management. Complete surgical resection has been proven to be the mainstay strategy in feasible cases. Contributions of pre- and postoperative chemotherapy and/or radiotherapy are crucial in extensive disease. LTx should be considered, with reasonable success rates, in unresectable and non-metastatic cases.
Footnotes
How to cite this article: Celik N, Karakas S, Koc C, Akatli AN, Yilmaz S. Surgical management of pediatric biliary rhabdomyosarcoma: Importance of differential diagnosis. Hepatology Forum 2025; 6(4):176–179.
Ethics Committee Approval
This study was approved by the Institutional Review Board of Inonu University with approval (date: 12.08.2025, number: 2025/8227).
Informed Consent
Written informed consent was obtained from participants.
Conflict of Interest
The authors have no conflict of interest to declare.
Financial Disclosure
The authors declared that this study has received no financial support.
Use of AI for Writing Assistance
Not declared.
Author Contributions
Concept – NC, SK, CK, ANA, SY; Design – NC, SK, CK, ANA, SY; Supervision – NC, SK, CK, ANA, SY; Data Collection and/or Processing – NC; Analysis and/or Interpretation – NC; Literature Search – NC; Writing – NC; Critical Reviews – NC, SY.
Peer-review
Externally peer-reviewed.
References
- 1.Guérin F, Rogers T, Minard-Colin V, Gaze MN, Terwisscha S, Van Noesel M, et al. Outcome of localized liver-bile duct rhabdomyosarcoma according to local therapy: a report from the European Paediatric Soft-Tissue Sarcoma Study Group (EpSSG)-RMS 2005 study. Pediatr Blood Cancer. 2019;66(7):e27725. doi: 10.1002/pbc.27725. [DOI] [PubMed] [Google Scholar]
- 2.Jung-Man N, Shin H, Gil-Chun P, Hyunhee K, Suhyeon H, Seak HO, et al. Pediatric living donor liver transplantation for biliary embryonal rhabdomyosarcoma: a case report of a case showing disease-free survival over 2 years. Korean J Transplant. 2022;36:148–153. doi: 10.4285/kjt.21.0008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Swieszkowska E, Broniszczak D, Kalicinski P, Szymczak M, Stefanowicz M, Grajkowska W, et al. Rhabdomyosarcoma of the biliary tract in children: analysis of single center experience. Cancers. 2024;16:3110. doi: 10.3390/cancers16173110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Aye JM, Xue W, Palmer JD, Walterhouse DO, Arnold MA, Heaton TE, et al. Suboptimal outcome for patients with biliary rhabdomyosarcoma treated on low-risk clinical trials: a report from the Children’s Oncology Group. Pediatr Blood Cancer. 2021;68(4):e28914. doi: 10.1002/pbc.28914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Spunt SL, Lobe TE, Pappo AS, Parham DM, Wharam MD, Arndt C, Jr, et al. Aggressive surgery is unwarranted for biliary tract rhabdomyosarcoma. J Pediatr Surg. 2000;35(2):309–316. doi: 10.1016/S0022-3468(00)90030-7. [DOI] [PubMed] [Google Scholar]
- 6.Spunt SL. Patients with nonmetastatic embryonal rhabdomyosarcoma arising in the biliary tract should be treated on low-risk clinical trials. Pediatr Blood Cancer. 2022;69(1):e29399. doi: 10.1002/pbc.29399. [DOI] [PubMed] [Google Scholar]
- 7.Fuchs J, Murtha-Lemekhova A, Kessler M, Günther P, Fichtner A, Pfeiffenberger J, et al. Biliary rhabdomyosarcoma in pediatric patients: a systematic review and meta-analysis of individual patient data. Front Oncol. 2021;11:701400. doi: 10.3389/fonc.2021.701400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Urla C, Warmann SW, Sparber-Sauer M, Schuck A, Leuschner I, Klingebiel T, et al. Treatment and outcome of the patients with rhabdomyosarcoma of the biliary tree: experience of the Cooperative Weichteilsarkom Studiengruppe (CWS) BMC Cancer. 2019;19:945. doi: 10.1186/s12885-019-6172-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Aye JM, Venkatramani R. Comment on: Patients with nonmetastatic embryonal rhabdomyosarcoma arising in the biliary tract should be treated on low-risk clinical trials. Pediatr Blood Cancer. 2022;69(7):e29554. doi: 10.1002/pbc.29554. [DOI] [PubMed] [Google Scholar]
- 10.Cecchetto G, Bisogno G, Treuner J, Ferrari A, Mattke A, Casanova M, et al. Role of surgery for nonmetastatic abdominal rhabdomyosarcomas: a report from the Italian and German Soft Tissue Cooperative Groups Studies. Cancer. 2003;97:1974–1980. doi: 10.1002/cncr.11285. [DOI] [PubMed] [Google Scholar]