

Abstract
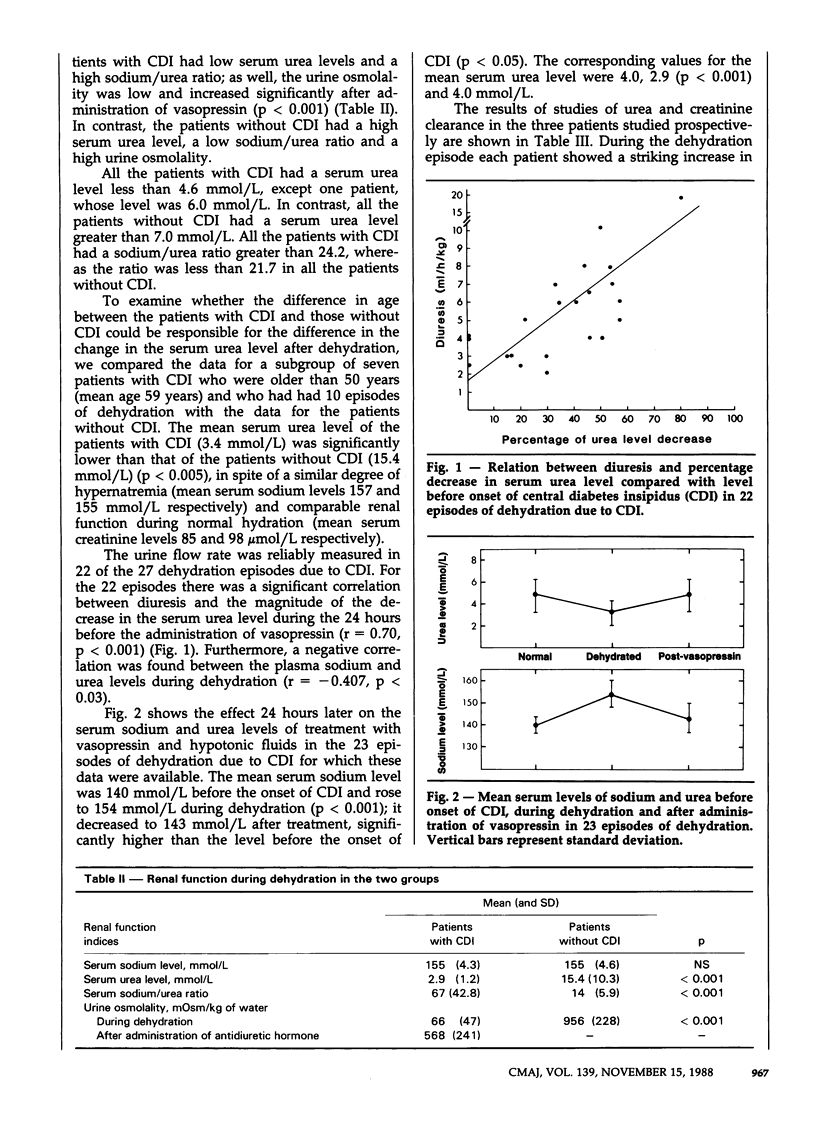
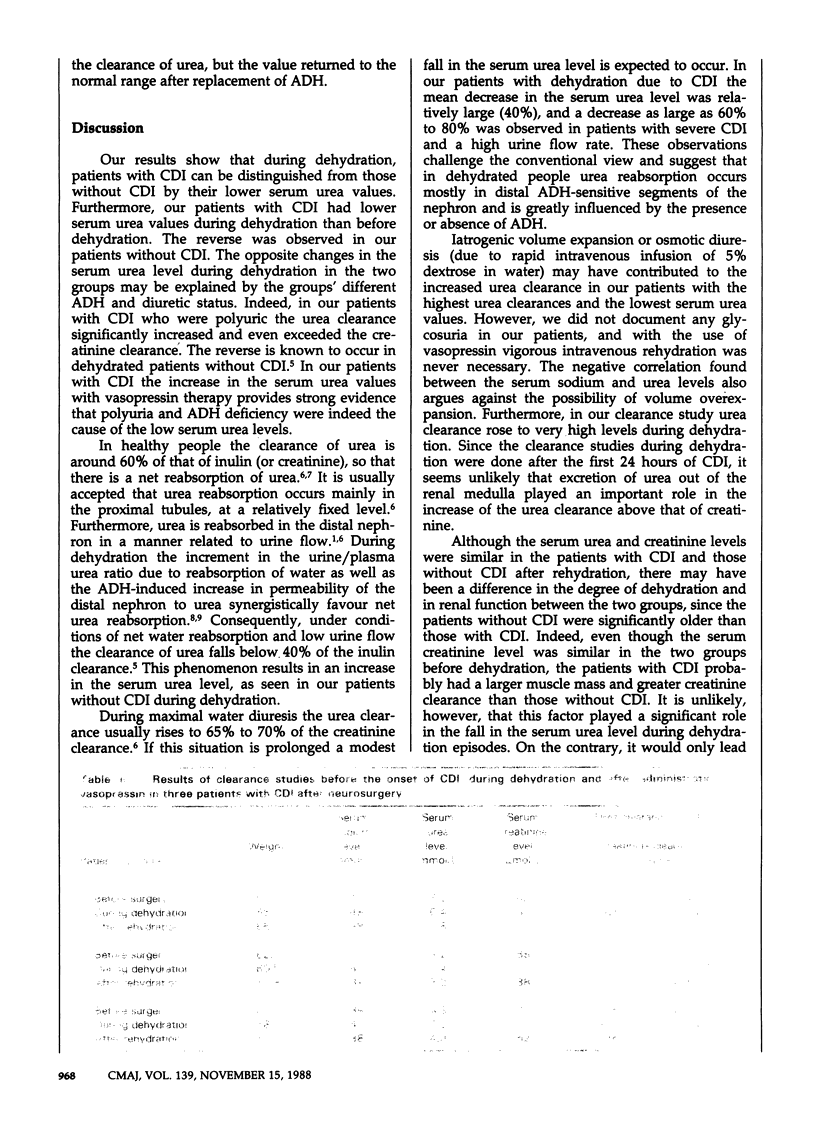
Dehydrated patients usually present with an elevated serum urea level, owing in part to increased renal reabsorption of urea mediated by antidiuretic hormone (ADH). We carried out a study to examine whether, during dehydration, the variations in the serum urea level could discriminate patients with central diabetes insipidus (CDI) from those with dehydration not due to CDI. We studied retrospectively 27 episodes of dehydration in 23 patients with CDI and 14 episodes in 14 patients without CDI. The mean serum urea level was 2.9 mmol/L in the CDI group and 15.4 mmol/L in the patients without CDI (p less than 0.001); the mean serum sodium level was 155 mmol/L in both groups. All the patients with CDI had a sodium/urea ratio greater than 24.2, whereas the ratio was less than 21.7 in all the patients without CDI. In the patients with CDI a positive correlation was found between the magnitude of diuresis and the percentage decrease in the serum urea level compared with the level before dehydration (p less than 0.001). In the patients with CDI the serum urea level returned to the level before dehydration after the administration of vasopressin; a striking increase in the clearance of urea, which exceeded the creatinine clearance, was observed during dehydration in the three patients in whom clearance studies were done. The results suggest that serum urea values can be used to distinguish patients dehydrated because of CDI from those with hypertonic dehydration but without ADH deficiency and that during dehydration the net reabsorption of urea is dependent on the renal action of ADH.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Chasis H., Smith H. W. THE EXCRETION OF UREA IN NORMAL MAN AND IN SUBJECTS WITH GLOMERULONEPHRITIS. J Clin Invest. 1938 May;17(3):347–358. doi: 10.1172/JCI100959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldstein M. H., Lenz P. R., Levitt M. F. Effect of urine flow rate on urea reabsorption in man: urea as a "tubular marker". J Appl Physiol. 1969 May;26(5):594–599. doi: 10.1152/jappl.1969.26.5.594. [DOI] [PubMed] [Google Scholar]
- LASSITER W. E., GOTTSCHALK C. W., MYLLE M. Micropuncture study of net transtubular movement of water and urea in nondiuretic mammalian kidney. Am J Physiol. 1961 Jun;200:1139–1147. doi: 10.1152/ajplegacy.1961.200.6.1139. [DOI] [PubMed] [Google Scholar]
- Miller M., Dalakos T., Moses A. M., Fellerman H., Streeten D. H. Recognition of partial defects in antidiuretic hormone secretion. Ann Intern Med. 1970 Nov;73(5):721–729. doi: 10.7326/0003-4819-73-5-721. [DOI] [PubMed] [Google Scholar]
- Rocha A. S., Kudo L. H. Water, urea, sodium, chloride, and potassium transport in the in vitro isolated perfused papillary collecting duct. Kidney Int. 1982 Nov;22(5):485–491. doi: 10.1038/ki.1982.201. [DOI] [PubMed] [Google Scholar]
- SCHIMKE R. T. Studies on factors affecting the levels of urea cycle enzymes in rat liver. J Biol Chem. 1963 Mar;238:1012–1018. [PubMed] [Google Scholar]
- Valtonen M. H., Uusi-Rauva A., Eriksson L. The effect of protein deprivation on the validity of creatinine and urea in evaluation of renal function. An experimental study in the goat. Scand J Clin Lab Invest. 1982 Oct;42(6):507–512. [PubMed] [Google Scholar]
- Wolf A. V., Pillay V. K. Renal concentration tests; osmotic pressure, specific gravity, refraction and electrical conductivity compared. Am J Med. 1969 Jun;46(6):837–843. doi: 10.1016/0002-9343(69)90085-0. [DOI] [PubMed] [Google Scholar]