

Abstract
This review examines how a “bottom-up” model of a civilian technology program works by recounting the story of the “genesis” of the Information Infrastructure for Healthcare (IIH) focused program of the Advanced Technology Program. The IIH program began with an exchange of ideas among members of the private and public sectors (through the submission of “white papers” by members of industry, workshops conducted by the ATP, and meetings among persons from both groups) to identify the technologies that are necessary for the development of a national information infrastructure in health care. What the ATP hoped to gain through this process and how the private sector responded are noted. A statistical description of the participants and a discussion of changes in the ATP review and selection process is included.
The Advanced Technology Program (ATP) at the National Institute of Standards and Technology (NIST) is a cost-sharing program designed to partner the federal government with the private sector to further both the development and the dissemination of high-risk technologies that have the potential to provide significant, broad-based economic benefits for the nation.*,† In this program, industry proposes research projects to the ATP to be judged in competitions for funding based on both the technical and the economic and business merits of the proposal.
From 1990 through 1998, the ATP held “general” competitions each year, open to all technologies. From 1994 through 1998, the ATP awarded most of its funding through “focused-program”‡ competitions, in which a suite of projects was funded to mobilize technology to address a particular problem. Thirty focused program competitions were held, each with a unifying set of project goals. This is the story of one program, the Information Infrastructure for Healthcare (IIH) focused program.
The IIH focused program was initiated in 1994 amid nationwide discussion of the rising costs of health care and the quality of that care. The objective of the program was to develop the information infrastructure technologies that are needed 1) to cut dramatically the 20 percent of the $1 trillion health care cost that is spent on paperwork and 2) to improve the quality and flexible delivery of care by faster broad access to better information.
ATP awards for research made possible new technologic capabilities in firms, allowing them to introduce advanced functionalities into their existing IIH products as well as develop new products. These awards enabled the smallest firms to extend their limited resources and overcome research barriers that impeded the attraction of private venture capital funding. It encouraged large companies to pursue enabling, high-risk research and development despite tight discretionary budgets.
The ATP and Focused Programs
Focused programs were introduced to the ATP during a period of program budgetary increases, which allowed for targeted opportunities for funding as well as a general competition to be held each year for those proposals outside the scope of announced focused areas. Between the end of 1993 and the beginning of 1994, a total of 920 “white papers”§ covering a range of technologies were submitted and sorted by a technology taxonomy. Of these papers, approximately two dozen addressed health care issues, providing both scope and technical detail.
Papers were submitted by companies, individuals with companies, associations of companies, university professors, members of other organizations, and private citizens without organizational affiliation. Some were submitted by large consortia offering a comprehensive road map for the ATP in developing a partnership with industry. The white paper process provided an opportunity for people to share their ideas and for the ATP to define more clearly the goals of the focused program. The white papers submitted to the ATP address a set of published criteria; namely, technical ideas, economic benefit, industry commitment, and the need for ATP funding.
Following the receipt of the first batch of white papers, the program manager for the IIH focused program organized a public workshop attended by representatives from industry and from the nonprofit and academic communities. Its purpose was to refine the many ideas identified in the white papers into a focused program.5–7 At the conclusion of the workshop a consensus developed, identifying infrastructural information technologies as offering the best means to achieve a significant reduction in health care costs while increasing quality of care. Information technologies for health care also offered one of the most clearly defined areas of technologic development requiring the public–private partnership offered by the ATP. The role of the ATP was thus defined as one of fostering cooperation and communication and serving as the catalyst to bring together the members of the information technology and medical communities to achieve the objectives.
The dialogue begun at the workshop was sustained through the solicitation of additional white papers, both formal and informal, and through multiple small group discussions.¶ The new white papers and additional interactions complemented the discussions held at the workshop, identifying the increased demands placed on the U.S. health care industry to raise the quality of service, to extend consistent quality in rural and urban areas, to provide accurate measures of success, and to accomplish all these with lower costs in a timely fashion while establishing national standards for the electronic transfer of patient records and related medical documents.
Specific technologies identified in the white papers included, but were not limited to, development of:
Information tools to automate, validate and distribute clinical practice guidelines for mass use. These could include clinical practice guidelines that capture the current “best practices” for a variety of medical situations.
Tools to enable health care providers and quality/cost monitors to browse and extract data automatically from a multitude of scattered clinical and administrative databases, without requiring changes to the existing databases.
Tools that facilitate the production of clinical notes and, as a by-product, gather the codified clinical data and store it in a database system.
An interoperable open-systems architecture to serve as an interface between independent health care information systems.
This input gave impetus to the final scope of the proposed focused program in the development of information infrastructure. As defined here, information infrastructure development includes the integration, synthesis, and definition of any information that needs to be shared across the enterprise and the development of the means by which to transport, store, and access that information in a way that enhances, rather than impedes, user productivity.
Information Infrastructure for Health Care Focused Program
The IIH focused program solicitation kit5 identified the program's goals. Technical goals were to establish the technologies for:
Reliable storage and retrieval of complex medical information for varied applications
Real-time, data-driven medical decisions
Real-time data entry by mobile medical personnel
Real-time global transport of complex medical records with accuracy, speed, and security
Computer-based medical training, diagnostic, and reference tools
Business goals were to gain the capability to develop products that will:
Reduce unit health care costs
Improve quality of health care (higher treatment success rates and avoidance of complications)
Capture global market share of new and improved products and services
Undertake infrastructural development focusing on “tools” and prototype systems to enhance the flow of information between existing “legacy” systems in the health care enterprise while being scalable from a single provider's office to a fully integrated health care system.
A model of the program, which would result in a portfolio of required technologies, is shown in Figure 1▶. The “pyramid” consists of three categories, which should be read from bottom to top: 1) infrastructure development technologies (e.g., tools for enterprise integration and business process modeling), 2) user interface and efficiency-enhanced technologies (e.g., hypermedia human interfaces, natural language processing, data retrieval, and advanced search mechanisms), and 3) health-care-specific technologies (e.g., clinical decision support systems, consumer health information systems, and education systems).5
Figure 1.
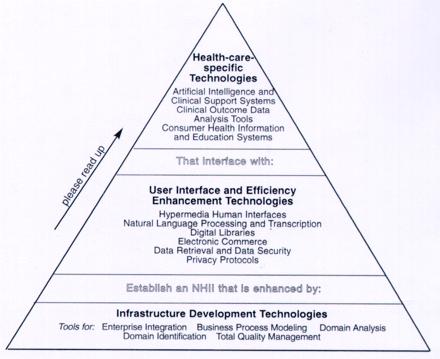
Model of the focused program. The model should be read from bottom to top. NHII indicates National Healthcare Information Infrastructure.
Each level of the model is presented as being distinct from the next, with the idea that development of those technologies on the lower levels should precede development of those above, resulting in a “bottom-up” approach. This logic influenced the announcement of the first and second solicitations, whereby only those projects in which the high-risk technology development “fit” in the respective level were to be funded. It was recognized, of course, that the overlap between levels is considerable and that, therefore, components from more than one level may be proposed in any given project.
Before the announcement of the third solicitation, it was recognized that technologic research and development in this industry requires additional and simultaneous development of “infrastructural” technologies along with those “higher” on the pyramid. In 1997, therefore, the third solicitation sought proposals that focused on the lower two levels of the pyramid but addressed all technologies in all levels.
IIH Focused Program Awardees
Table 1▶ summarizes statistical data from the three IIH solicitations held between 1994 and 1997. In response to these solicitations, 221 proposals were received and 32 awards were made to 79 participants. Research and development funding totaled $295 million, representing a commitment of $146 million from the government and $149 million from the private sector.
Table 1.
IIH Focused Program Participation
| 1994 | 1995 | 1997 | |
|---|---|---|---|
| Total proposals submitted | 59 | 68 | 94 |
| Total projects funded | 16 | 10 | 6 |
| Type of award participant: | |||
| Single applicant | 10 | 7 | 6 |
| Joint venture | 6 | 3 | |
| Total participants | 43 | 32 | 6 |
| Type/size of organization: | |||
| For-profit small company | 17 | 12 | 6 |
| For-profit medium company | 6 | 4 | |
| For-profit large company | 6 | 5 | |
| Nonprofit organization | 7 | 8 | |
| University | 4 | 3 |
Note: The statistical data are from the Business Reporting System (BRS) database maintained by the ATP Economic Assessment Office. Begun in 1994, the BRS provides a comprehensive data tool used for tracking on a routine and regular basis and for measuring the progress of projects against business plans and projected economic benefits, as outlined in the project proposals and updated over the course of the projects.
What remains relatively constant across the three solicitations is a dominant role of small for-profit companies. These companies participated both as single applicants and as members of joint ventures. Single applicant award recipients included start-ups as well as research organizations in medium and large companies. The joint ventures consisted of several types of organizations of various sizes and scales and with different orientations to technology development. They include a diverse group of large and small companies, nonprofit organizations, and universities. In some instances, competitors joined to overcome rather complex technical issues. Also, the IIH focused program encouraged collaborations among computer and medical professionals and organizations to enhance the development of needed technologies and to “… help the health care industry avoid ‘fragmentation.’”9
New Format for Proposal Solicitation, Review, and Selection
Beginning with fiscal year 1999, the ATP merged the concept of focused program competitions and general competitions, resulting in an “open” format that combines the best features of previous competition models. Under an open competition, a proposal selected for funding that is synergistic with an existing focused program is managed under that program. In other cases, proposals developing complementary technologies that form a critical mass are “bundled,”# treated as a virtual focused program, and managed like the announced focused programs.
In health care informatics, proposals that formerly would have been submitted under the IIH Focused Program competition are now directed to the Information Technology Source Evaluation Board. Proposals selected for funding will be administered as part of the IIH Focused Program. The ATP continues to work with industry and other organizations to define and update current challenges and opportunities in medical informatics.
Companies wanting to submit proposals that address elements of any of the three tiers of the pyramid model developed under the existing IIH focused program may still do so. Alternatively, companies may submit proposals offering innovative solutions to those technical challenges outlined in the white paper authored jointly by ATP and industry entitled “Initiatives in Healthcare Informatics” and available at the ATP Web site, www.atp.nist.gov. New technical areas that have not been addressed in the IIH focused program, by the white paper, or in other ATP focused program areas are also encouraged. All proposals submitted to the ATP will be evaluated solely on their scientific and technological merit and their potential for broad-based economic benefits, with parts weighted equally. There is no longer a need to determine whether a proposal falls within the scope of a specific technical program.
Conclusions
The ATP IIH focused program is intended to accelerate the development of infrastructural tools and the user interface and efficiency-enhancement technology necessary for a national information infrastructure for health care. It encourages their development from the “bottom up” rather than imposing them in a “top down” fashion, which could have resulted in restrictions on the types of technologies developed. The key to advances remains the development of open, interoperable yet secure systems—systems that will provide the medical community with the capability to integrate diverse information and business systems as well as the data necessary to support continuous quality improvement. The program thus addresses several primary issues of critical importance in the delivery of health care.
The IIH focused program has also acted as a catalyst for collaborations, bringing together the stakeholders and providing opportunities to pursue cross-disciplinary projects, with participation from health care providers, computer scientists, and information technology specialists. In several cases, collaborations have included companies that never had and, under ordinary circumstances, never would have worked together.
Such efforts reduce the likelihood of closed systems and increase industry entry opportunities for small and medium-sized companies. For the end user, this program has the potential to accelerate market acceptance and enable industry to improve medical care while lowering costs.
Today, with rapid changes in both technology and the delivery of health care, new challenges face health care informatics research. The ATP provides a vehicle by which government–industry partnerships in this area can accelerate the development of high-risk technologies and offer a promise of significant commercial payoffs and widespread benefits for the economy.
Footnotes
The ATP statute originated in the Omnibus Trade and Competitiveness Act of 1988 (Pub. L. 100-418, 15 U.S.C. 278n) and was amended by the American Technology Preeminence Act of 1991 (Pub. L. 102-245).
High-risk technologies are defined as technical challenges “that should result in a dramatic change in the future direction of technology. Risk may be high in developing single innovations, integrating technologies, or both.”4
“Focused programs are defined as multi-year efforts aimed at specific, well-defined technology and business goals. These programs, which involve the parallel development of a suite of interlocking research and development projects, tackle major technology problems with high payoff potential which cannot be solved by an occasional project coming through the general competition. By managing groups of projects that complement and reinforce each other, the ATP can have the greatest possible impact on the economy.” (See http://www.atp.nist.gov/atp/.)
White papers are a mechanism by which industry conceptualizes the problems it is having difficulty addressing, including the kinds of technological barriers that must be overcome.
Additional white papers were received from workshop attendees as well as from others who became aware of the program.
The “bundling” of proposals for the purpose of creating a “virtual” focused program will occur only when a critical mass of proposals in a shared domain has been achieved. Any proposal that does not fall within an announced or virtual focused program is managed independently.
References
- 1.Blum BI, Duncan K (eds). A History of Medical Informatics. Reading, Mass.: Addison Wesley, 1990.
- 2.Etzkowitz H, Webster A, Healey P (eds). Capitalizing Knowledge: New Intersection of Industry and Academia. Albany, NY: State University of New York Press, 1998.
- 3.National Science Foundation. Comparing National Efforts at Technological Foresight, Science Indicators. Chapter 6. Arlington, Va: NSF, 1998.
- 4.U.S. Department of Commerce, National Institute of Standards and Technology, Advanced Technology Program. ATP Proposal Preparation Kit. Gaithersburg, Md.: NIST/ATP, Nov 1999.
- 5.U.S. Department of Commerce, National Institute of Standards and Technology, Advanced Technology Program. Information Infrastructure for Healthcare 94-04. Gaithersburg, Md.: NIST/ATP, 1994.
- 6.U.S. Department of Commerce, National Institute of Standards and Technology, Advanced Technology Program. Information Infrastructure for Healthcare 95-10. Gaithersburg, Md.: NIST/ATP, 1995.
- 7.U.S. Department of Commerce, National Institute of Standards and Technology, Advanced Technology Program. Information Infrastructure for Healthcare 97-03. Gaithersburg, Md.: NIST/ATP, 1997.
- 8.U.S. Department of Commerce, National Institute of Standards and Technology, Advanced Technology Program. Program Idea Guide. Gaithersburg, Md.: NIST/ATP, May 1997.
- 9.Etzkowitz H, Spivack R. Information Infrastructure for Healthcare: An Evaluation of a Government–Industry Technology Development Initiative. Gaithersburg, Md.: NIST/ATP, Oct 1999. Publication NISTIR 6404.