

Abstract
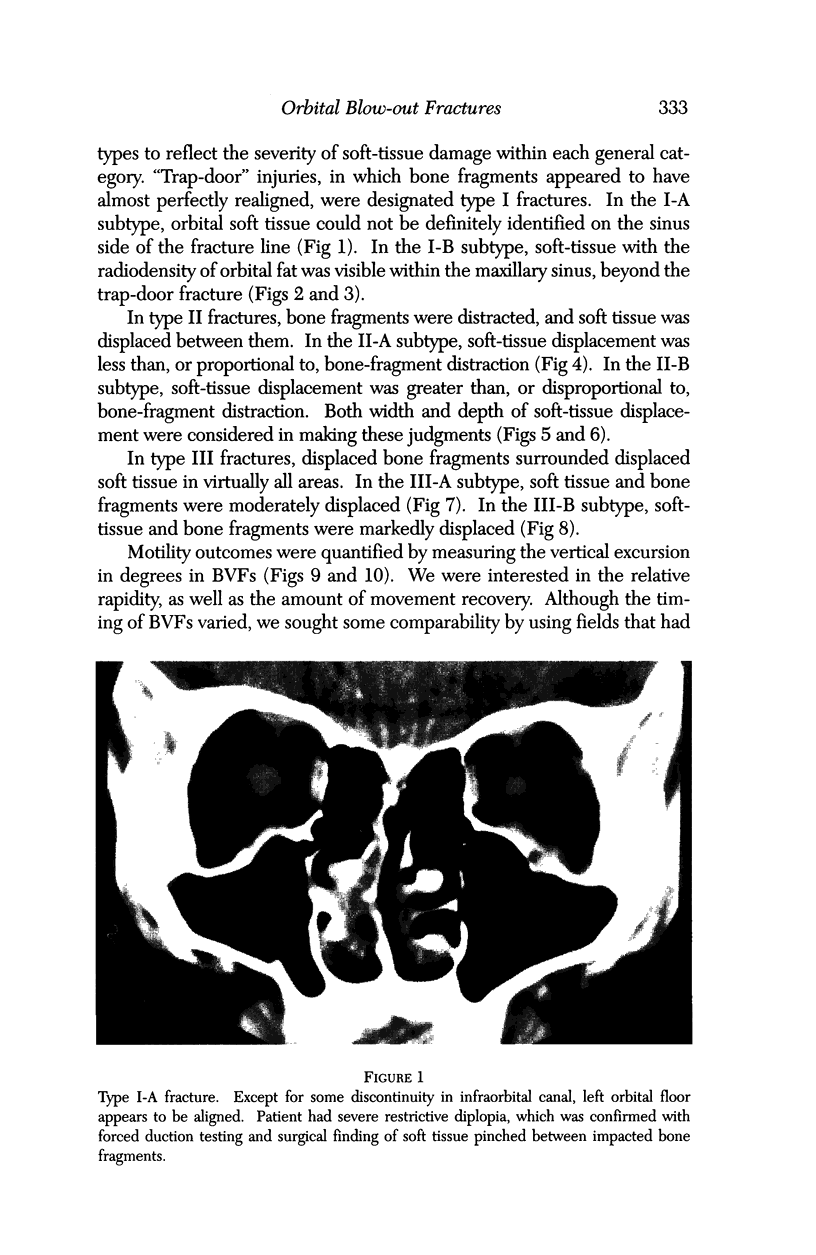
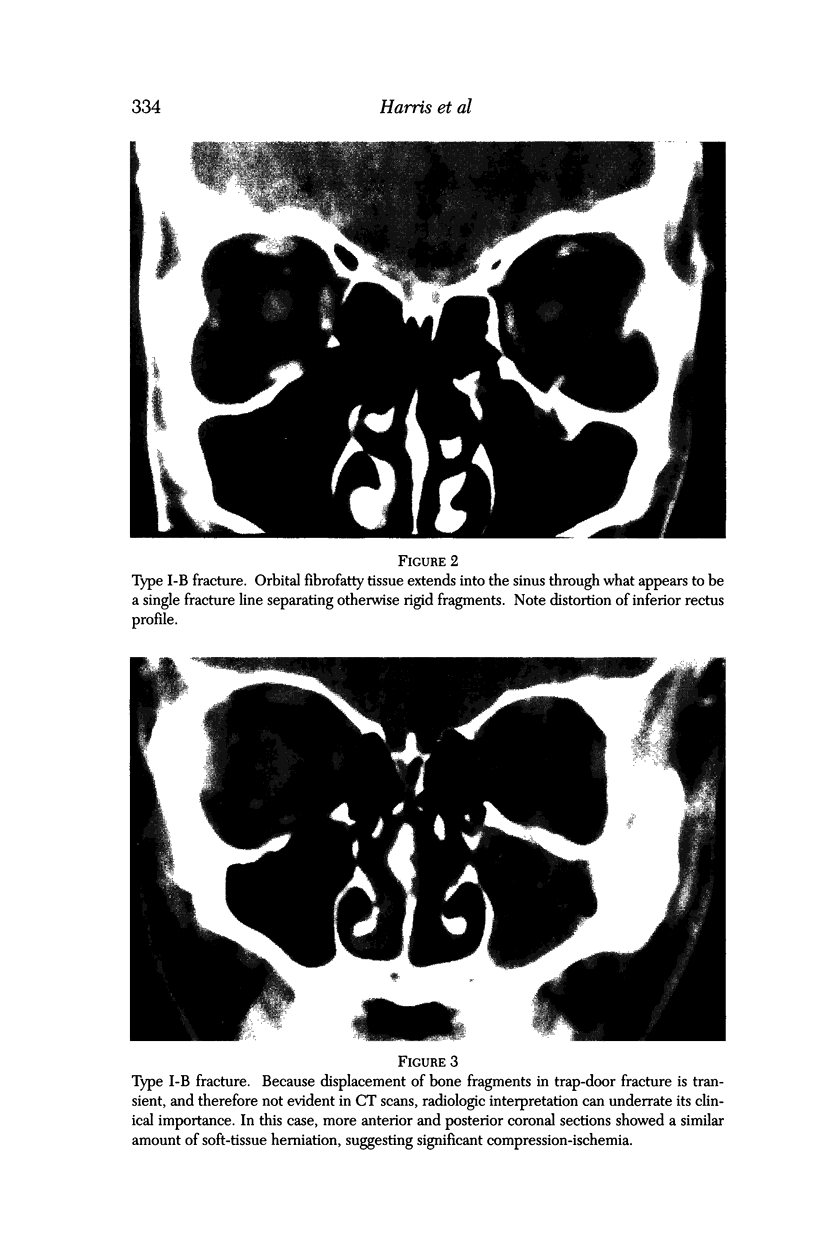
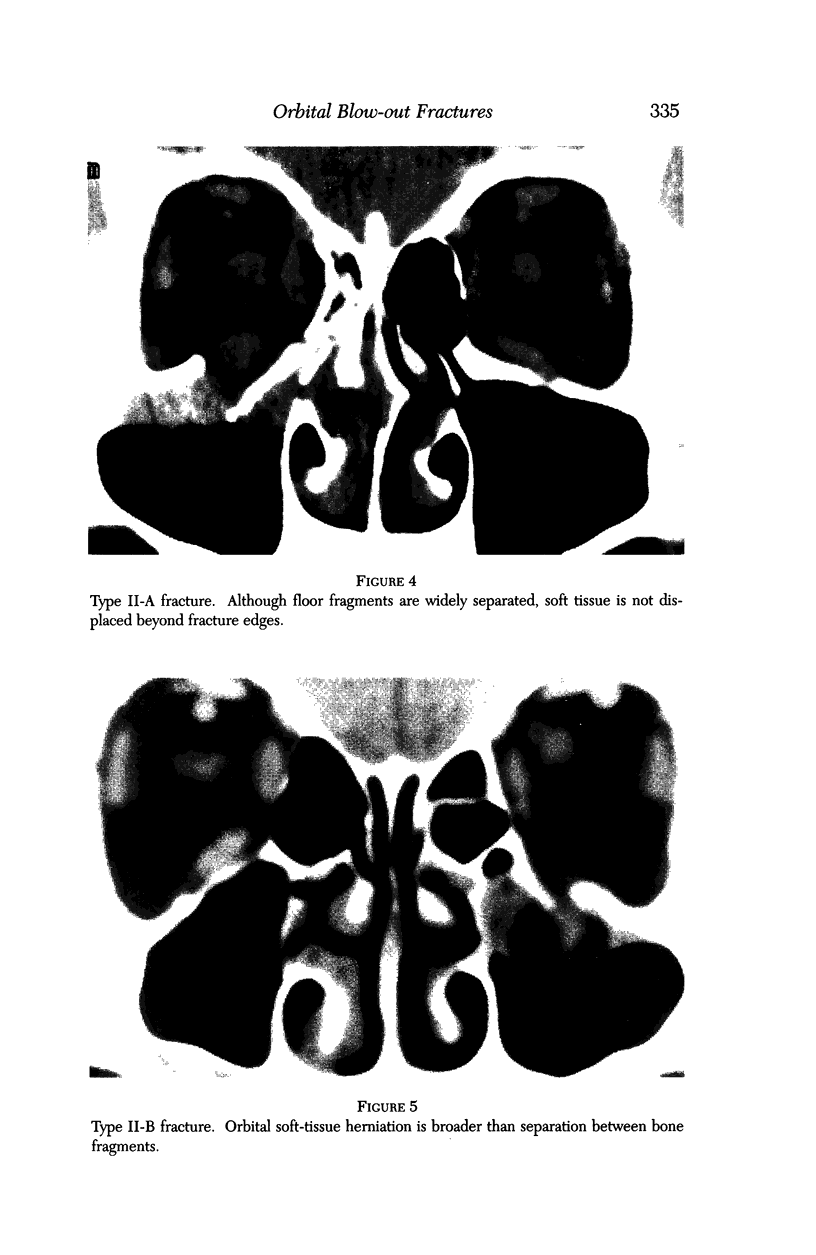
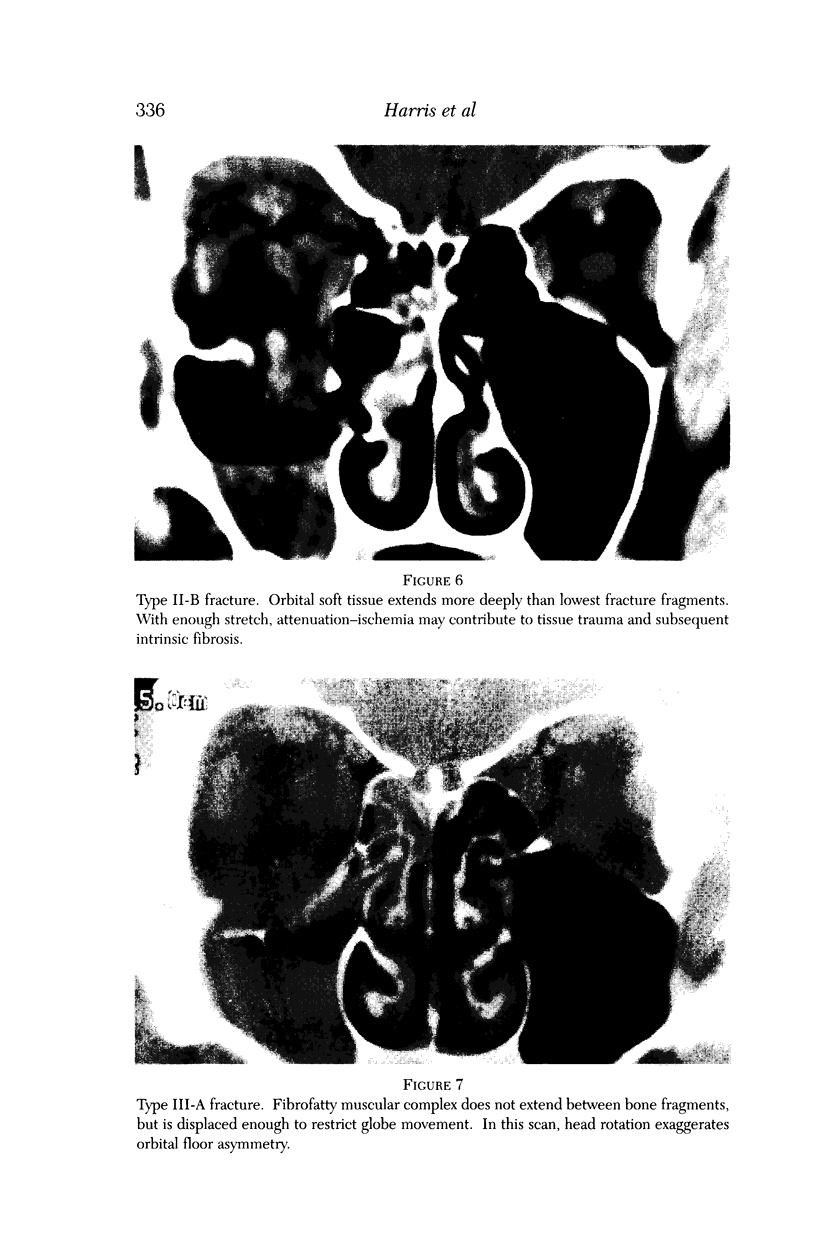
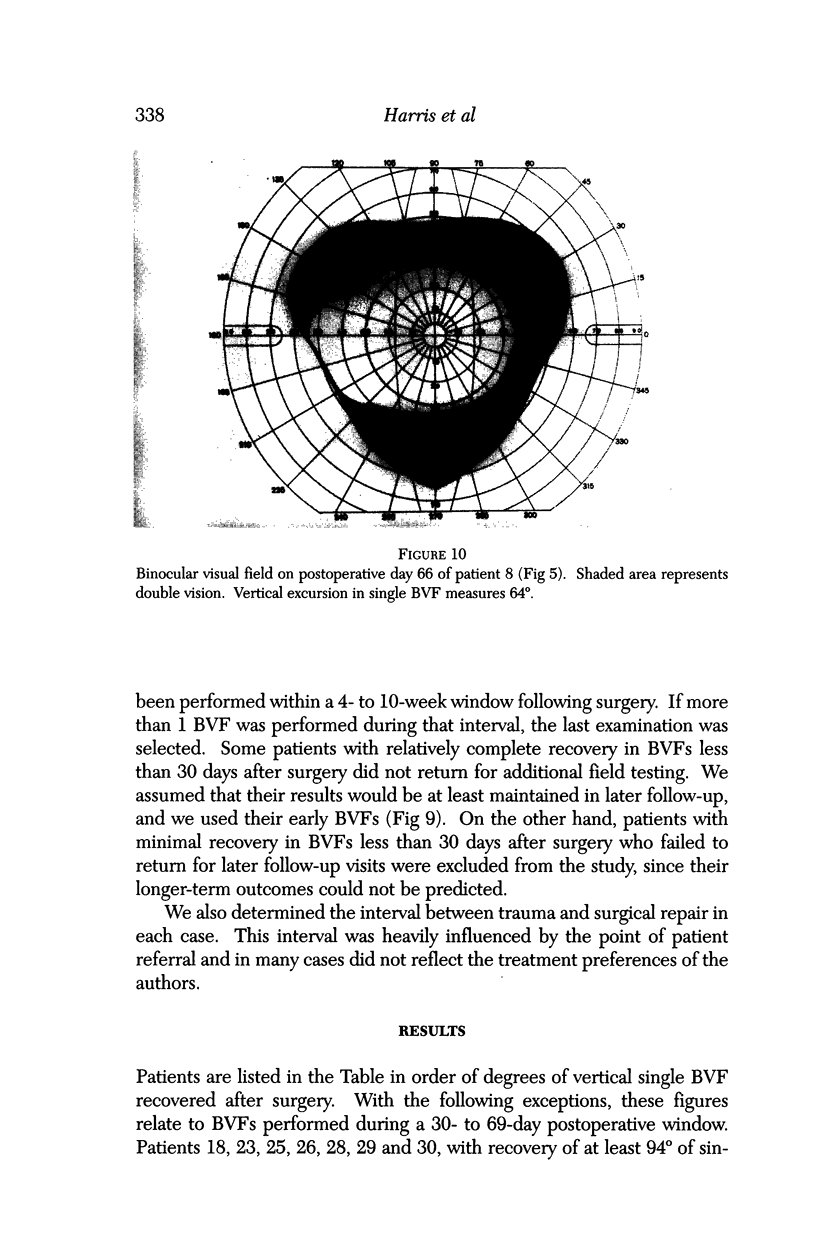
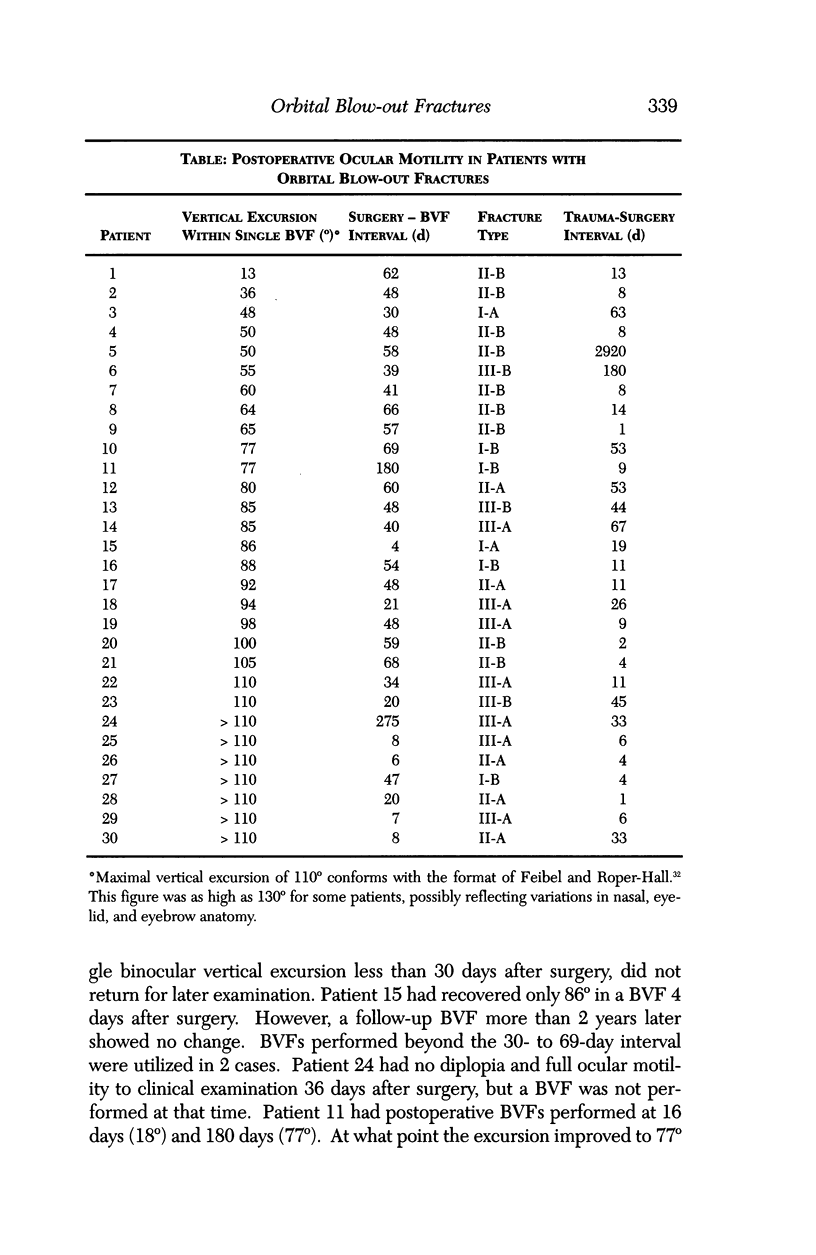
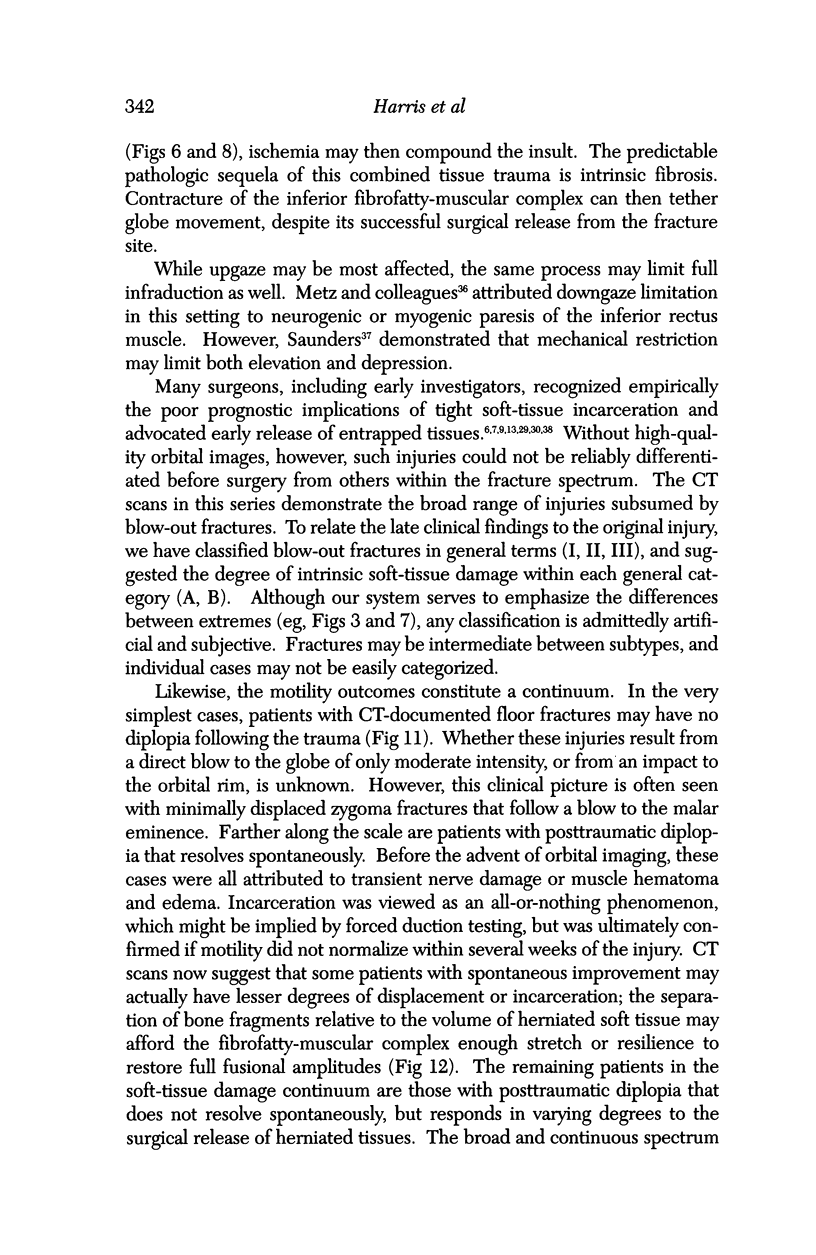
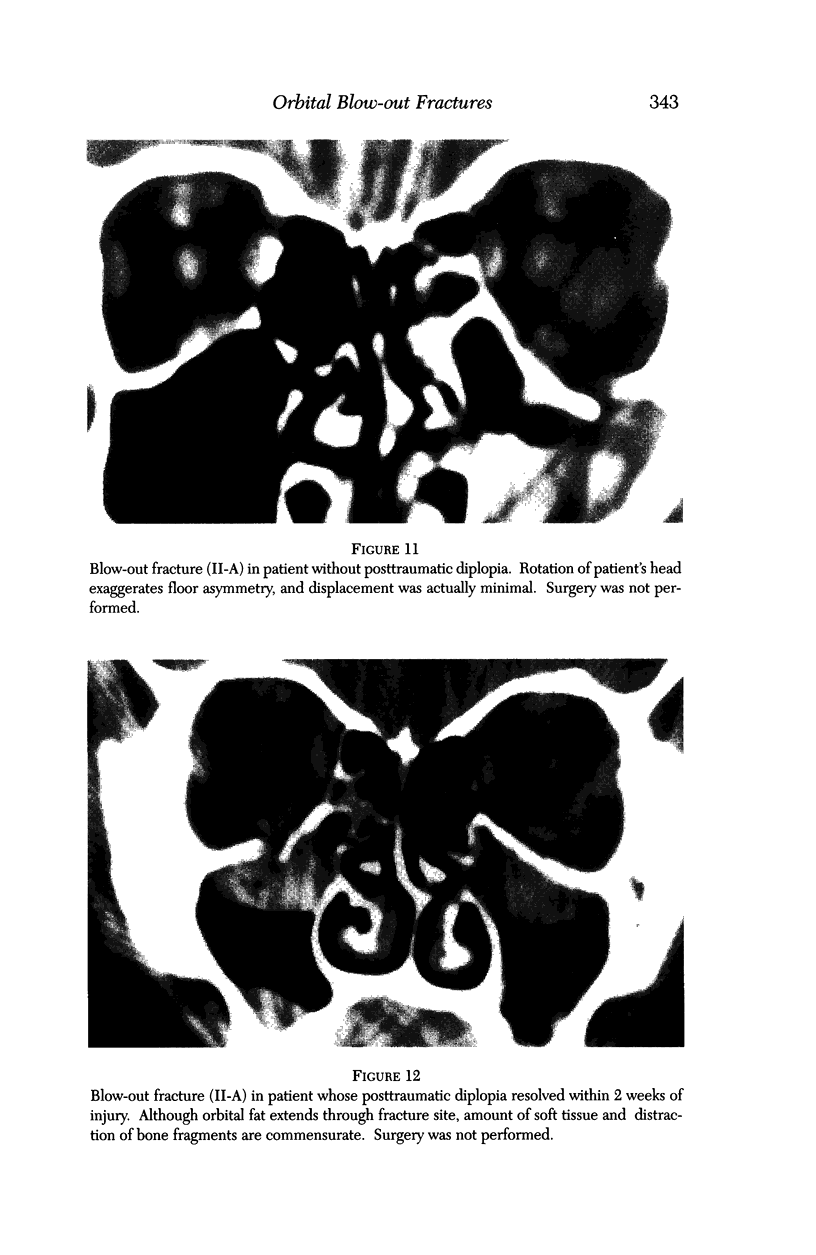
BACKGROUND/PURPOSE: Although the management of orbital blow-out fractures was controversial for many years, refined imaging with computed tomography (CT) helped to narrow the poles of the debate. Many orbital surgeons currently recommend repair if fracture size portends late enophthalmos, or if diplopia has not substantially resolved within 2 weeks of the injury. While volumetric considerations have been generally well-served by this approach, ocular motility outcomes have been less than ideal. In one series, almost 50% of patients had residual diplopia 6 months after surgery. A fine network of fibrous septa that functionally unites the periosteum of the orbital floor, the inferior fibrofatty tissues, and the sheaths of the inferior rectus and oblique muscles was demonstrated by Koornneef. Entrapment between bone fragments of any of the components of this anatomic unit can limit ocular motility. Based on the pathogenesis of blow-out fractures, in which the fibrofatty-muscular complex is driven to varying degrees between bone fragments, some measure of soft tissue damage might be anticipated. Subsequent intrinsic fibrosis and contraction can tether globe movement, despite complete reduction of herniated orbital tissue from the fracture site. We postulated that the extent of this soft tissue damage might be estimated from preoperative imaging studies. METHODS: Study criteria included: retrievable coronal CT scans; fractures of the orbital floor without rim involvement, with or without extension into the medial wall; preoperative diplopia; surgical repair by a single surgeon; complete release of entrapped tissues; and postoperative ocular motility outcomes documented with binocular visual fields (BVFs). Thirty patients met all criteria. The CT scans and BVFs were assessed by different examiners among the authors. Fractures were classified into 3 general categories and 2 subtypes to reflect the severity of soft tissue damage within each category. "Trap-door" injuries, in which bone fragments appeared to have almost perfectly realigned, were classified as type I fractures. In the I-A subtype, no orbital tissue was visible on the sinus side of the fracture line. In the I-B subtype, soft tissue with the radiodensity of orbital fat was visible within the maxillary sinus. In type II fractures, bone fragments were distracted and soft tissue was displaced between them. In the II-A subtype, soft tissue displacement was less than, or proportional to, bone fragment distraction. In the II-B subtype, soft tissue displacement was greater than bone fragment distraction. In type III fractures, displaced bone fragments surrounded displaced soft tissue in all areas. In the III-A subtype, soft tissue and bone were moderately displaced. In the III-B subtype, both were markedly displaced. Motility outcomes were quantified by measuring the vertical excursion in BVFs. The interval between trauma and surgical repair was also determined. RESULTS: Among the 15 patients with a motility outcome in BVFs which was poorer than the median (86 degrees or less of single binocular vertical excursion), 4 patients (27%) had type A fractures; 11 patients (73%) had type B fractures. Among the 15 patients with a better outcome than the median (88 degrees or more), 10 patients (67%) had type A fractures; 5 patients (33%) had type B fractures. These differences became more defined as analysis moved away from the median. Among 5 patients with type B fractures and better than the median result in BVFs, 3 patients (60%) had surgical repair during the first week after injury. Among the 11 patients with type B fractures and less than the median result, 1 patient (9%) had repair during the first week. CONCLUSIONS: When the CT-depicted relationship between bone fragments and soft tissues is considered, a wide spectrum of injuries is subsumed under the rubric of blow-out fractures. In general, greater degrees of soft tissue incarceration or displacement, with presumably greater intrinsic damage and subsequent fibrosis, appear to result in poorer motility outcomes. Although this retrospective study does not conclusively prove its benefit, an urgent surgical approach to selected injuries should be considered.
Full text
PDF

Images in this article



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Biesman B. S., Hornblass A., Lisman R., Kazlas M. Diplopia after surgical repair of orbital floor fractures. Ophthal Plast Reconstr Surg. 1996 Mar;12(1):9–17. doi: 10.1097/00002341-199603000-00002. [DOI] [PubMed] [Google Scholar]
- COLE H. G., SMITH B. Eye muscle imbalance complicating orbital floor fractures. Am J Ophthalmol. 1963 May;55:930–935. doi: 10.1016/0002-9394(63)90370-2. [DOI] [PubMed] [Google Scholar]
- Converse J. M., Smith B., Obear M. F., Wood-Smith D. Orbital blowout fractures: a ten-year survey. Plast Reconstr Surg. 1967 Jan;39(1):20–36. doi: 10.1097/00006534-196701000-00002. [DOI] [PubMed] [Google Scholar]
- Dortzbach R. K., Elner V. M. Which orbital floor blowout fractures need surgery? Adv Ophthalmic Plast Reconstr Surg. 1987;6:287–289. [PubMed] [Google Scholar]
- Emery J. M., Noorden G. K., Sclernitzauer D. A. Orbital floor fractures: long-term follow-up of cases with and without surgical repair. Trans Am Acad Ophthalmol Otolaryngol. 1971 Jul-Aug;75(4):802–812. [PubMed] [Google Scholar]
- Feibel R. M., Roper-Hall G. Evaluation of the field of binocular single vision in incomitant strabismus. Am J Ophthalmol. 1974 Nov;78(5):800–805. doi: 10.1016/0002-9394(74)90303-1. [DOI] [PubMed] [Google Scholar]
- Gilbard S. M., Mafee M. F., Lagouros P. A., Langer B. G. Orbital blowout fractures. The prognostic significance of computed tomography. Ophthalmology. 1985 Nov;92(11):1523–1528. doi: 10.1016/s0161-6420(85)33826-5. [DOI] [PubMed] [Google Scholar]
- Greenwald H. S., Jr, Keeney A. H., Shannon G. M. A review of 128 patients with orbital fractures. Am J Ophthalmol. 1974 Oct;78(4):655–664. doi: 10.1016/s0002-9394(14)76304-4. [DOI] [PubMed] [Google Scholar]
- Hawes M. J., Dortzbach R. K. Surgery on orbital floor fractures. Influence of time of repair and fracture size. Ophthalmology. 1983 Sep;90(9):1066–1070. doi: 10.1016/s0161-6420(83)80049-9. [DOI] [PubMed] [Google Scholar]
- Ilankovan V., Hadley D., Moos K., el Attar A. A comparison of imaging techniques with surgical experience in orbital injuries. A prospective study. J Craniomaxillofac Surg. 1991 Nov;19(8):348–352. doi: 10.1016/s1010-5182(05)80277-x. [DOI] [PubMed] [Google Scholar]
- Jackson A., Whitehouse R. W. Low-dose computed tomographic imaging in orbital trauma. Br J Radiol. 1993 Aug;66(788):655–661. doi: 10.1259/0007-1285-66-788-655. [DOI] [PubMed] [Google Scholar]
- Koornneef L. Current concepts on the management of orbital blow-out fractures. Ann Plast Surg. 1982 Sep;9(3):185–200. doi: 10.1097/00000637-198209000-00001. [DOI] [PubMed] [Google Scholar]
- Koornneef L. Orbital septa: anatomy and function. Ophthalmology. 1979 May;86(5):876–880. doi: 10.1016/s0161-6420(79)35444-6. [DOI] [PubMed] [Google Scholar]
- Koornneef L., Zonneveld F. W. The role of direct multiplanar high resolution CT in the assessment and management of orbital trauma. Radiol Clin North Am. 1987 Jul;25(4):753–766. [PubMed] [Google Scholar]
- LERMAN S., CRAMER L. M. BLOWOUT FRACTURES OF THE ORBIT. Am J Ophthalmol. 1964 Feb;57:264–267. doi: 10.1016/0002-9394(64)91832-x. [DOI] [PubMed] [Google Scholar]
- Manson P. N., Iliff N. Management of blow-out fractures of the orbital floor. II. Early repair for selected injuries. Surv Ophthalmol. 1991 Jan-Feb;35(4):280–292. doi: 10.1016/0039-6257(91)90049-l. [DOI] [PubMed] [Google Scholar]
- Metz H. S., Scott W. E., Madson E., Scott A. B. Saccadic velocity and active force studies in blow-out fractures of the orbit. Am J Ophthalmol. 1974 Oct;78(4):665–670. doi: 10.1016/s0002-9394(14)76305-6. [DOI] [PubMed] [Google Scholar]
- Millman A. L., Della Rocca R. C., Spector S., Leibeskind A. L., Messina A. Steroids and orbital blowout fractures--a new systematic concept in medical management and surgical decision-making. Adv Ophthalmic Plast Reconstr Surg. 1987;6:291–300. [PubMed] [Google Scholar]
- Nathanson A., Matthis S. P., Tengvar M. Diagnosis and treatment of fractures of the orbital floor. A ten-year retrospective study. Acta Otolaryngol Suppl. 1992;492:28–32. doi: 10.3109/00016489209136804. [DOI] [PubMed] [Google Scholar]
- Nicholson D. H., Guzak S. W. Visual loss complicating repair of orbital floor fractures. Arch Ophthalmol. 1971 Oct;86(4):369–375. doi: 10.1001/archopht.1971.01000010371003. [DOI] [PubMed] [Google Scholar]
- Putterman A. M., Stevens T., Urist M. J. Nonsurgical management of blow-out fractures of the orbital floor. Am J Ophthalmol. 1974 Feb;77(2):232–239. doi: 10.1016/0002-9394(74)90679-5. [DOI] [PubMed] [Google Scholar]
- Ruttum M. S., Harris G. J. Orbital blowout fracture with ipsilateral fourth nerve palsy. Am J Ophthalmol. 1985 Aug 15;100(2):343–344. doi: 10.1016/0002-9394(85)90816-5. [DOI] [PubMed] [Google Scholar]
- SMITH B., CONVERSE J. M. Early treatment of orbital floor fractures. Trans Am Acad Ophthalmol Otolaryngol. 1957 Sep-Oct;61(5):602–608. [PubMed] [Google Scholar]
- SMITH B., REGAN W. F., Jr Blow-out fracture of the orbit; mechanism and correction of internal orbital fracture. Am J Ophthalmol. 1957 Dec;44(6):733–739. doi: 10.1016/0002-9394(76)90774-1. [DOI] [PubMed] [Google Scholar]
- SMITH B., REGAN W. F., Jr Blow-out fracture of the orbit; mechanism and correction of internal orbital fracture. Am J Ophthalmol. 1957 Dec;44(6):733–739. doi: 10.1016/0002-9394(76)90774-1. [DOI] [PubMed] [Google Scholar]
- Saunders R. A. Incomitant vertical strabismus. Treatment with posterior fixation of the inferior rectus muscle. Arch Ophthalmol. 1984 Aug;102(8):1174–1177. doi: 10.1001/archopht.1984.01040030952022. [DOI] [PubMed] [Google Scholar]
- Smith B., Lisman R. D., Simonton J., Della Rocca R. Volkmann's contracture of the extraocular muscles following blowout fracture. Plast Reconstr Surg. 1984 Aug;74(2):200–216. doi: 10.1097/00006534-198408000-00004. [DOI] [PubMed] [Google Scholar]
- Tadmor R., New P. F. Computed tomography of the orbit with special emphasis on coronal sections: Part I. Normal anatomy. J Comput Assist Tomogr. 1978 Jan;2(1):24–34. doi: 10.1097/00004728-197801000-00004. [DOI] [PubMed] [Google Scholar]
- Tonami H., Yamamoto I., Matsuda M., Tamamura H., Yokota H., Nakagawa T., Takarada A., Okimura T. Orbital fractures: surface coil MR imaging. Radiology. 1991 Jun;179(3):789–794. doi: 10.1148/radiology.179.3.2027993. [DOI] [PubMed] [Google Scholar]
- Wachler B. S., Holds J. B. The missing muscle syndrome in blowout fractures: an indication for urgent surgery. Ophthal Plast Reconstr Surg. 1998 Jan;14(1):17–18. doi: 10.1097/00002341-199801000-00005. [DOI] [PubMed] [Google Scholar]