

Abstract
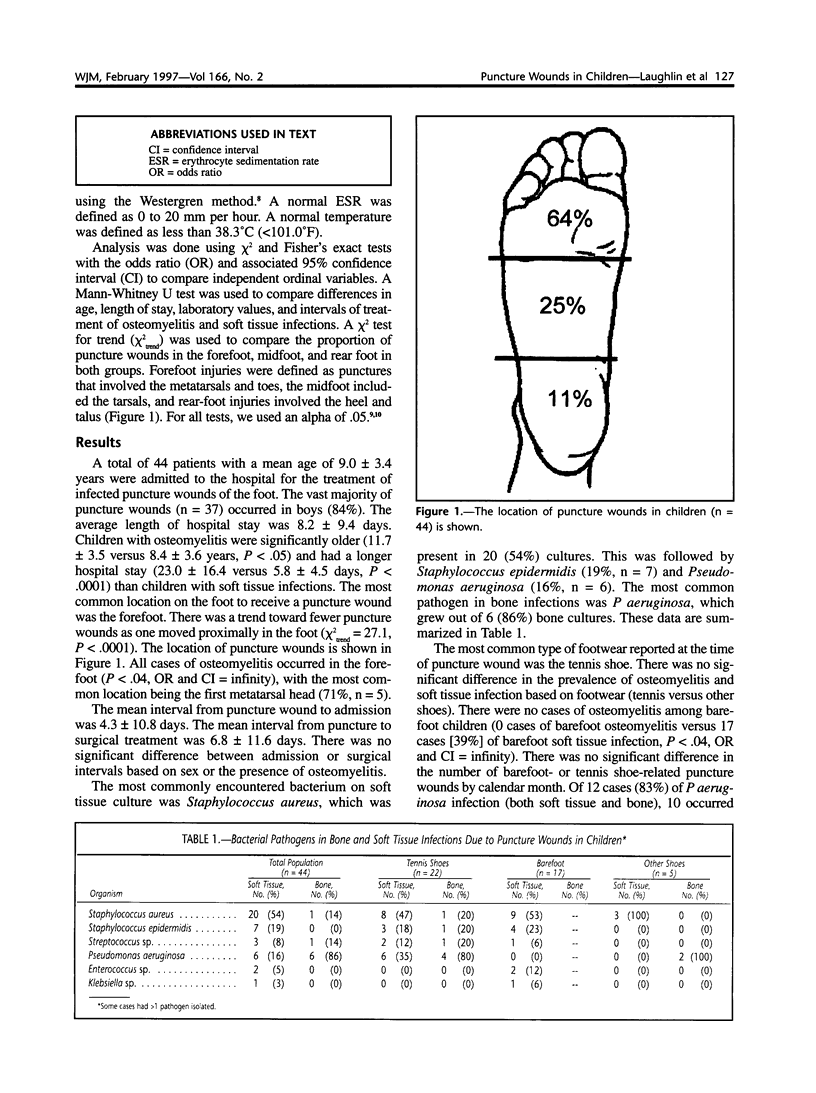
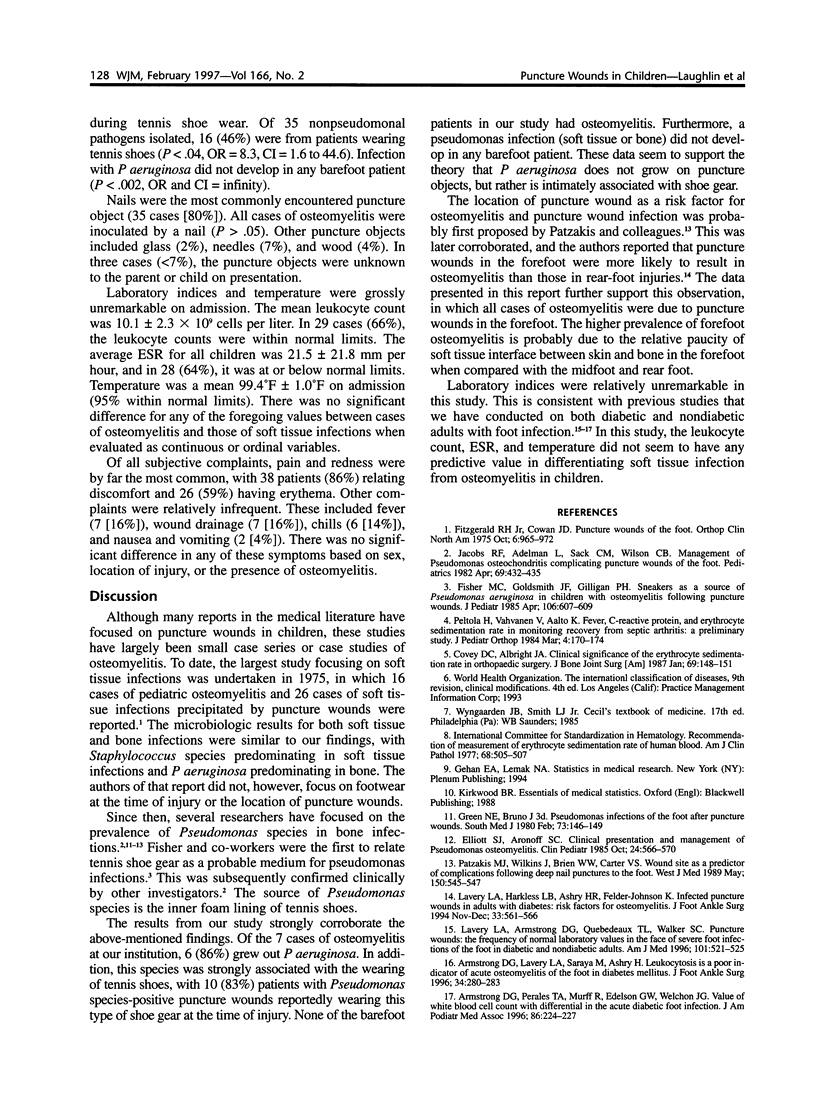
We report on the prevalence of osteomyelitis, the prevalence of soft tissue infections, and the type and number of pathogens encountered in bone and soft tissue infections caused by puncture wounds in children. In addition, we seek to establish whether shoe gear plays a role in the flora in infected puncture wounds and if laboratory indices are indicative of the presence of infection. The group consisted of 44 nondiabetic children admitted to hospital for puncture wounds of the foot. Cultures were positive for osteomyelitis in 7 patients (16%), all involving the forefoot (P < .04). The most common pathogen in soft tissue infections was Staphylococcus aureus. The most common pathogen in osteomyelitis was Pseudomonas aeruginosa. There was no significant difference in the prevalence of osteomyelitis and soft tissue infection based on footwear. There were no cases of osteomyelitis encountered among barefoot children (P < .04). In 10 cases (83%), P aeruginosa infection (both soft tissue and bone) occurred while the patients were wearing tennis shoes (P < .04). In this study, the leukocyte count (normal in 29 patients [66%]), erythrocyte sedimentation rate (normal in 28 patients [64%]), and temperature (normal in 44 patients [95%]) did not have any predictive value in differentiating soft tissue infection from osteomyelitis in children.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Armstrong D. G., Lavery L. A., Sariaya M., Ashry H. Leukocytosis is a poor indicator of acute osteomyelitis of the foot in diabetes mellitus. J Foot Ankle Surg. 1996 Jul-Aug;35(4):280–283. doi: 10.1016/s1067-2516(96)80075-5. [DOI] [PubMed] [Google Scholar]
- Armstrong D. G., Perales T. A., Murff R. T., Edelson G. W., Welchon J. G. Value of white blood cell count with differential in the acute diabetic foot infection. J Am Podiatr Med Assoc. 1996 May;86(5):224–227. doi: 10.7547/87507315-86-5-224. [DOI] [PubMed] [Google Scholar]
- Covey D. C., Albright J. A. Clinical significance of the erythrocyte sedimentation rate in orthopaedic surgery. J Bone Joint Surg Am. 1987 Jan;69(1):148–151. [PubMed] [Google Scholar]
- Elliott S. J., Aronoff S. C. Clinical presentation and management of Pseudomonas osteomyelitis. Clin Pediatr (Phila) 1985 Oct;24(10):566–570. doi: 10.1177/000992288502401004. [DOI] [PubMed] [Google Scholar]
- Fisher M. C., Goldsmith J. F., Gilligan P. H. Sneakers as a source of Pseudomonas aeruginosa in children with osteomyelitis following puncture wounds. J Pediatr. 1985 Apr;106(4):607–609. doi: 10.1016/s0022-3476(85)80082-2. [DOI] [PubMed] [Google Scholar]
- Fitzgerald R. H., Jr, Cowan J. D. Puncture wounds of the foot. Orthop Clin North Am. 1975 Oct;6(4):965–972. [PubMed] [Google Scholar]
- Green N. E., Bruno J., 3rd Pseudomonas infections of the foot after puncture wounds. South Med J. 1980 Feb;73(2):146–149. doi: 10.1097/00007611-198002000-00008. [DOI] [PubMed] [Google Scholar]
- Jacobs R. F., Adelman L., Sack C. M., Wilson C. B. Management of Pseudomonas osteochondritis complicating puncture wounds of the foot. Pediatrics. 1982 Apr;69(4):432–435. [PubMed] [Google Scholar]
- Lavery L. A., Armstrong D. G., Quebedeaux T. L., Walker S. C. Puncture wounds: normal laboratory values in the face of severe infection in diabetics and non-diabetics. Am J Med. 1996 Nov;101(5):521–525. doi: 10.1016/s0002-9343(96)00283-5. [DOI] [PubMed] [Google Scholar]
- Lavery L. A., Harkless L. B., Ashry H. R., Felder-Johnson K. Infected puncture wounds in adults with diabetes: risk factors for osteomyelitis. J Foot Ankle Surg. 1994 Nov-Dec;33(6):561–566. [PubMed] [Google Scholar]
- Patzakis M. J., Wilkins J., Brien W. W., Carter V. S. Wound site as a predictor of complications following deep nail punctures to the foot. West J Med. 1989 May;150(5):545–547. [PMC free article] [PubMed] [Google Scholar]
- Peltola H., Vahvanen V., Aalto K. Fever, C-reactive protein, and erythrocyte sedimentation rate in monitoring recovery from septic arthritis: a preliminary study. J Pediatr Orthop. 1984 Mar;4(2):170–174. doi: 10.1097/01241398-198403000-00004. [DOI] [PubMed] [Google Scholar]