

Abstract
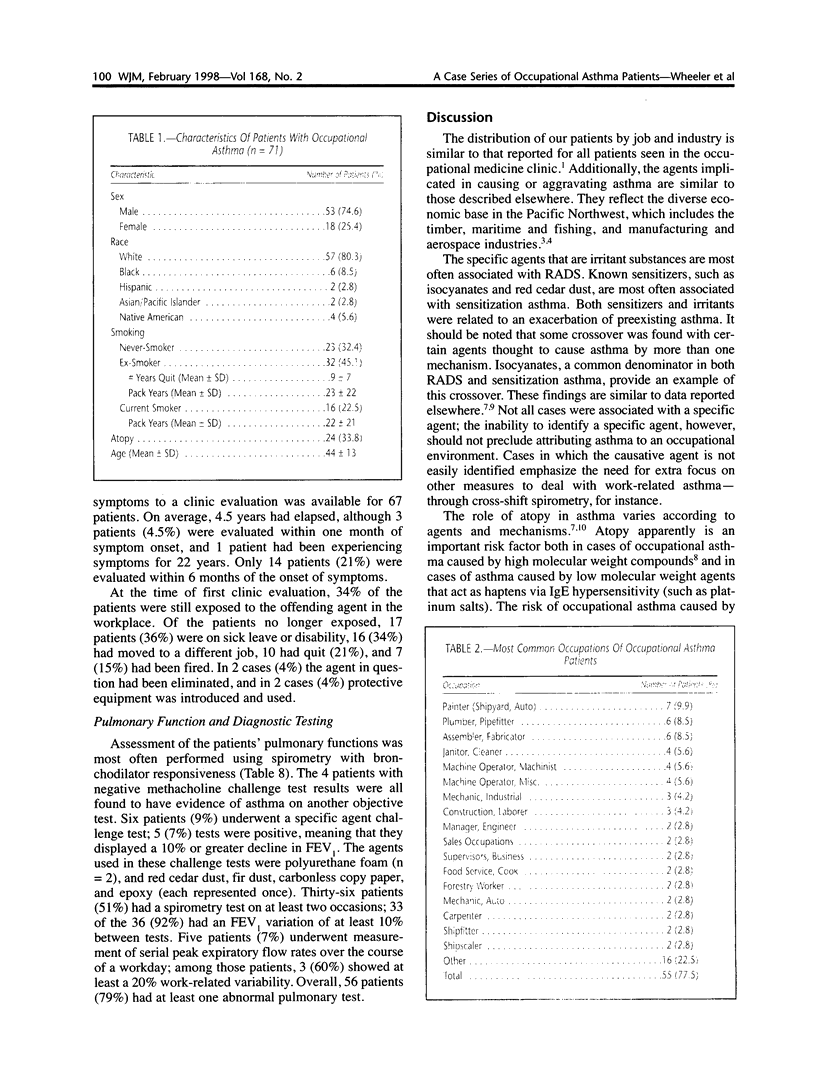
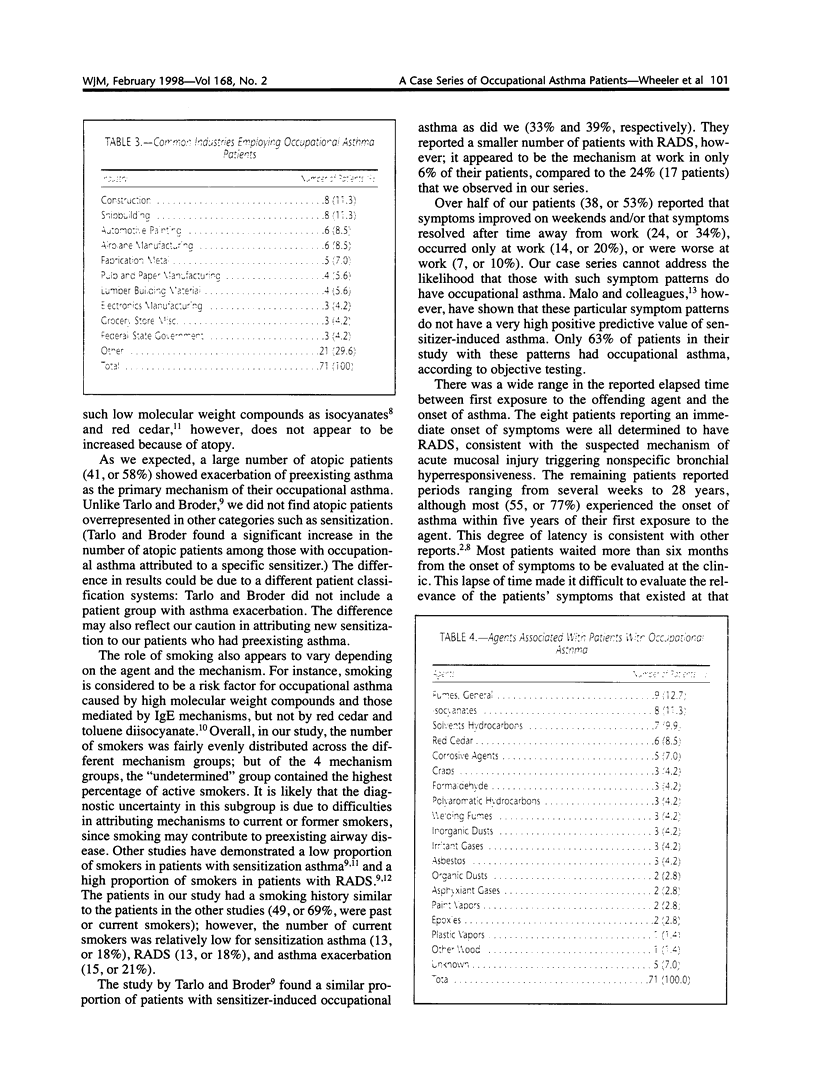
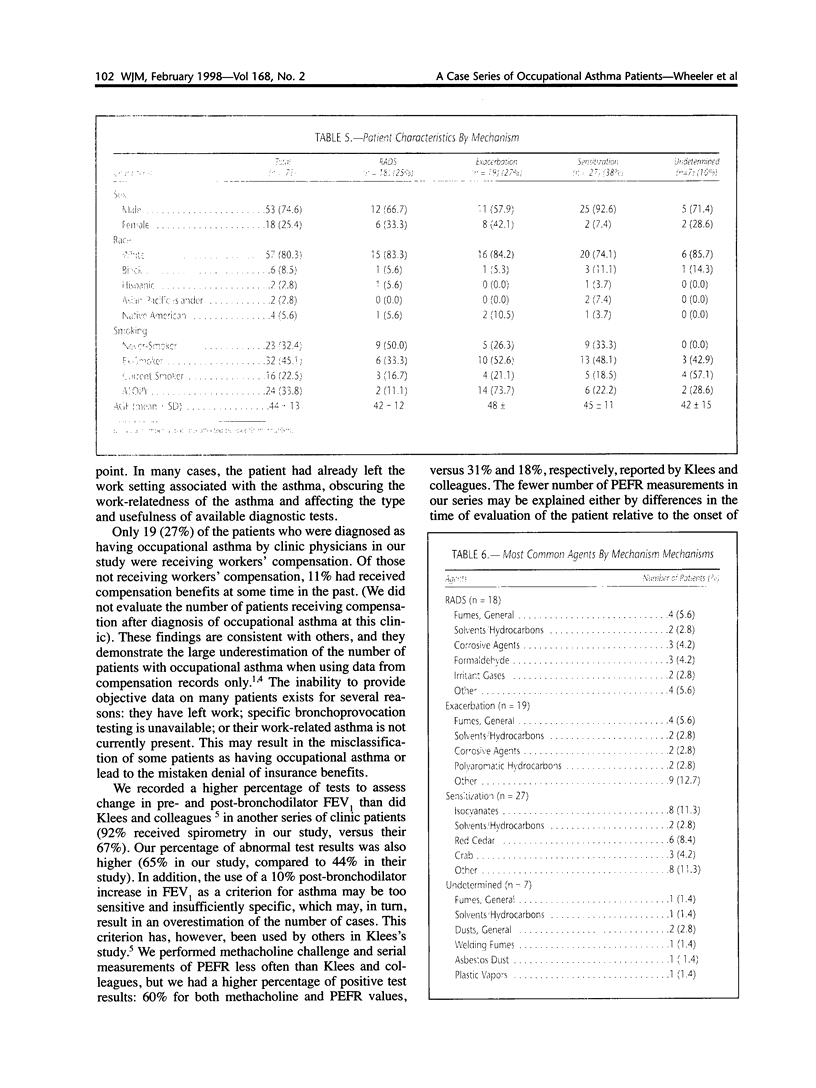
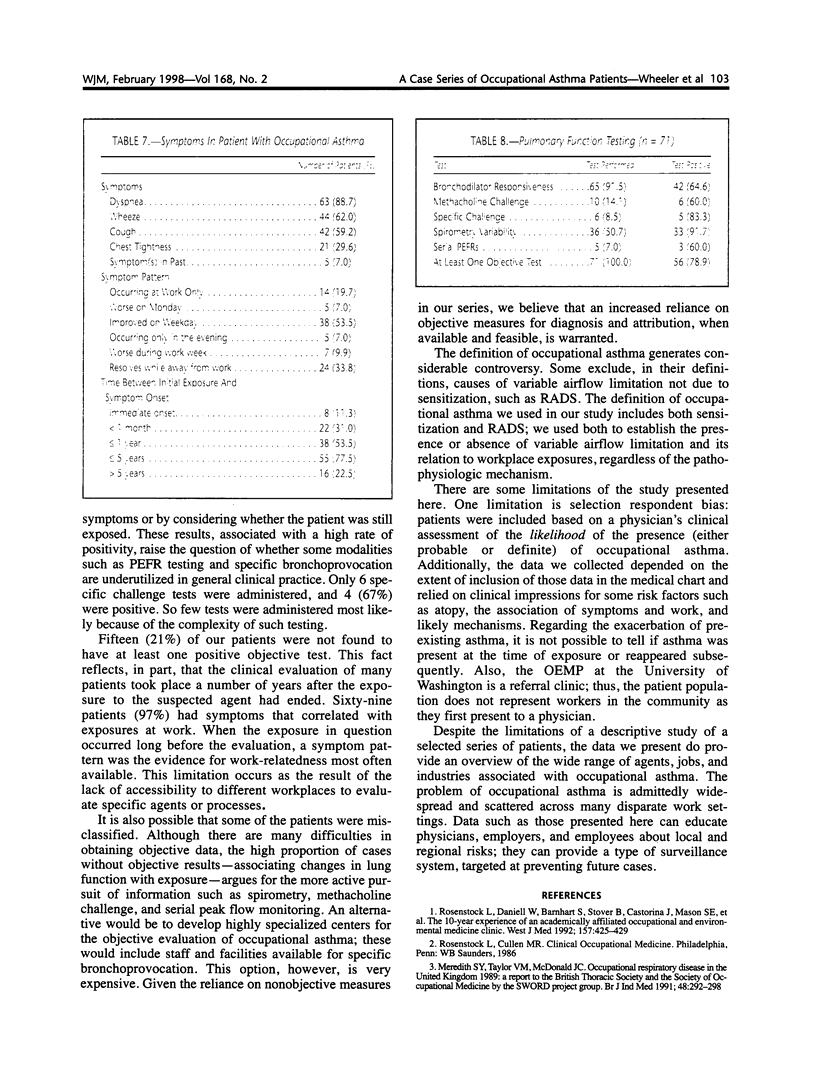
In a ten-year period at the Occupational and Environmental Medicine Program (OEMP) of the University of Washington in Seattle, 71 patients were determined by attending physicians to have work-related asthma. In this cross-sectional descriptive study, we describe these patients. Data were obtained from a database maintained by the OEMP and from chart reviews. We found that the three most common specific agents causing asthma were isocyanates, red cedar, and crabs. At least one pulmonary function study was available for all patients and was positive in 56 patients (79%). Among the 71 asthma cases reported in this article, 18 (25%) were attributed to reactive airways dysfunction syndrome (RADS); 19 (27%) to exacerbation of pre-existing asthma; 27 (38%) to sensitization; and 7 (10%) had undetermined causes. We conclude that occupational asthma presents as a result of diverse exposures in multiple work settings and with an array of characteristics. Prevention efforts need to recognize this diversity.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Boulet L. P. Increases in airway responsiveness following acute exposure to respiratory irritants. Reactive airway dysfunction syndrome or occupational asthma? Chest. 1988 Sep;94(3):476–481. doi: 10.1378/chest.94.3.476. [DOI] [PubMed] [Google Scholar]
- Chai H., Farr R. S., Froehlich L. A., Mathison D. A., McLean J. A., Rosenthal R. R., Sheffer A. L., Spector S. L., Townley R. G. Standardization of bronchial inhalation challenge procedures. J Allergy Clin Immunol. 1975 Oct;56(4):323–327. doi: 10.1016/0091-6749(75)90107-4. [DOI] [PubMed] [Google Scholar]
- Chan-Yeung M. Immunologic and nonimmunologic mechanisms in asthma due to western red cedar (Thuja plicata). J Allergy Clin Immunol. 1982 Jul;70(1):32–37. doi: 10.1016/0091-6749(82)90198-1. [DOI] [PubMed] [Google Scholar]
- Gannon P. F., Burge P. S. A preliminary report of a surveillance scheme of occupational asthma in the West Midlands. Br J Ind Med. 1991 Sep;48(9):579–582. doi: 10.1136/oem.48.9.579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malo J. L., Ghezzo H., L'Archevêque J., Lagier F., Perrin B., Cartier A. Is the clinical history a satisfactory means of diagnosing occupational asthma? Am Rev Respir Dis. 1991 Mar;143(3):528–532. doi: 10.1164/ajrccm/143.3.528. [DOI] [PubMed] [Google Scholar]
- Meredith S. K., Taylor V. M., McDonald J. C. Occupational respiratory disease in the United Kingdom 1989: a report to the British Thoracic Society and the Society of Occupational Medicine by the SWORD project group. Br J Ind Med. 1991 May;48(5):292–298. doi: 10.1136/oem.48.5.292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenstock L., Daniell W., Barnhart S., Stover B., Castorina J., Mason S. E., Heyer N. J., Hubbard R., Kaufman J. D., Brodkin C. A. The 10-year experience of an academically affiliated occupational and environmental medicine clinic. West J Med. 1992 Oct;157(4):425–429. [PMC free article] [PubMed] [Google Scholar]
- Tarlo S. M., Broder I. Irritant-induced occupational asthma. Chest. 1989 Aug;96(2):297–300. doi: 10.1378/chest.96.2.297. [DOI] [PubMed] [Google Scholar]
- Tarlo S. M., Broder I. Outcome of assessments for occupational asthma. Chest. 1991 Aug;100(2):329–335. doi: 10.1378/chest.100.2.329. [DOI] [PubMed] [Google Scholar]