

Abstract
Study Objectives
This report describes the associations, specificities, sensitivities, and positive likelihood ratios of clinical symptoms to a finding of sleep-disordered breathing (SDB) on polysomnography in children.
Methods
Four hundred eighty unattended home polysomnograms were completed in a community-based cohort of children 6 to 11 years of age (50% boys, 42.3% Hispanic, and 52.9% between the ages of 6 and 8 years). SDB was present if the child had a respiratory disturbance index of ≥ 1 event per hour.
Measurements and Results
Boys were twice as likely as girls to have SDB (p<.01); however, witnessed apnea, ethnicity, age, obesity, and air-way size (based on clinical evaluation) were not significantly different between those with SDB and without SDB. The sensitivity of any individual or combined clinical symptoms was poor, with male sex (60%) and snoring (29.5%) having the greatest proportion of SDB children. However, high specificities for snoring (89.5%), excessive daytime sleepiness (86.3%), and learning problems (95.9%) were noted. Combinations of symptoms such as snoring+male sex (95.1%), snoring+excessive daytime sleepiness (97.0%), and snoring+learning problems (98.9%) had specificities approaching 1. Positive likelihood ratios for snoring (2.8), learning (2.8), and symptoms combined with snoring such as snoring+male sex(3.9), snoring+learning problems (4.0), and snoring+excessive daytime sleepiness (2.9) were observed.
Conclusions
Snoring, excessive daytime sleepiness, and learning problems are each highly specific, but not sensitive, for SDB in 6- to 11-year old children. However, specificities and positive likelihood ratios for the combination of some of these symptoms is sufficiently high to suggest that some children may not require a polysomnogram for the diagnosis of SDB.
Keywords: Sleep, children, sleep-disordered breathing, sleep apnea, respiratory disturbance index
Sleep disordered-breathing (SDB), including obstructive sleep apnea syndrome, is acknowledged as an important cause of morbidity in children, with behavioral and neurocognitive abnormalities occurring more commonly in children with SDB than in those without SDB.1 Symptoms that have been associated with SDB in children include frequent snoring, excessive daytime sleepiness, parasomnias, nocturnal arousals, hyperactivity, and behavioral problems.2–9
Many children with SDB present to their physician with snoring. However, snoring by itself, in the absence of other symptoms or behaviors, has insufficient predictive value, and thus is not suitable as the sole indication to perform polysomnography in children. 10 Thus, one of the more perplexing problems encountered by physicians and other providers caring for children is how to determine which elementary-school-aged child should be referred for overnight polysomnographic evaluation of SDB. Use of adult standards can be misleading because clinical manifestations of childhood SDB differ from those found in adults.11 It is possible that other symptoms or findings obtained during a clinic visit may assist the clinician in deciding whether or not to refer a child for overnight polysomnography (PSG). In clinic populations or studies with small sample sizes, some of these have been shown to be associated with SDB. However, the clinical presentation of SDB has not been evaluated in a community sample of children using full PSG. No epidemiologic study in a normative population has been conducted to model clinically obtained signs and symptoms of SDB with their corresponding polysomnographic severity.
The Tucson Children’s Assessment of Sleep Apnea (TuCASA) study is a prospective cohort study designed to determine the prevalence of objectively documented SDB in preadolescent children and to investigate its relationship to symptoms, performance on neurobehavioral measures, and physiologic and anatomic risk factors. Using only measures that could be easily obtained during an outpatient clinical visit, this report describes the usefulness of common clinical symptoms and findings as predictors of SDB in Hispanic and Caucasian elementary-school-aged children.
METHODS
The design of the TuCASA study specified recruitment of Hispanic and Caucasian children aged 6 through 11 years to undergo unattended home PSG with concomitant anthropometric measurements, to complete a pediatric sleep habits questionnaire, and to have a neurocognitive assessment. Subjects were recruited through the Tucson Unified School District, a very large district with an elementary-school population representative of children living in southern Arizona. Detailed recruitment methods have been described previously.12,13 Parents were asked to complete a short sleep-habits screening questionnaire and to provide their contact information if they would allow study personnel to call and schedule a PSG for their child.
The screening questionnaire consists of a 1-page, 13-item survey designed to assess the severity of symptoms related to obstructive sleep apnea syndrome in children. Questions such as How often does your child snore loudly? Is your child sleepy during the daytime? Does your child stop breathing during sleep? Is your child easily distracted? and Does your child have learning problems? were evaluated by the parent on the scale of Never, Rarely, Occasionally, Frequently, Almost Always, or Don’t Know. We encouraged maximum participation through recruitment incentives for the school and also allowed parents to return the survey anonymously. Children who were not of Hispanic or Caucasian ethnicity were excluded according to the study design. Parents were called regarding the possibility of a PSG for their child if they indicated their willingness to participate further. Children were excluded from the PSG recording if they had a history of asthma, obstructive sleep apnea syndrome, tonsillectomy or adenoidectomy, other chronic respiratory problems, or mental retardation. An unattended home PSG was scheduled as soon as possible after recruitment. All children meeting these criteria whose parents agreed to the home recording were scheduled.
The screening questionnaire was used to define the occurrence of habitual snoring, excessive daytime sleepiness (EDS), witnessed apnea, and learning problems. Snoring was defined as present if parents reported their child snored loudly frequently or almost always. Subjects were classified as having EDS if the parents reported that their child had any of the following frequently or almost always: child was sleepy in the daytime, fell asleep while watching TV or in school, or had problems falling asleep during the day. Witnessed apnea was present if the parents reported that their child stopped or struggled to breathe, their child’s lips turned blue, or they shook their child because they were worried about their child’s breathing during sleep frequently or almost always. The child was classified as having learning problems if the parent reported the child had learning problems frequently or almost always. Finally, the child was defined as being easily distracted, interrupting frequently, fidgety, or acting as if he or she had a motor running if the parent reported any of these symptoms frequently or almost always.
On the night of the home visit, the parent was asked to complete a detailed Sleep Habits Questionnaire. Included were questions such as: “Does this child sleepwalk?” and “Does this child talk in his or her sleep? (Talk without being fully awake?).” Responses were “Never,” “Less than three times per month,” “Three to five times per month,” or “More than five times per month.” The occurrence of these parasomnias was defined as follows: sleepwalking was present if it was reported more than 3 times per month, and sleep talking was present if it was reported more than 5 times per month. Additionally, the parent was asked “How often does this child awaken at night afraid or appearing tearful?” If the parent answered that the child had more than 5 fearful awakenings per month, then the child was classified as having fearful awakenings. Enuresis was present if it was reported as occurring more than 5 times per month. Difficulty initiating and maintaining sleep (insomnia) was present if the parents reported that their child had trouble falling asleep, staying asleep, had not enough sleep, or was troubled by waking up too early and not being able to get back to sleep. Although the specific range and order of questions used on the TuCASA sleep habits and screening questionnaires have not been previously validated, key questions in the questionnaires have face validity and were taken from those used by Carroll and colleagues.10 They also have been used in prior analyses of data from this cohort.13,14 At the time we implemented the TuCASA in 1999, there were no universally accepted and validated questionnaires of this nature to use in children.
Home-visit procedures and methods for obtaining PSG data have been described previously. Briefly, a 2-person mixed-sex team arrived at the home approximately 1 hour prior to the child’s normal bedtime. Institutional Review Board-approved informed consent was obtained from the parent, and an assent form was signed by the child. Questionnaires were administered, and anthropometric and other physiologic measurements were completed. The oral airway was examined by a trained technician and rated with a value from 1 (unobstructed) to 3 (tonsils encroaching upon airway). Unattended overnight PSGs were obtained using the Compumedics PS-2 system (Abbotsford, Victoria, Australia). The following signals were acquired as part of the TuCASA montage: C3/A2 and C4/A1 electroencephalogram, right and left electrooculogram, a bipolar submental electromyogram, thoracic and abdominal displacement (inductive plethysmography bands), air-flow (nasal/oral thermister), nasal pressure cannula, finger pulse oximetry, electrocardiogram to detect major arrhythmias (single bipolar lead), snoring microphone, body position (mercury gauge sensor), and ambient light to determine sleep period time (sensor attached to the vest to record on/off).
The Compumedics software system was used to process all PSG data. Scoring has been described in detail previously.12 Briefly, sleep stages were scored according to Rechtschaffen and Kales criteria. Arousals were identified using criteria published by the American Academy of Sleep Medicine. Apneas were scored if the amplitude (peak to trough) of the airflow signal using the thermister decreased below at least 25% of the amplitude of baseline breathing (identified during a period of regular breathing with stable oxygen levels), if this change lasted for more than 6 seconds or 2 breath cycles. Hypopneas were designated if the amplitude of any respiratory signal decreased below (approximately) 70% of the amplitude of baseline and if the thermister signal did not meet the criterion for apnea. Central events were marked if no displacement was noted on both the chest and abdominal inductance channels. Otherwise, events were scored as obstructive. After full scoring, analysis software was used to link each event to data from the oxygen saturation and arousals from the electroencephalogram channels. In this manner, the respiratory disturbance index (RDI) was defined as the number of respiratory events (apneas and hypopneas) per hour of the total sleep time. For this analysis, a 3% oxygen desaturation was required for an event to be counted in the total RDI. We considered a child to have SDB if their RDI was greater than or equal to 1 event per hour of total sleep time. Use of this definition is supported by previous evidence that a RDI of 1, based on events with a 3% oxygen desaturation, is clinically significant.13,15,16
All studies were scored by a single registered polysomnographic technologist who was required to demonstrate a complete understanding of the study’s scoring rules and to articulate reasons for assigning epoch-by-epoch codes for sleep and respiratory scoring. The initial ‘pass’ rate for polysomnograms was 90%; the overall pass rate was 97%. Detailed scoring procedures have been described previously.12 Briefly, a PSG was scored “good” if there were a minimum of 5 or more hours of scorable signal on at least 2 respiratory channels (airflow, thoracic, or abdominal bands), oximetry, and 1 electroencephalogram signal. A score of “fair” was given if at least 4 hours but less than 5 hours of scorable signal were present on at least 1 electroencephalogram, oximeter, and respiratory signal. If an initial study was failed (approximately 10%), the subject was asked to have another sleep recording.
Approximately 5% of studies were rescored by the same scorer on a blinded basis to determine consistency in scoring. No systematic differences were observed between initial and rescored studies. The mean initial RDI for 24 rescored studies was .70, and the mean RDI after rescoring was .77 (p>.622). When these rescored studies were classified as having a RDI < 1 or ≥ 1, blinded scoring resulted in satisfactory agreement with a κ statistic of 0.78. Only 2 studies that had been recorded from our earliest months of enrollment had differences in classification. Furthermore, a night-to-night variability study in 10 children showed no statistically significant differences in key sleep parameters between 2 different nights of recording. The TuCASA protocol was approved by both the University of Arizona Human Subjects Committee and the Tucson Unified School District Research Committee.
Statistical analysis was done using SPSS 11.5 for Windows XP (SPSS, Inc., Chicago, IL). Comparisons of proportions were made using contingency tables with statistical significance (p < .05) determined using the Pearson χ2 test statistic. The Mann-Whitney test was used to compare means for nonparametric data, and the Student t test was used to compare means on normally distributed data. Forward stepwise logistic regression was used to model variables that have previously been shown to be associated with SDB in children, with factor entry into the model set at p ≤ .10. We also calculated the sensitivity, specificity, and positive likelihood ratio for those factors found to be related to SDB alone and in combination. 17
RESULTS
From November 1999 through June 2003, 7055 screening questionnaires were sent home, and 2327 were returned (33%) (Figure 1). The return rate was similar for boys and girls (49.7% and 49.4%) and was higher for Hispanics than Caucasians (45.4% and 38.1%, respectively). Other ethnicities comprised 16.5% of the surveys. Of those returning questionnaires, 1219 (52.4%) supplied recruitment information from whom we selected children to undergo unattended home PSG. The profile of children who participated in the sleep studies was similar to that of nonparticipants in terms of symptoms; however, Hispanic parents were more likely than Caucasian parents to complete the screening survey but opt out of having a PSG for their child.
Figure 1.
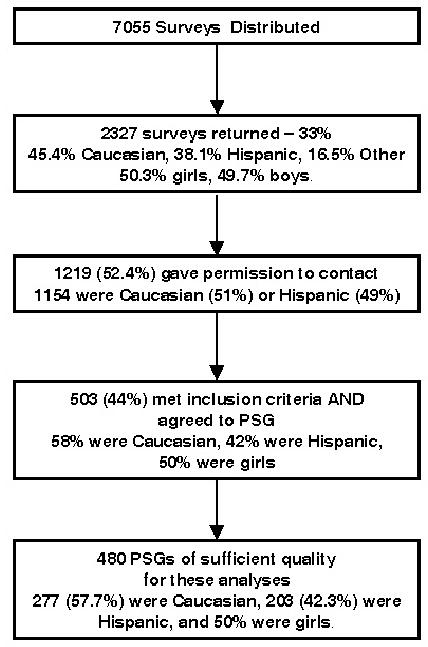
Enrollment algorithm.
A total of 480 PSGs were completed on a sample that was 50.0% female and 42.3% Hispanic (Table 1). The mean age of these children was 8.3 years (SD=1.6), with approximately 53% between the ages of 6 and 8 years. The mean body mass index was 18.0 kg/m2 (SD=4.4); 9.2% were classified as obese because their body mass index exceeded the 95th percentile for their age, sex, and ethnicity.18 Describing the sample in terms of sleep-related symptoms, 15.0% of these children had snoring, 16.3% had report of EDS, 5.2% had witnessed apnea, 29.4% had insomnia, and 5.8% had learning problems. Parental reports also show that 3.5% of these children had sleepwalking, 11.3% had sleep talking, 6.3% had fearful awakenings, and 7.5% had enuresis. Polysomnographic evidence of SDB (RDI ≥ 1) was found in 24% of children (n = 115, mean RDI=2.6, SD=3.4). The mean RDI in children without SDB was 0.38 (SD=0.28). Some common characteristics of sleep architecture and the profile of SDB events in this cohort are shown in Table 2. Except for small differences in percentage of stage 1 sleep and rapid eye movement latency, there were no differences between boys and girls. In addition, there were 57 subjects who spent at least 10% of their total sleep time with O2 saturations < 95%. In contrast, only 7 children spent 1% of total sleep time at O2 saturations < 90%.
Table 1.
Baseline Characteristics
|
Boys (50%) (n = 240) |
Girls (50%) (n = 240) |
Total (N = 480) |
|||||
|---|---|---|---|---|---|---|---|
| No. | % of total* | No. | % of total* | No. | % of total* | ||
| Ethnicity | Caucasian | 129 | 53.8 | 148 | 61.7 | 277 | 57.7 |
| Hispanic | 111 | 45.8 | 92 | 38.3 | 203 | 42.3 | |
| Age, years | 6–8 | 130 | 54.2 | 124 | 51.7 | 254 | 52.9 |
| 9–11 | 110 | 45.8 | 116 | 48.3 | 226 | 47.1 | |
| BMI >95% | Yes | 28 | 11.7 | 16 | 6.6 | 44 | 9.2 |
| No | 212 | 88.3 | 224 | 93.3 | 436 | 90.8 | |
| Frequent Snorer | Yes | 40 | 16.6 | 32 | 13.3 | 72 | 15.0 |
| No | 200 | 83.3 | 208 | 86.7 | 408 | 85.0 | |
| EDS | Yes | 33 | 13.8 | 45 | 18.8 | 78 | 16.3 |
| No | 207 | 86.3 | 195 | 81.3 | 402 | 83.8 | |
| Witnessed Apnea | Yes | 15 | 6.3 | 10 | 4.2 | 25 | 5.2 |
| No | 225 | 93.8 | 230 | 95.8 | 455 | 94.8 | |
| Insomnia | Yes | 76 | 31.7 | 65 | 27.1 | 141 | 29.4 |
| No | 164 | 8.2 | 175 | 72.9 | 339 | 70.6 | |
| Sleepwalking | Yes | 8 | 3.3 | 9 | 3.8 | 17 | 3.5 |
| No | 232 | 96.7 | 231 | 96.3 | 463 | 96.5 | |
| Sleep talking | Yes | 26 | 10.8 | 28 | 11.7 | 54 | 11.3 |
| No | 214 | 89.2 | 212 | 88.3 | 426 | 88.8 | |
| Fearful awakenings | Yes | 15 | 6.3 | 15 | 6.3 | 30 | 6.3 |
| No | 225 | 93.8 | 225 | 93.8 | 450 | 93.8 | |
| Enuresis | Yes | 23 | 9.6 | 13 | 5.4 | 36 | 7.5 |
| No | 217 | 90.4 | 227 | 95.6 | 444 | 92.5 | |
| Airway >2 | Yes | 42 | 17.5 | 39 | 16.3 | 81 | 16.9 |
| No | 198 | 82.5 | 201 | 83.8 | 399 | 83.1 | |
| Learning problems | Yes | 16 | 6.7 | 12 | 5.0 | 28 | 5.8 |
| No | 224 | 93.3 | 228 | 95.0 | 452 | 94.2 | |
| Easily distracted | Yes | 125 | 52.1 | 91 | 37.9 | 216 | 45 |
| No | 115 | 47.9 | 149 | 62.1 | 264 | 55 | |
| Interrupts often | Yes | 124 | 51.7 | 112 | 46.7 | 236 | 49.2 |
| No | 116 | 48.3 | 128 | 53.3 | 244 | 50.8 | |
| Motor running | Yes | 98 | 40.8 | 68 | 28.3 | 166 | 34.6 |
| No | 142 | 59.2 | 172 | 71.7 | 314 | 65.4 | |
| Fidgety | Yes | 119 | 49.6 | 74 | 30.8 | 193 | 40.2 |
| No | 121 | 50.4 | 166 | 69.2 | 287 | 59.8 | |
May not sum to 100% due to rounding. BMI refers to body mass index; EDS, excessive daytime sleepiness.
Table 2.
Sleep and Sleep-Disordered Breathing Event Characteristics in 480 Children
| Sleep Characteristics | Mean | SD | Min | Max | p value | |
|---|---|---|---|---|---|---|
| Time in bed, min | Boy | 538.9 | 86.3 | 276 | 687 | |
| Girl | 546.5 | 85.2 | 275 | 786 | ||
| All | 542.7 | 85.7 | 275 | 786 | .33 | |
| Sleep time, min | Boy | 483.6 | 78.4 | 215 | 634 | |
| Girl | 490.4 | 81.1 | 217 | 744 | ||
| All | 487 | 79.7 | 215 | 744 | .35 | |
| Sleep efficiency, % | Boy | 89.9 | 5.5 | 59.0 | 97.5 | |
| Girl | 89.8 | 6.2 | 52.2 | 97.5 | ||
| All | 89.8 | 5.8 | 52.2 | 97.5 | .90 | |
| Stage 1, % | Boy | 5.0 | 3.6 | 0.5 | 23.8 | |
| Girl | 4.2 | 3.0 | 0.6 | 23.6 | ||
| All | 4.6 | 3.3 | 0.5 | 23.8 | .01 | |
| Stage 2, % | Boy | 52.0 | 6.4 | 34.3 | 69.2 | |
| Girl | 52.1 | 5.9 | 35.3 | 67.9 | ||
| All | 52.0 | 6.1 | 34.3 | 69.2 | .84 | |
| Stage 3/4, % | Boy | 21.8 | 6.3 | 9.2 | 46.2 | |
| Girl | 22.0 | 5.8 | 9.3 | 47.7 | ||
| All | 21.9 | 6.1 | 9.2 | 47.7 | .71 | |
| REM, % | Boy | 21.2 | 5.1 | 5.3 | 32.4 | |
| Girl | 21.7 | 4.8 | 2.3 | 35.0 | ||
| All | 21.5 | 5.0 | 2.3 | 35.0 | .32 | |
| Sleep latency, min | Boy | 17.2 | 18.2 | 0 | 113 | |
| Girl | 19.8 | 23.3 | 0 | 174 | ||
| All | 18.5 | 21.0 | 0 | 174 | .18 | |
| REM latency, min | Boy | 136.6 | 51.3 | 5 | 362 | |
| Girl | 125.1 | 49.6 | 6 | 346 | ||
| All | 130.9 | 50.8 | 5 | 362 | .01 | |
| Respiratory disturbance index | Boy | 0.90 | 1.2 | 0 | 7.4 | |
| Girl | 0.87 | 2.4 | 0 | 29.1 | ||
| All | 0.90 | 1.91 | 0 | 29.1 | .11* | |
| Obstructive apnea index | Boy | 0.01 | 0.03 | 0 | 0.24 | |
| Girl | 0.03 | 0.39 | 0 | 5.9 | ||
| All | 0.02 | 0.27 | 0 | 5.9 | .83* | |
| Central apnea index | Boy | 0.25 | 0.47 | 0 | 4.3 | |
| Girl | 0.30 | 1.1 | 0 | 15.4 | ||
| All | 0.28 | 0.84 | 0 | 15.4 | .91* | |
| Obstructive hypopnea index | Boy | 0.67 | 0.97 | 0 | 6.6 | |
| Time in bed, min | Girl | 0.57 | 1.5 | 0 | 15.8 | |
| All | 0.62 | 1.23 | 0 | 15.8 | .04* |
Mann-Whitney test for non-parametric data. REM refers to rapid eye movement.
Table 3 shows bivariate associations between SDB-related factors and RDI ≥ 1. Boys were more likely than girls to have SDB (p< .01); however, ethnicity (Hispanic vs Caucasian), age category (6–8 years vs 9–11 years), obesity (> 95th percentile), and airway size (3 vs ≤ 2) were not significantly different in children with SDB than those without SDB. The associations between SDB and snoring (29.6% snorers with RDI ≥ 1 versus 10.4% snorers with RDI < 1), EDS (24.3% children report EDS when RDI ≥ 1 versus 13.7% children with EDS when RDI < 1), and learning problems (11.3% with RDI ≥ 1 and learning problems versus 4.1% with RDI < 1 and learning problems) remain very strong, as we have shown previously in a smaller yet representative sample of TuCASA children.14 Witnessed apnea and insomnia were not associated with SDB. Sleepwalking (p< .02) and sleeptalking (p< .006) were also shown to be associated with SDB in children.
Table 3.
Bivariate Associations With a Respiratory Disturbance Index of 1 or Higher
| 95% CI | ||||
|---|---|---|---|---|
| Factor | Unadjusted OR | Lower | Upper | p value |
| Sex, male | 1.70 | 1.11 | 2.61 | .01* |
| Ethnicity | 1.17 | 0.76 | 1.78 | .47 |
| Age, 6–8 years | 1.04 | 0.68 | 1.58 | .86 |
| Obese, BMI ≥ 95 % | 1.55 | 0.79 | 3.03 | .20 |
| Airway size | 1.23 | 0.71 | 2.11 | .46 |
| Snoring | 3.61 | 2.14 | 6.09 | .001* |
| EDS | 2.03 | 1.21 | 3.41 | .007* |
| Witnessed Apnea | 1.85 | 0.80 | 4.31 | .15 |
| Insomnia | 0.96 | 0.60 | 1.52 | .85 |
| Learning Problems | 2.97 | 1.37 | 6.45 | .004* |
| Sleepwalking | 2.96 | 1.11 | 7.85 | .02* |
| Sleeptalking | 2.25 | 1.24 | 4.07 | .006* |
| Enuresis | 1.90 | 0.93 | 3.88 | .08 |
| Fearful Awakenings | 1.39 | 0.62 | 3.13 | .42 |
| Fidgety | 1.25 | 0.82 | 1.91 | .30 |
| Interrupts | 1.48 | 0.97 | 2.25 | .07 |
| Easily Distracted | 1.33 | 0.88 | 2.03 | .18 |
| Motor Running | 0.87 | 0.56 | 1.356 | .53 |
OR refers to odds ratio; CI, confidence interval; BMI, body mass index; EDS, excessive daytime sleepiness.
Logistic regression of all collected potential SDB-related variables resulted in several factors that are predictors for a child having an RDI ≥ 1. These include male sex, frequent loud snoring, EDS, and learning problems. The variables significant at .10 or greater were regressed on RDI ≥ 1 for a final model of predictors for SDB (Table 4). Children with frequent loud snoring were 3.5 times more likely to have SDB than were children who did not snore, and children with EDS and learning problems were also at greater risk for SDB, with odds ratios of 2.1 and 3.0, respectively. Boys were twice as likely as girls to have SDB.
Table 4.
Final Model for Clinical Predictors of Sleep-Disordered Breathing
| 95% CI | ||||
|---|---|---|---|---|
| Factor | Adjusted OR | Lower | Upper | p value |
| Sex | 1.91* | 1.21 | 3.01 | .006 |
| Snoring | 3.55* | 2.04 | 6.20 | .001 |
| EDS | 2.12* | 1.19 | 3.78 | .011 |
| Learning Problems | 3.03* | 1.28 | 7.17 | .012 |
Indicates significant odds ratio (OR) at p ≤ .05. CI refers to confidence interval; EDS, excessive daytime sleepiness.
Table 5 depicts the sensitivity (the probability that the patient has the symptom given that SDB is present [true positives/true positives+false negatives]) and specificity (the probability that the patient does not have the symptom given that SDB is absent [true negatives/true negatives+false positives]) for factors found to be significantly associated with SDB by logistic regression in our sample. None of the characteristics have adequate sensitivity, with male sex (60%) and snoring (29.5%) having the greatest proportion of SDB children with the symptom. Combinations of symptoms have the least sensitivity in terms of identifying children with SDB. However, the specificities of snoring (89.5%), EDS (86.3%), and learning problems (95.9%) were high. Combinations of symptoms such as snoring+male (95.1%), snoring+EDS (97.0%), and snoring+learning problems (98.9%) had specificities that approach 1. Positive likelihood ratios (how much the odds of having SDB increase when the symptom is present) were calculated for the symptoms and combinations of symptoms given above. Increased positive likelihood ratios for snoring (2.8) and symptoms combined with snoring such as snoring+male (3.9), snoring+learning problems (4.0), and snoring+EDS (2.9) were noted. Learning problems alone had a positive likelihood ratio of 2.8.
Table 5.
Sensitivity, Specificity, and Positive Likelihood Ratios
| Factor | Sensitivity | Specificity | Positive Likelihood Ration |
|---|---|---|---|
| Snoring | 29.5 | 89.5 | 2.84 |
| Male | 60.0 | 53.2 | 1.28 |
| EDS | 24.4 | 86.3 | 1.78 |
| Learning problems | 11.3 | 95.9 | 2.75 |
| Snoring + male | 19.1 | 95.1 | 3.88 |
| Snoring + learning problems | 4.4 | 98.9 | 3.97 |
| Snoring + EDS | 8.7 | 97.0 | 2.89 |
| Male + EDS | 10.4 | 94.3 | 1.81 |
| Male + learning problems | 6.1 | 97.5 | 2.47 |
| Obese | 12.2 | 91.8 | 1.48 |
EDS refers to excessive daytime sleepiness.
DISCUSSION
In this study, we have provided evidence from a general population of 6- to 11-year-old Hispanic and Caucasian elementary-school children about risk factors for SDB to enhance decision making in the clinic on whether or not to refer a child for PSG. We found that those children with frequent loud snoring or with parental report of learning problems were 3 times more likely to have SDB than those children who did not snore. Finally, children with EDS or children who are boys were twice as likely to have SDB.
We found that habitual snoring was one of the most important factors associated with SDB in this cohort. Our data are consistent with those from previous studies performed in clinic patients also demonstrating this relationship, as well as with a recent report by Montgomery-Downs and colleagues in a population-based sample.19 However, in contrast to findings from clinical populations, habitual snoring in our cohort had a relatively low sensitivity for SDB. Even with a more liberal definition of snoring that includes “occasional” snoring, snoring in our cohort was still a somewhat insensitive marker of SDB (sensitivity 50.4%). This suggests that, in a general population, there may be a number of children with polysomnographic evidence of SDB who do not snore at least occasionally. Nevertheless, habitual snoring had a high specificity and positive likelihood ratio, indicating that, in habitually snoring children, PSG had a greater probability of being positive. Our findings stand in contrast to those reported by Montgomery-Downs and colleagues, who reported a higher sensitivity and lower specificity for habitual and occasional snoring.19 The younger age range of their population and a slightly different definition of SDB may be explanations for these discrepancies.
Although EDS is a very common symptom of SDB in adults, clinical descriptions of SDB in children have emphasized the paradoxical presence of hyperactive behavior. Our findings suggest that EDS is common symptom associated with SDB in children as well and are consistent with data recently reported by Melendres et al in a clinic population.20 However, similar to habitual snoring, EDS had a low sensitivity but a high specificity and positive likelihood ratio for SDB. Thus, our data indicate that while EDS is not a sensitive surrogate for identification of SDB in the general population, children without SDB are unlikely to have EDS and the presence of EDS increases the odds of finding SDB on a PSG. More striking are the higher specificity and positive likelihood ratio of the combination of EDS and habitual snoring (Table 5), suggesting that a PSG for evaluation of possible SDB may not be necessary for some children. However, these observations require additional confirmation before translation into practice.
Recent studies have implicated SDB as a causative factor in poorer academic achievement.6,21 Our finding that parental report of learning problems is associated with SDB confirms these reports in a large population of children who had PSGs. In addition, our data are consistent with those from a previous analysis of a smaller subset of the TuCASA cohort that documented poorer performance on a multi-trial auditory learning task in children with SDB.22 However, the sensitivity of learning problems for SDB was low and less than that observed for habitual snoring and EDS. Nevertheless, the specificity and positive likelihood ratios were high, suggesting that a PSG is likely to show SDB in children with learning problems. Similar to the combination of habitual snoring and EDS, the high specificity and the positive likelihood ratio of both habitual snoring and learning problems suggests that PSG may be unnecessary for some children in this group as well.
Our analyses generated 3 unexpected findings. First, we observed that boys were slightly more likely than girls to have SDB. Although there is a male sex predilection for SDB in adults, this was not observed in another population-based cohort of children that used cardiorespiratory monitoring to identify SDB.16 However, this latter study included a large number of children who were born prematurely. Most other studies have been performed in clinical populations or have used snoring as a surrogate for SDB. Thus, our finding requires confirmation. In addition, neither the sensitivity nor the specificity of male sex as a predictor of SDB is sufficiently high to have clinical utility. Second, we observed that neither obesity nor estimation of airway size, 2 common physical-examination findings, were predictive of the presence of SDB. Although tonsillectomy leads to resolution of SDB in most children, our data suggest that the presence of significant tonsillar hypertrophy will not be useful in helping clinicians decide on whether or not to order a PSG. Although our estimate of tonsillar size was based on a calibrated estimate, as described in a previous study,23 it is possible that there was insufficient precision to detect an association with SDB. In addition, although obesity in some studies has been associated with an increased risk of SDB,24,25 our data would indicate that any association is not sufficiently robust to be useful as a marker of SDB. Furthermore, it would be consistent with clinical observations that many children with SDB are not obese.26 Finally, we observed small differences between boys and girls in the percentage of stage 1 sleep and rapid eye movement sleep latency. Although they are statistically different, we do not believe they are clinically important.
Several issues related to our identification of SDB events merit comment. First, threshold values for abnormal SDB in children are still not well established. In this study, we defined the presence of SDB as an RDI >1. This definition of SDB is consistent with those used in other studies.15,27 Second, although the RDI in this study included central apneas, central apneas comprised a very small percentage of the overall RDI and thus had little impact on our results. Moreover, reanalysis of our data without the child with the greatest number of central apnea did not alter our conclusions. Finally, the criteria used to identify hypopneas in this study (minimum 30% airflow reduction and 3% oxygen desaturation) are less stringent than the criteria used in some studies. However, there is no standard definition of hypopnea in children, and similar definitions have been used by others.15,16 Furthermore, these criteria, in conjunction with a threshold value of >1 event per hour, have been shown to be associated with an increased prevalence of SDB symptoms.14
We acknowledge that there are some limitations to our study design. First, we performed PSGs in the home. Although we had a high success rate in completing these studies, in some cases, they may not be comparable to a laboratory-based study, thus engendering more variability in our estimates of RDI. However, the size of our cohort and the high quality of most studies suggest that our measurements of RDI are a reasonable assessment of SDB in these children. Second, we did not measure end-tidal CO2 as part of our recording montage because we were performing home-based studies. Thus, it is possible that some cases of obstructive hypoventilation were missed and our prevalence of SDB was underestimated. Third, although we recorded nasal pressure as part of the recording montage, we did not use this physiologic parameter in these analyses. There are very limited data available in children regarding the significance of nasal pressure measurements. In addition, the nasal pressure recording had a relatively higher failure rate. Fourth, our assessments of sleep symptoms are based on parental report. Although the intent of our paper is to incorporate the sleep history that a parent would give to a clinician, it should be stated that parental report of a child’s sleep symptoms could be biased or inaccurate. Finally, our overall prevalence rate of SDB is somewhat higher than that reported in other population-based studies.1,16 We suspect this is related to both an increase in ascertainment from use of a “liberal” definition of SDB, as well as possibly some selection bias on the part of parents agreeing to enroll their child if they suspected problems with sleep. Although a higher rate of SDB may have diminished the sensitivity of some symptoms, such as snoring, to predict the presence of SDB, it nonetheless emphasizes that the absence of such symptoms does not exclude SDB.
In summary, we found that habitual snoring, EDS, and parental report of learning problems are each highly specific but not sensitive for SDB in 6- to 11-year-old children. Although these symptoms were not sensitive predictors for the presence of SDB, they did occur more commonly in children with SDB; thus, PSG may be still be indicated in those with persistent and severe symptoms. Moreover, the specificity and positive likelihood ratio of the combination of some of these symptoms was sufficiently high to suggest that some children may not require a PSG for the diagnosis of SDB.
Acknowledgments
This work was supported by grant HL 62373 from the National Heart Lung and Blood Institute in addition to a grant from the Max and Victoria Dreyfus Foundation. The authors wish to thank the University of Arizona General Clinical Research Center, as well as the principals, teachers, parents, and students from the Tucson Unified School District for their ongoing support of this research.
Footnotes
Disclosure Statement
Drs. Goodwin, Kaemingk, Mulvaney, Morgan, and Quan have indicated no financial conflicts of interest.
References
- 1.Schechter MS. Technical report: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2002;109:e69. doi: 10.1542/peds.109.4.e69. [DOI] [PubMed] [Google Scholar]
- 2.Brouillette R, Hanson D, David R, Klemka L, Hunt C. A diagnostic approach to suspected obstructive sleep apnea in children. J Pediatr. 1984;105:10–4. doi: 10.1016/s0022-3476(84)80348-0. [DOI] [PubMed] [Google Scholar]
- 3.Guilleminault C. Obstructive sleep apnea. Med Clin N Am. 1985;69:1187–203. doi: 10.1016/s0025-7125(16)30982-8. [DOI] [PubMed] [Google Scholar]
- 4.Guilleminault C. Obstructive sleep apnea syndrome in children. In: Guilleminault C, ed. Sleep and its Disorders in Children. New York: Raven; 1987:213–24.
- 5.Carroll J, Loughlin G. Obstructive sleep apnea syndrome in infants and children: clinical features and pathophysiology. In: Kryger M, Ferber R, eds. Principles and Practice of Sleep Medicine in the Child. Philadelphia: WB Saunders; 1995:163–91.
- 6.Gozal D. Sleep-disordered breathing and school performance in children. Pediatrics. 1998;102:616–20. doi: 10.1542/peds.102.3.616. [DOI] [PubMed] [Google Scholar]
- 7.Ali NJ, Pitson D, Stradling JR. Natural history of snoring and related behaviour problems between the ages of 4 and 7 years. Arch Dis Child. 1994;71:74–6. doi: 10.1136/adc.71.1.74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Owens J, Opipari L, Nobile C, Spirito A. Sleep and daytime behavior in children with obstructive sleep apnea and behavioral sleep disorders. Pediatrics. 1998;102:1178–84. doi: 10.1542/peds.102.5.1178. [DOI] [PubMed] [Google Scholar]
- 9.Chervin RD, Archbold KH, Dillon J, et al. Inattention, hyperactivity, and symptoms of sleep-disordered breathing. Pediatrics. 2002;109:449–56. doi: 10.1542/peds.109.3.449. [DOI] [PubMed] [Google Scholar]
- 10.Carroll JL, McColley SA, Marcus CL, Curtis S, Loughlin GM. Inability of clinical history to distinguish primary snoring from obstructive sleep apnea syndrome in children. Chest. 1995;108:610–8. doi: 10.1378/chest.108.3.610. [DOI] [PubMed] [Google Scholar]
- 11.Rosen CL, D’Andrea L, Haddad GG. Adult criteria for obstructive sleep apnea do not identify children with serious obstruction. Am Rev Respir Dis. 1992;146:1231–4. doi: 10.1164/ajrccm/146.5_Pt_1.1231. [DOI] [PubMed] [Google Scholar]
- 12.Goodwin JL, Enright PL, Morgan W, et al. Feasibility of using un-attended polysomnography in children for research: report of the Tucson Children’s Assessment of Sleep Apnea Study (TuCASA) Sleep. 2001;24:937–44. doi: 10.1093/sleep/24.8.937. [DOI] [PubMed] [Google Scholar]
- 13.Goodwin JL, Babar SI, Kaemingk KL, et al. Symptoms related to sleep disordered breathing in Caucasian and Hispanic children - the Tucson Children’s Assessment of Sleep Apnea study (TuCASA) Chest. 2003;124:196–203. doi: 10.1378/chest.124.1.196. [DOI] [PubMed] [Google Scholar]
- 14.Goodwin JL, Kaemingk KL, Fregosi RS, et al. Clinical outcomes associated with sleep-disordered breathing in Caucasian and Hispanic children—The Tucson Children’s Assessment of Sleep Apnea Study (TuCASA) Sleep. 2003;26:587–91. doi: 10.1093/sleep/26.5.587. [DOI] [PubMed] [Google Scholar]
- 15.Huang YS, Chen NH, Li HY, Wu YY, Chao C, Guilleminault C. Sleep disorders in Taiwanese children with attention deficit/hyperactivity disorder. J Sleep Res. 2004;13:269–77. doi: 10.1111/j.1365-2869.2004.00408.x. [DOI] [PubMed] [Google Scholar]
- 16.Rosen CL, Larkin EK, Kirchner HL, et al. Prevalence and risk factors for sleep-disordered breathing in 8–11 year old children: association with race and prematurity. J Pediatr. 2003;142:383–9. doi: 10.1067/mpd.2003.28. [DOI] [PubMed] [Google Scholar]
- 17.Mackinnon A. A spreadsheet for the calculation of comprehensive statistics for the assessment of diagnostic tests and inter-rater agreement. Comput Biol Med. 2000;30:127–34. doi: 10.1016/s0010-4825(00)00006-8. [DOI] [PubMed] [Google Scholar]
- 18.Rosner B, Prineas R, Loggie J, Daniels SR. Percentiles for body mass index in U.S. children 5 to 17 years of age. J Pediatr. 1998;132:211– 22. doi: 10.1016/s0022-3476(98)70434-2. [DOI] [PubMed] [Google Scholar]
- 19.Montgomery-Downs HE, O’Brien LM, Holbrook CR, Gozal D. Snoring and sleep-disordered breathing in young children: subjective and objective correlates. Sleep. 2004;27:87–94. doi: 10.1093/sleep/27.1.87. [DOI] [PubMed] [Google Scholar]
- 20.Melendres MC, Lutz JM, Rubin ED, Marcus CL. Daytime sleepiness and hyperactivity in children with suspected sleep-disordered breathing. Pediatrics. 2004;114:768–75. doi: 10.1542/peds.2004-0730. [DOI] [PubMed] [Google Scholar]
- 21.O’Brien LM, Gozal D. Behavioural and neurocognitive implications of snoring and obstructive sleep apnoea in children: facts and theory. Paediatr Respir Rev. 2002;3:3–9. doi: 10.1053/prrv.2002.0177. [DOI] [PubMed] [Google Scholar]
- 22.Kaemingk KL, Pasvogel AE, Goodwin JL, et al. Learning and memory in children with sleep disordered breathing: findings of the Tucson Children’s Assessment of Sleep Apnea Study (TuCASA) J Int Neuro Physcol Soc. 2003;9:1016–26. doi: 10.1017/S1355617703970056. [DOI] [PubMed] [Google Scholar]
- 23.Brodsky L, Adler E, Stanievich JF. Naso- and oropharyngeal dimensions in children with obstructive sleep apnea. Int J Pediatr Otorhinolaryngol. 1989;17:1–11. doi: 10.1016/0165-5876(89)90288-7. [DOI] [PubMed] [Google Scholar]
- 24.Ng DK, Lam YY, Kwok KL, Chow PY. Obstructive sleep apnoea syndrome and obesity in children. Hong Kong Med J. 2004;10:44– 8. [PubMed] [Google Scholar]
- 25.Morton S, Rosen C, Larkin E, Tishler P, Aylor J, Redline S. Predictors of sleep-disordered breathing in children with a history of tonsillectomy and/or adenoidectomy. Sleep. 2001;24:823–9. doi: 10.1093/sleep/24.7.823. [DOI] [PubMed] [Google Scholar]
- 26.Marcus CL. Sleep-disordered breathing in children. Am J Respir Crit Care Med. 2001;164:16–30. doi: 10.1164/ajrccm.164.1.2008171. [DOI] [PubMed] [Google Scholar]
- 27.Tauman R, Ivanenko A, O’Brien LM, Gozal D. Plasma C-reactive protein levels among children with sleep-disordered breathing. Pediatrics. 2004;113:e564–9. doi: 10.1542/peds.113.6.e564. [DOI] [PubMed] [Google Scholar]