

Abstract
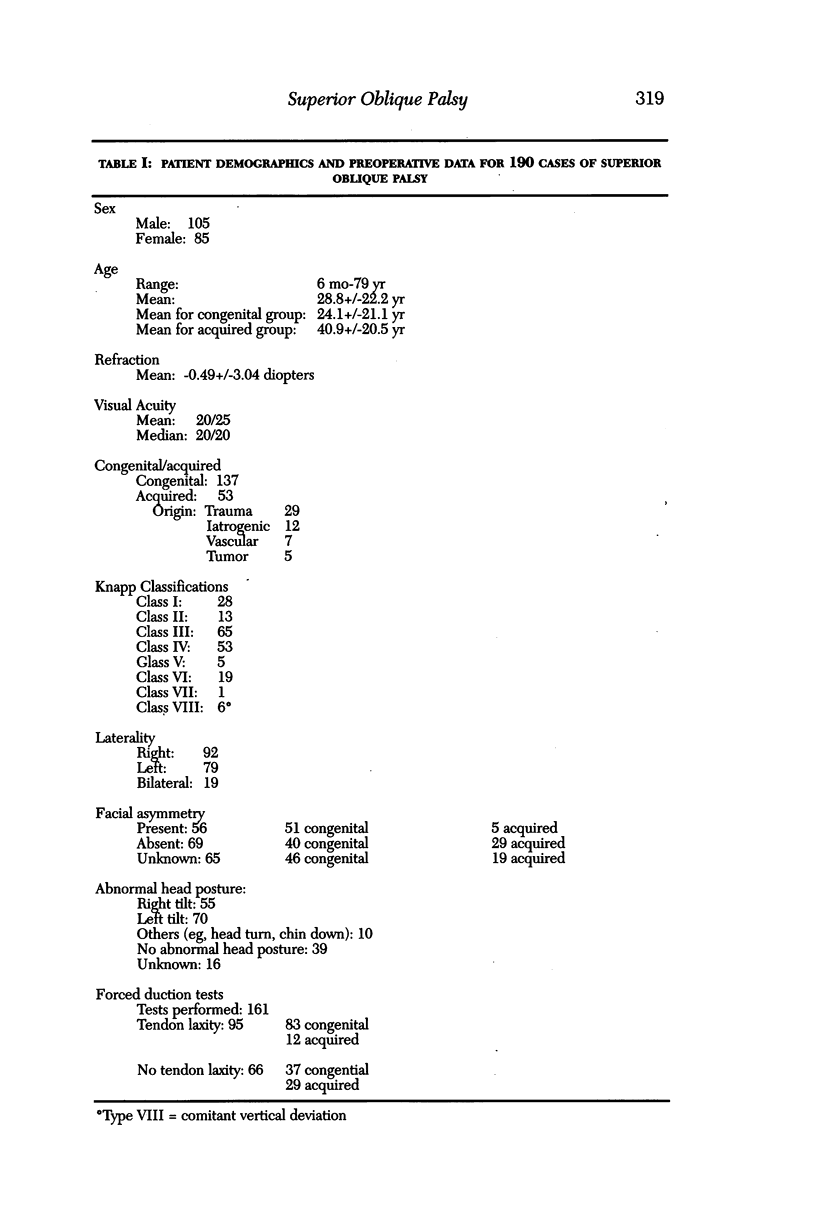
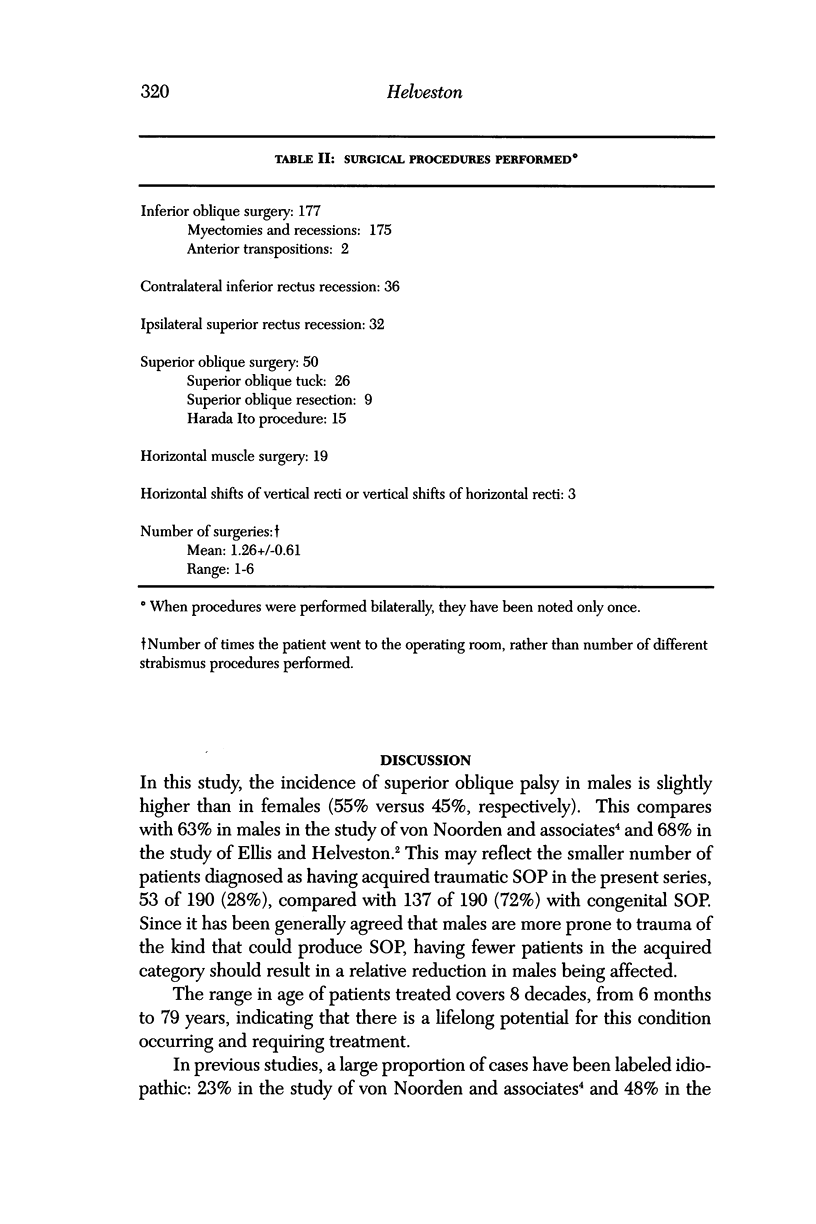
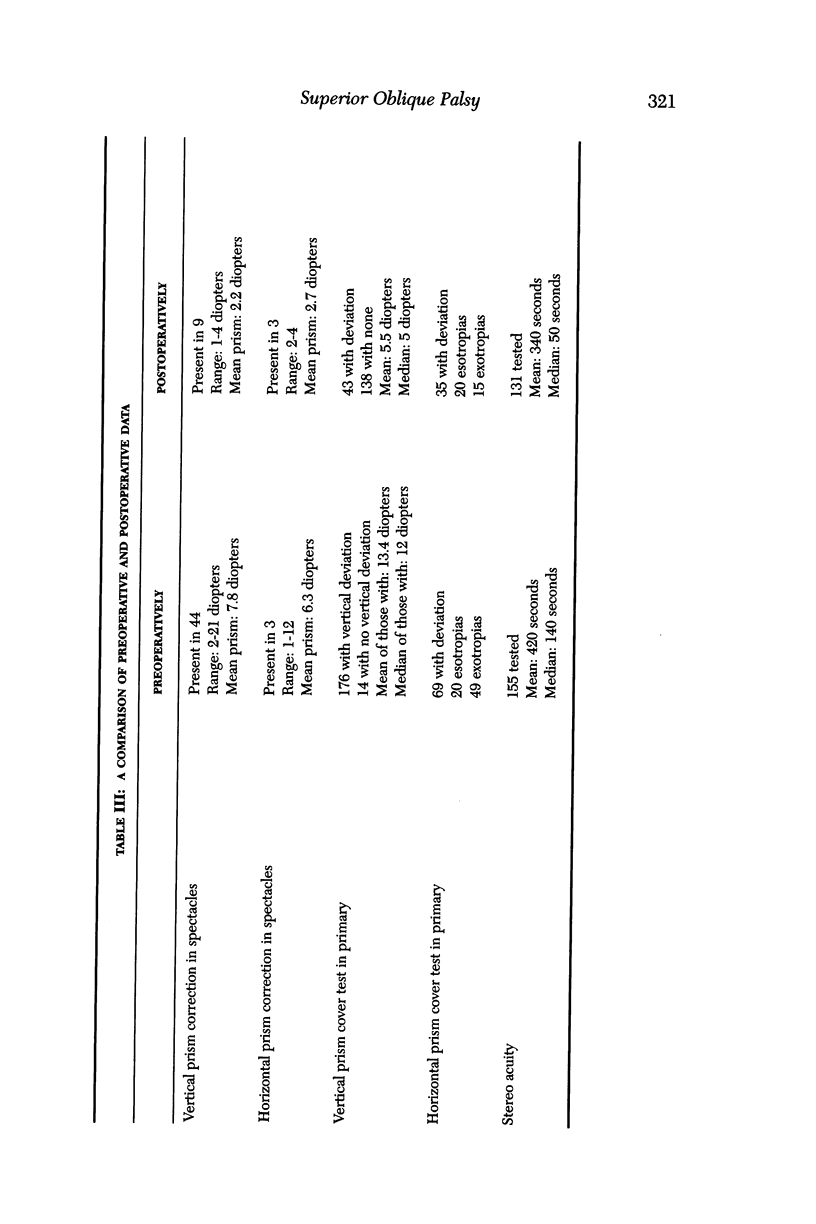
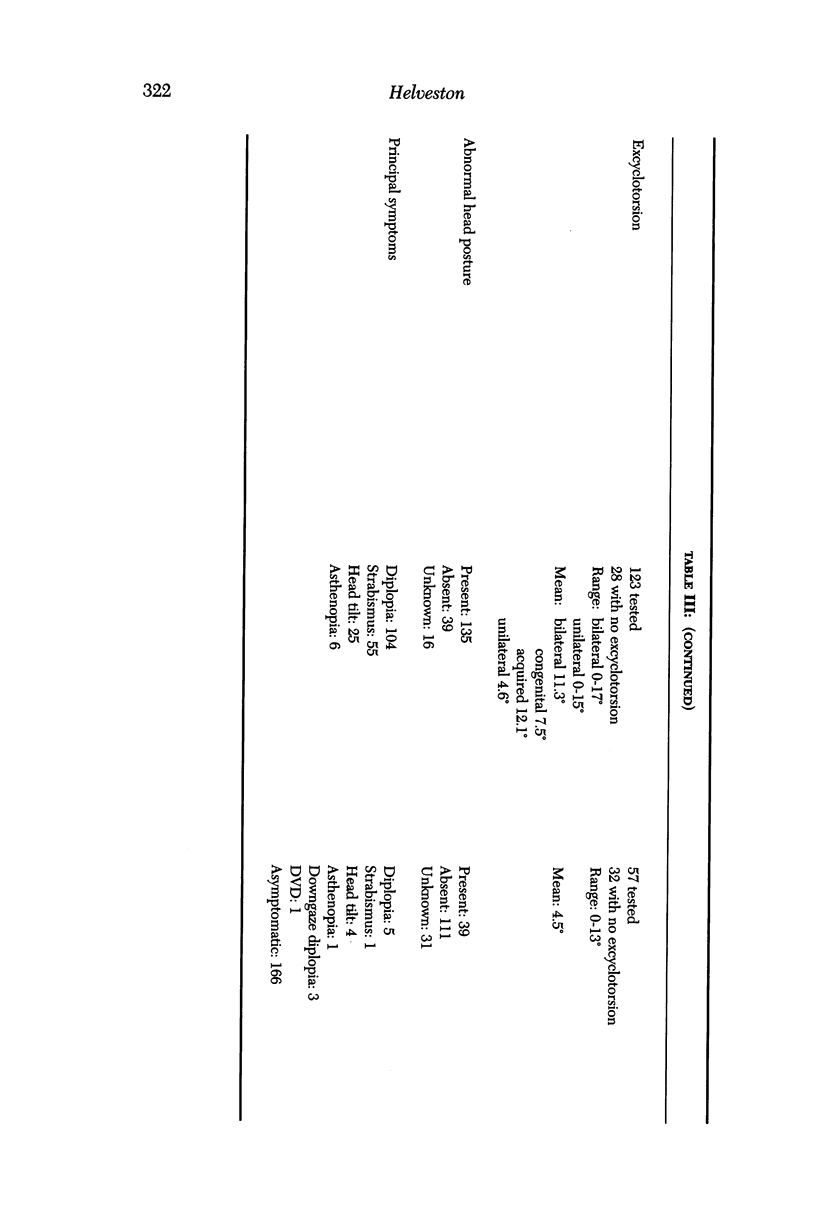
Reports of several large series of patients with superior oblique palsy (SOP) published in 1986 or before set forth important guidelines for both diagnosis and treatment of this condition. Newer information about the anatomy, physiology, and pathophysiology of the superior oblique has accrued over the past decade. This paper reviews our experience with diagnosis and treatment of SOP over the past 5 years in light of this new information. Charts of patients treated for SOP over 5 year (1990 to 1995) were reviewed for male or female sex, age, symptoms, refraction, vision, stereo acuity, head posture, facial asymmetry, intraoperative superior oblique traction test, diagnostic position prism and cover test, torsion, surgery performed, and results of treatment. The charts of 190 patients were reviewed. In 181, postoperative examinations were performed by us. The etiology of the SOP was congenital in 137 and acquired in 53. Twenty-nine acquired cases were due to trauma and 24 arose from other causes. Fifty-six patients had facial asymmetry, 51 of whom had congenital SOP. Ninety-five had a lax tendon, 83 (87%) of whom had congenital SOP. Sixty-six had a normal tendon, 29 (44%) of whom had acquired SOP. Seventy-seven percent of patients had Knapp class I, III, or IV palsy. An average of 1.26 surgeries was performed per patient. Inferior oblique weakening was performed in 177 (93%), while 68 vertical rectus recessions were done. Thirty-five patients had superior oblique tuck or resection, all on lax tendons, and 15 had Harada Ito procedures for torsion. Six patients had mild Brown syndrome postoperatively, none of which required a takedown. A cure, defined as relief of symptoms or elimination of strabismus and head tilt, was achieved in 166 of 181 (92%) of patients. Successful treatment of SOP can be accomplished in the majority of cases by selective surgery usually beginning with inferior oblique weakening plus additional vertical rectus and horizontal surgery as needed, with superior oblique strengthening used only for lax tendons or when torsion is the main problem.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Demer J. L., Miller J. M., Koo E. Y., Rosenbaum A. L. Quantitative magnetic resonance morphometry of extraocular muscles: a new diagnostic tool in paralytic strabismus. J Pediatr Ophthalmol Strabismus. 1994 May-Jun;31(3):177–188. doi: 10.3928/0191-3913-19940501-10. [DOI] [PubMed] [Google Scholar]
- Demer J. L., Miller J. M. Magnetic resonance imaging of the functional anatomy of the superior oblique muscle. Invest Ophthalmol Vis Sci. 1995 Apr;36(5):906–913. [PubMed] [Google Scholar]
- Ellis F. D., Helveston E. M. Superior oblique palsy: diagnosis and classification. Int Ophthalmol Clin. 1976 Fall;16(3):127–135. [PubMed] [Google Scholar]
- Guyton D. L. Exaggerated traction test for the oblique muscles. Ophthalmology. 1981 Oct;88(10):1035–1040. doi: 10.1016/s0161-6420(81)80033-4. [DOI] [PubMed] [Google Scholar]
- Helveston E. M., Ellis F. D. Superior oblique tuck for superior oblique palsy. Aust J Ophthalmol. 1983 Aug;11(3):215–220. [PubMed] [Google Scholar]
- Helveston E. M., Giangiacomo J. G., Ellis F. D. Congenital absence of the superior oblique tendon. Trans Am Ophthalmol Soc. 1981;79:123–135. [PMC free article] [PubMed] [Google Scholar]
- Helveston E. M., Krach D., Plager D. A., Ellis F. D. A new classification of superior oblique palsy based on congenital variations in the tendon. Ophthalmology. 1992 Oct;99(10):1609–1615. doi: 10.1016/s0161-6420(92)31759-2. [DOI] [PubMed] [Google Scholar]
- Helveston E. M., Merriam W. W., Ellis F. D., Shellhamer R. H., Gosling C. G. The trochlea. A study of the anatomy and physiology. Ophthalmology. 1982 Feb;89(2):124–133. doi: 10.1016/s0161-6420(82)34835-6. [DOI] [PubMed] [Google Scholar]
- Helveston E. M., Oberlander M., Evan A., Connors B., Clendenon J. Ultrastrucure of the superior oblique tendon. J Pediatr Ophthalmol Strabismus. 1995 Sep-Oct;32(5):315–316. doi: 10.3928/0191-3913-19950901-11. [DOI] [PubMed] [Google Scholar]
- Hermann J. S. Masked bilateral superior oblique paresis. J Pediatr Ophthalmol Strabismus. 1981 Mar-Apr;18(2):43–48. doi: 10.3928/0191-3913-19810301-10. [DOI] [PubMed] [Google Scholar]
- Knapp P. First Annual Richard G. Scobee Memorial Lecture. Diagnosis and surgical treatment of hypertropia. Am Orthopt J. 1971;21:29–37. [PubMed] [Google Scholar]
- Paysee E. A., Coats D. K., Plager D. A. Facial asymmetry and tendon laxity in superior oblique palsy. J Pediatr Ophthalmol Strabismus. 1995 May-Jun;32(3):158–161. doi: 10.3928/0191-3913-19950501-07. [DOI] [PubMed] [Google Scholar]
- Scott W. E., Kraft S. P. Classification and surgical treatment of superior oblique palsies: I. Unilateral superior oblique palsies. Trans New Orleans Acad Ophthalmol. 1986;34:15–38. [PubMed] [Google Scholar]
- Wilson M. E., Hoxie J. Facial asymmetry in superior oblique muscle palsy. J Pediatr Ophthalmol Strabismus. 1993 Sep-Oct;30(5):315–318. doi: 10.3928/0191-3913-19930901-11. [DOI] [PubMed] [Google Scholar]
- von Noorden G. K., Murray E., Wong S. Y. Superior oblique paralysis. A review of 270 cases. Arch Ophthalmol. 1986 Dec;104(12):1771–1776. doi: 10.1001/archopht.1986.01050240045037. [DOI] [PubMed] [Google Scholar]