

Abstract
Structural equation modeling was used to examine the relationships among stress, social support, negative interaction, and mental health in a sample of African American men and women between ages 18 and 54 (N = 591) from the National Comorbidity Study. The study findings indicated that social support decreased the number of depressive symptoms, did not mitigate the effects of stress, and was reduced in response to financial strain. Financial strain and traumatic events were associated with increased negative interaction with relatives and depressive symptoms. The findings verify that stressful and traumatic events have direct influences on levels of depressive symptoms and affect the quality of social interactions and suggest how social interaction processes contribute to mental health.
Keywords: African Americans, depression, negative interaction, social support
Informal social support networks are important for health and well-being and can be particularly helpful during difficult times. Social interactions involving support network members, however, can also be a source of stress. Recent evidence examining negative social interactions (e.g., criticisms, excessive demands) documents both the costs and benefits of social relationships for mental health (e.g., Lakey, Tardiff, & Drew, 1994; Okun & Keith, 1998; Swindle, Heller, & Frank, 2000). With few exceptions, however, studies on this topic rarely focus on social support and negative interactions within representative samples of African Americans (Lincoln, 2000). The lack of studies on this topic on African Americans and other racial minority groups fosters an assumption of race or ethnic similarity that characterizes a good deal of social science research (Hunt, 1996; Hunt, Jackson, Powell, & Steelman, 2000); that is, social theories and models are conceptually and functionally equivalent across racial and ethnic groups.
The current investigation, drawing on a representative sample of African Americans, uses structural equation modeling to examine the effect of social support and negative interactions on depressive symptoms among African Americans. The study explores whether these constructs mediate the effects of stressful and traumatic events on depressive symptoms. The following sections discuss the relevant literature for this investigation and a conceptual model that depicts the proposed relationships among model constructs.
Informal Social Support Networks of African Americans
The reliance on informal networks as a viable and consistent source of support to African Americans (Taylor, Chatters, & Jackson, 1997) has been attributed both to cultural factors as well as to the social and economic circumstances and barriers faced by African Americans (Billingsley, 1992). Moreover, informal networks have demonstrated their effectiveness as sources of assistance as well as their ability to provide a variety of aid that is used to manage stressful events. Broman (1996) found that African Americans identified informal help as one of the most common coping resources used for a variety of stressful situations, such as economic problems (88.9%) and interpersonal problems involving a spouse or family member (91.7%). Similarly, Neighbors and LaVeist (1989) found that among African Americans, informal network members were the main source of assistance when coping with financial difficulties. Finally, Taylor, Chatters, and Celious (2003) found that informal support networks help their members by providing housing for extended periods of time (6 months or more). Stated reasons for extended family household arrangements included physical illness, family conflict, death of a family member, and monetary problems, and as a way to prevent homelessness following the loss of housing.
Social Support Processes
Social scientists have long theorized about the association between social support and mental health outcomes (Cohen & Wills, 1985; Pearlin, Lieberman, Menaghan, & Mullan, 1981; Wethington & Kessler, 1986). The main effects model (Wheaton, 1985) assumes that social support has a direct effect and serves a health-restorative role by meeting basic human needs for social contact, regardless of the level of stress present. This generalized beneficial effect of social support occurs because social networks provide positive interactions, support, and affirmation that lead to an overall sense of self-worth, self-esteem, and positive affect. Social support has also been studied widely as a psychosocial resource that potentially mitigates or buffers the deleterious psychological effects of stress on mental health outcomes. Cohen and Wills’s theory of the stress process proposes that social support buffers or protects individuals from the deleterious effects of stress. In the event of a stressful situation, supportive network members can variously help individuals reappraise the stressor as something that is within their ability to manage, help provide a solution to the problem, or encourage healthy coping behaviors. Social networks can also help one avoid potentially stressful situations such as financial problems or problematic relationships that would otherwise increase one’s risk of psychological problems.
The process of social stress theory (Pearlin et al., 1981) combines components of stress—the sources, mediators, and manifestations of stress—into a conceptual framework that takes into account both structural and individual factors. The underlying proposition of this theory is that stressful life events (e.g., unemployment, death of a loved one) disrupt an individual’s psychological equilibrium and potentially have adverse effects on mental health outcomes by eroding one’s sense of self. Resources such as social support, however, can intervene in this process to effectively mediate the effects of stress on psychological outcomes. Reflecting the influence of structural factors, the theory suggests that exposure to both stressors and resources is influenced by the social structure (e.g., experiences of racism and discrimination). Accordingly, the hypothesis follows that the relationship between stress and mental health is influenced by differences in social statuses, such as race and socioeconomic status. This is consistent with previously noted findings indicating that African Americans are at higher risk of exposure to stress because of their position in the social structure.
African Americans, Social Support, and Stress
The few studies examining the association between stress, social support, and mental health among African Americans have produced equivocal findings. For example, the Brown, Gary, Greene, and Milburn (1992) study of a community-based sample of 927 African Americans found no beneficial effect of close family ties (e.g., social support) on levels of depressive symptoms. Moreover, family ties did not buffer the influence of chronic economic strain on depressive symptoms (Brown et al., 1992). In contrast, Dressler (1985) found that aspects of extended kinship networks (e.g., number of relatives, perceived social support) buffered the effect of economic stress on depressive symptoms among Black men only. Brown and Gary (1987) found that perceived support buffered the effect of stress on depressive symptoms among women, but not among men. Finally, Neighbors and LaVeist (1989) found that financial assistance from one’s informal support network buffered the influence of economic stress on psychological distress among African Americans, with financial support being particularly beneficial for lower income respondents.
In contrast to normative stressful life events (e.g., financial problems, divorce, illness), traumatic events are major unanticipated and uncontrollable events that are outside the realm of normal human experience (e.g., rape, natural disaster, war). These extreme negative stressors can cause psychological and emotional distress, produce extreme fear or aversion in those who are affected, and can precipitate significant disruptions in individual and social functioning. Of the few studies examining traumatic events among African Americans, most focus primarily on combat experiences. Although these studies use national data (e.g., National Vietnam Veterans Readjustment Study, National Survey of the Vietnam Generation), the specialized nature of the samples (e.g., veterans, Vietnam cohorts) limit their generalizability. Other studies of trauma experienced by African Americans that use small, convenience, or otherwise nonrepresentative samples have similar restrictions.
Despite their limitations, these studies contribute to our current knowledge of trauma among African Americans. For example, the Green, Grace, Lindy, and Leonard (1990) study of racial differences in accounts of experiences during and after the Vietnam War found that Blacks reported higher levels of exposure to stress (e.g., combat, artillery, injury, and exposure to grotesque death), were more likely to report racial tension in their units, and considered racial problems the worst aspect of their Vietnam experience. Blacks were also more likely to report higher rates of childhood trauma (e.g., parental death, severe alcoholism, extreme deprivation), to be disabled or unemployed after the war (despite their higher levels of prewar employment), and to have higher lifetime and current rates of posttraumatic stress disorder (Green et al., 1990). Breslau, Davis, and Andreski (1995) found that African Americans (as compared to Whites) had higher exposure to traumatic events (e.g., attacked or raped, threatened with a weapon, witnessing an injury or murder) and were more likely to report exposure to multiple traumatic events. Moreover, although comparable to Whites in reporting childhood traumatic events, African Americans were more likely to report adulthood traumatic events (Breslau et al., 1995).
Negative Interactions, Social Support, and Mental Health
Research linking social support and mental health among trauma victims (Davidson, Hughes, Blazer, & George, 1991) indicates that access to a supportive network is crucial for recovery. Specifically, victims of trauma who can discuss their feelings with someone are better able to cope with their experience and less likely to experience psychological problems (Wolff & Ratner, 1999). In the absence of social support, however, victims are more likely to blame themselves for the event, have ruminating thoughts, and express their feelings in maladaptive ways, such as anger, withdrawal, or depression. Further, social relationships that are strained, involve social friction and isolation, or discourage discussion of trauma-related feelings, may increase depressive symptoms (Nolen-Hoeksema & Davis, 1999).
Applying these insights to African Americans suggests that, despite the prominence of extended families as an important support resource, continued and prolonged reliance on family members may be burdensome, especially in situations involving financial difficulties or severe trauma. Indeed, repeated requests for assistance from informal helpers “may severely tax support providers and actually diminish potential resources for assistance” (Chatters & Taylor, 1990, p. 89). Neighbors’s study (1997) of informal social support networks among African Americans found that a significant number of interpersonal problems directly involved family members (e.g., spouse, parent, child); a third of these problems explicitly involved a conflict (e.g., marital problems, problems with children). Lincoln, Taylor, and Chatters (2003) found that older African Americans view their informal network as generally supportive and only rarely felt that interactions with family and friends were negative.
Research suggests that social support and negative interactions are distinct dimensions of social relationships that have unique effects on mental health status (Lincoln et al., 2003; Okun & Keith, 1998; Rook, 1990). The majority of studies indicate that, across a variety of samples and indicators, negative interactions have more potent effects on mental health than does social support (Rook, 1984; Swindle et al., 2000). The harmful effects of negative interactions with network members may, in fact, offset or even cancel out the benefits of social support on well-being (see Lakey et al., 1994; Lepore, 1992; Vinokur, Price, & Caplan, 1996, for a different perspective). A recent analysis among Black women (Gray & Keith, 2003) found that negative interactions with family and friends increased psychological distress whereas social support decreased distress. Negative interactions, however, had a stronger effect on distress than did social support.
In sum, although social support is recognized as an important resource that helps individuals confront stressful situations, we know little about the possible role of negative interactions within this context. Further, the lack of research on both social support and negative interactions and their potential influence on the mental health status of African Americans limits our understanding of how these factors function in relation to stressful and traumatic events. Given the prominence of informal social support networks in African American life and this group’s disproportionate exposure to stress, examinations of the relationships among stressors, negative interactions, and social support and their effect on psychological functioning are essential.
The present analysis advances prior research on these topics in several respects. First, research on negative interactions is an emerging area of study, and very little research explores these relations among African Americans. Second, surprisingly few studies of traumatic events focus on this group despite evidence that African Americans are disproportionately exposed to traumatic events of various types (e.g., Breslau et al., 1995; Green et al., 1990). Third, the current investigation’s use of a nationally representative sample of African Americans will allow the generalization of these findings to the population as a whole. Finally, our investigation posits a specific conceptual model and uses structural equation modeling techniques to examine the effects of proposed relationships involving stress, social support, negative interactions, and mental health.
The Proposed Model
Structural equation modeling was used to test the hypothesized relationships among stress (e.g., financial strain, traumatic events), social support, negative interactions, and depressive symptoms. The proposed model (Figure 1) is a reflection of findings from previous studies regarding these relationships. The relationship between stress and social support has been tested in several studies, with mixed results to date. The mediating model suggests that social support offsets the noxious effects of stress on mental health outcomes (Barrera, 1986; Pearlin et al., 1981; Wheaton, 1985). According to this perspective, individuals actively seek assistance from members of their supportive networks in order to avoid or minimize distress. An alternative view suggests that the experience of stress may actually erode social support (Hobfoll, 1985), such that, when faced with stress (i.e., traumatic events or financial problems), affected individuals may withdraw from members of their social networks because of embarrassment or the stigmatizing nature of the stressful situation. Further, network members themselves may withdraw their support or even sever ties with stressed network members (Wortman, 1984), especially if the network is overtaxed. On the basis of these different perspectives and the noted prevalence of stress among African Americans, it is expected that financial strain and traumatic events will be associated with reduced social support and more negative interactions with network members. Financial strain and traumatic events are also expected to increase levels of depressive symptoms.
Figure 1.
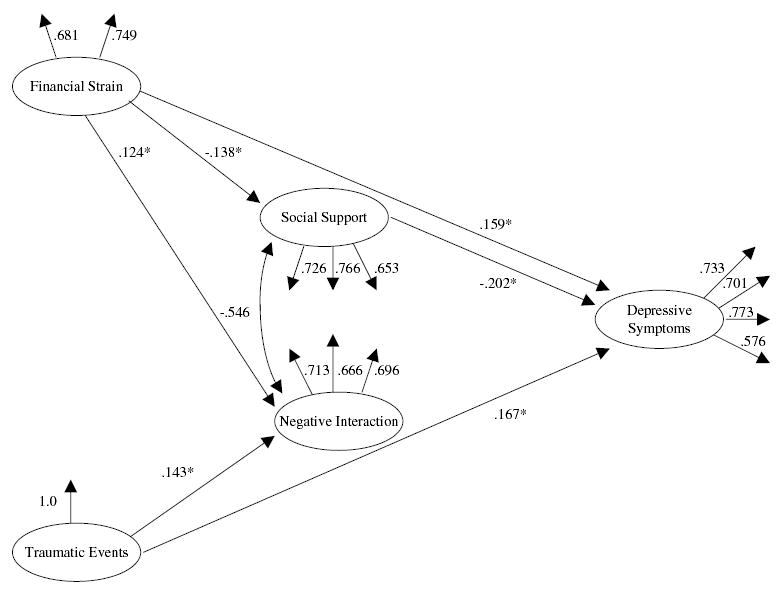
Estimated Model of Social Relations, Stress, and Depressive Symptoms
Social interaction is expected to influence depressive symptoms such that individuals whose network members are understanding, appreciative, and reliable (i.e., provide social support) are expected to experience lower levels of depressive symptoms. Conversely, individuals whose network members make them feel tense, make critical remarks, and get on their nerves (i.e., negative interactions) will experience heightened levels of depressive symptoms.
Method
The National Comorbidity Study was a collaborative epidemiologic investigation designed to study the prevalence and correlates of DSM III-R disorders and patterns and correlates of service utilization. The survey is based on a stratified, multistage area probability sample of persons aged 15–54 years in the noninstitutionalized civilian population in the 48 contiguous states. Interviewing was conducted by the staff of the Survey Research Center at the University of Michigan between September 14, 1990, and February 6, 1992. A total of 8,098 respondents participated in the survey, representing a response rate of 82.4%. The National Comorbidity Study was administered in two parts, each of which took a little more than 1 hour to complete. Part 1 was administered to all 8,098 respondents. Part 2 was administered to a subsample of respondents consisting of persons aged 15–24 years, persons who screened positive for any lifetime diagnosis in Part 1, and a random subsample of other respondents. A total of 5,877 respondents completed Part 2. Many of the items in the present investigation are taken from Part 2 of the survey.
The present analyses are based on the responses of 591 African American respondents between the ages of 18 and 54. The average age of respondents included in the analyses is 32.35 years (SD = 9.83 years). Approximately 58% of the respondents are women; 26% of the respondents are married, 7.6% are separated, 16.1% are divorced, 1.4% are widowed, and 49.1% have never been married. The average number of years of education is 12.86 (SD = 2.06 years); 17.6% of the respondents did not have a high school diploma, whereas 13.5% had at least 4 years of college. With regard to employment status, the majority of the sample (70.2%) are working, and approximately half (49.2%) of the sample report incomes below $20,000. Finally, one third of respondents report living with a spouse or partner (32%) and about 21% live alone. Overall, this subgroup of the National Comorbidity Study compares favorably to Census profiles of the African American population (Kessler et al., 1996).
Table 1 presents the frequency distributions of the items used to develop the constructs in the model. Four indicators are used to measure the major dependent variable, depressive symptoms. These items are generally included in symptom checklists (Almeida & Kessler, 1998; Kessler, Mickelson, & Williams, 1999) and assess the extent to which respondents felt blue, had no interest in things, had trouble concentrating, and felt everything was an effort “during the past 30 days.” The four response categories range from never to often; a high score on these items indicates high levels of depressive symptoms. Financial strain is measured by two indicators that assess whether respondents have enough money to meet their needs (more than need, just enough, not enough) or have difficulty meeting their monthly bills (not at all difficult, not very difficult, somewhat difficult, very difficult). Traumatic events are measured with a 10-item checklist containing major negative events that have happened during the respondents’ lifetime, such as witnessing someone being badly injured or killed, being a victim of rape, being sexually molested, being physically attacked or assaulted, or being threatened with a weapon. Respondents are asked to indicate whether each of these events has happened in their lifetime. The summary score is a count of the number of events experienced.
Table 1.
Social Support, Negative Interaction, Stressful Life Events, and Depressive Symptoms: Frequency Distributions (N = 591)
| N | % | |
|---|---|---|
| Financial strain | ||
| Enough money to meet needs | ||
| More than need | 27 | 4.6 |
| Just enough | 267 | 45.6 |
| Not enough | 292 | 49.8 |
| Difficulty paying monthly bills | ||
| Not at all | 138 | 23.5 |
| Not very | 176 | 30.0 |
| Somewhat | 203 | 34.6 |
| Very | 69 | 11.8 |
| Social support | ||
| Understand way I feel | ||
| Not at all | 33 | 5.6 |
| A little | 110 | 18.8 |
| Some | 211 | 36.0 |
| A lot | 232 | 39.6 |
| Appreciate me | ||
| Not at all | 16 | 2.7 |
| A little | 41 | 7.0 |
| Some | 147 | 25.1 |
| A lot | 382 | 65.2 |
| Can rely on for help | ||
| Not at all | 36 | 6.1 |
| A little | 53 | 9.0 |
| Some | 109 | 18.6 |
| A lot | 388 | 66.2 |
| Depressive symptoms | ||
| Feel blue | ||
| Often | 34 | 5.8 |
| Sometimes | 138 | 23.5 |
| Rarely | 137 | 23.4 |
| Never | 277 | 47.3 |
| No interest in things | ||
| Often | 25 | 4.3 |
| Sometimes | 74 | 12.6 |
| Rarely | 148 | 25.3 |
| Never | 339 | 57.8 |
| Traumatic events | ||
| None | 233 | 39.8 |
| One | 142 | 24.2 |
| Two | 97 | 16.6 |
| Three | 48 | 8.2 |
| Four | 40 | 6.8 |
| Five | 14 | 2.4 |
| Six | 7 | 1.2 |
| Seven | 3 | 0.5 |
| Eight | 2 | 0.3 |
| Negative interaction | ||
| Make me feel tense | ||
| Not at all | 180 | 30.7 |
| A little | 203 | 34.6 |
| Some | 147 | 25.1 |
| A lot | 56 | 9.6 |
| Criticize me | ||
| Not at all | 169 | 28.8 |
| A little | 216 | 36.9 |
| Some | 139 | 23.7 |
| A lot | 62 | 10.6 |
| Get on my nerves | ||
| Not at all | 108 | 18.4 |
| A little | 160 | 27.3 |
| Some | 203 | 34.6 |
| A lot | 115 | 19.6 |
| Have trouble concentrating | ||
| Often | 26 | 4.4 |
| Sometimes | 109 | 18.6 |
| Rarely | 132 | 22.5 |
| Never | 324 | 54.4 |
| Everything an effort | ||
| Often | 56 | 9.6 |
| Sometimes | 145 | 24.7 |
| Rarely | 130 | 22.2 |
| Never | 260 | 43.5 |
Social support is measured by three indicators that were derived from previous measures of affective support (Schuster, Kessler, & Aseltine, 1990; Turner, Frankel, & Levin, 1983). These items assess the extent to which respondents’ relatives (excluding spouse and nonkin) understand the way they feel, appreciate them, and can be relied on for help. Each item has four response categories, ranging from not at all to a lot, with a high score corresponding to higher levels of social support. Negative interaction is measured by three indicators that represent a range of negative social interactions (Abbey, Abramis, & Caplan, 1985; Manne & Zautra, 1989; Ruelman & Karoly, 1991). These items assess the extent to which respondents’ relatives (excluding spouse and nonkin) make them feel tense, criticize them, and get on their nerves. Each item has four response categories, ranging from never to often.
Results
Table 2 presents the means and standard deviations for the variables included in the analyses. Overall, respondents report receiving social support more frequently than experiencing negative interactions. Specifically, they indicate that their relatives made them feel tense (M = 2.13; SD = .96), criticized them (M = 2.17; SD = .95), and got on their nerves (M = 2.55; SD = 1.00) less often, on average, than their relatives understood the way they feel (M = 3.09; SD = .89), appreciate them (M = 3.53; SD = .74), and can be relied on for help (M = 3.46; SD = .89). In terms of stress, respondents report experiencing relatively high levels of financial strain in terms of not having enough money to meet their needs (M = 2.45; SD = .58, range from 1 to 3) and difficulty paying monthly bills (M = 2.34; SD = .96, range from 1 to 4). In contrast, they report few traumatic life events (M = 2.36; SD = 1.56, range from 1 to 8). Finally, respondents indicate having a moderate number of depressive symptoms: feeling blue (M = 1.88; SD = .96), having no interest in things (M = 1.63; SD = .86), having trouble concentrating (M = 1.73; SD = .92), and feeling like everything is an effort (M = 2.00; SD = 1.03).
Table 2.
Social Support, Negative Interaction, Stressful Life Events, and Depressive Symptoms: Means and Standard Deviations (N = 591)
| Variable | M | SD |
|---|---|---|
| Age | 32.35 | 9.83 |
| Education | 12.86 | 2.06 |
| Financial strain | ||
| Enough money to meet needs | 2.45 | .58 |
| Difficulty paying monthly bills | 2.34 | .96 |
| Traumatic events | ||
| Life event summary score | 2.36 | 1.56 |
| Social support | ||
| Understand the way the respondent feels | 3.09 | .89 |
| Appreciate the respondent | 3.53 | .74 |
| Respondent can rely on for help | 3.46 | .89 |
| Negative interaction | ||
| Make the respondent feel tense | 2.13 | .96 |
| Criticize the respondent | 2.17 | .95 |
| Get on the respondent’s nerves | 2.55 | 1.00 |
| Depressive symptoms | ||
| Feel blue | 1.88 | .96 |
| No interest in things | 1.63 | .86 |
| Have trouble concentrating | 1.73 | .92 |
| Everything an effort | 2.00 | 1.03 |
All analyses were conducted using covariance matrices as input and the maximum likelihood estimator in LISREL 8.53 (Jöreskog & Sörbom, 2002) (the standardized factor loadings are presented in Figure 1). These estimates provide information about the psychometric properties of the measures. Although there are no firmly established guidelines regarding cutoff points, researchers generally agree that items above .40 have acceptable psychometric properties. As seen in Figure 1, individual factor loadings were moderate to high in magnitude, ranging from .576 to .773.
Table 3 presents the completely standardized maximum likelihood parameter estimates for the proposed causal model. All analyses control for the effects of age, gender, education, and marital status on these relationships. Respondents who experience more financial strain report lower levels of social support (β = −.138, p < .05) and more negative interaction with relatives (β = .124, p < .05) compared to their counterparts. The experience of traumatic events is also associated with more instances of negative interaction with relatives (β = .143, p < .05) but is unrelated to social support. In contrast to previous findings indicating that negative interactions are a more substantial predictor of depressive symptoms than social support, the present results indicate that social support is associated with fewer depressive symptoms (β = −.202, p < .05). In contrast, negative interactions have no significant effects on depressive symptoms. As expected, respondents who experience traumatic events report more depressive symptoms (β = .167, p < .05, direct effect; β = .185, p < .05, total effect) compared to their counterparts. In addition, financial strain has both direct and indirect effects on depressive symptoms, such that more financial strain increases the number of symptoms (β = .159, p < .05, direct effect; β = .196, p < .05, total effect), in part, by decreasing the level of social support and increasing the level of negative interactions (β = .037, p < .05, indirect effect).
Table 3.
Completely Standardized Maximum Likelihood Parameter Estimates for the Relationships Between Social Support, Negative Interaction, Stressful Life Events, and Depressive Symptomsa (N = 591)
| Dependent Variablesb |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Financial Strain
|
Traumatic Events
|
Social Support
|
Negative Interaction
|
Depressive Symptoms
|
||||||
| Independent Variablesb | B | SE | B | SE | B | SE | B | SE | B | SE |
| Gender (1 = female) | .053 | .071 | −.090* | .129 | .044 | .062 | .176* | .067 | .126* | .067 |
| Age | .121* | .004 | .085* | .007 | .034 | .003 | −.034 | .003 | −.067 | .003 |
| Education | −.291** | .018 | .119* | .031 | .048 | .016 | .050 | .017 | .014 | .016 |
| Marital status (0 = married) | .113 | .083 | .125* | .148 | .004 | .073 | .187* | .078 | .081 | .077 |
| Financial strain | −.138* | .057 | .124* | .060 | .159* | .059 | ||||
| Traumatic events | −.038 | .020 | .143* | .021 | .167* | .021 | ||||
| Social support | −.202* | .079 | ||||||||
| Negative interaction | .073 | .078 | ||||||||
Note: χ2(89, 586) = 125.435; goodness-of-fit index = .975; normed fit index = .958; comparative fit index = .987; root mean square error of approximation = .027; standardized root mean squared residual = .030.
Standardized regression coefficients.
Endogenous factors.
p < .05.
p < .01.
p < .001.
Finally, the coefficients for the effects of the exogenous variables on the latent constructs are provided in Table 4. Women, as compared to men, report fewer traumatic events, more negative interactions with relatives, and more depressive symptoms. Findings for age indicate that older African Americans experience more financial strain and more traumatic events than their younger counterparts. Education is related to financial strain and traumatic events such that persons with higher levels of education report less financial strain, but more traumatic events, compared to their less educated counterparts. Finally, marital status is predictive of stressful events, negative interactions, and depressive symptoms. Compared to married individuals, unmarried persons report both more financial strain and traumatic events, more negative interactions with relatives, and more depressive symptoms.
Table 4.
Completely Standardized Exogenous Effects of the Proposed Model
| Exogenous Constructs
|
||||
|---|---|---|---|---|
| Endogenous Constructs | aGender | Age | Education | bMarital Status |
| Financial strain | ||||
| Direct | .053 | .121* | −.291** | .113* |
| Indirect | .000 | .000 | .000 | .000 |
| Total | .053 | .121* | −.291** | .113* |
| Traumatic events | ||||
| Direct | −.090* | .085* | .119* | .125* |
| Indirect | .000 | .000 | .000 | .000 |
| Total | −.090* | .085* | .119* | .125* |
| Social support | ||||
| Direct | .044 | .034 | .048 | .004 |
| Indirect | −.004 | −.020 | .036 | −.020 |
| Total | .040 | .013 | .084 | −.017 |
| Negative interaction | ||||
| Direct | .176* | −.034 | .050 | .187* |
| Indirect | −.006 | .027* | −.019 | .032* |
| Total | .170* | −.007 | .031 | .219** |
| Depressive symptoms | ||||
| Direct | .126* | −.067 | .014 | .081 |
| Indirect | −.002 | .030 | −.041 | .058* |
| Total | .124* | −.037 | −.027 | .139* |
0 = male, 1 = female.
0 = married, 1 = other.
p < .05.
p < .01.
p < .001.
Discussion
This investigation examined the role of social support and negative interactions in the relationship between stress (i.e., financial strain and traumatic events) and depressive symptoms among a representative sample of African Americans. The findings revealed a number of interesting features regarding the role of social support and negative interactions in the stress process. Although previous studies indicate that the adverse effect of negative interactions on mental health outcomes is more potent than the beneficial effect of social support, these findings indicated that negative interactions were unrelated to depressive symptoms. In contrast, higher levels of social support from network members were associated with fewer depressive symptoms. Contrary to the process of social stress theory (Pearlin et al., 1981) and previous research (Dressler, 1985; Neighbors & LaVeist, 1989), however, social support did not mediate the effects of financial strain or traumatic events in this sample. As predicted by the process of social stress theory, financial strain and traumatic events had adverse effects on mental health status. Social support, however, although effective in decreasing depressive symptoms related to financial strain, was not an effective mediator. It is clear from these findings that financial strain has an especially strong negative effect on social support, which may explain the inability of social support to mediate the effects of financial strain. This particularly potent influence of financial strain on social support may be a reflection of overtaxed kinship-based support networks that are unable to meet the financial needs of individuals. Stressors, such as financial problems, are generally assumed to result in support mobilization rather than erosion or withdrawal. Acute stressors, however, are more likely to result in support mobilization in the short run, whereas chronic stressors may entail serious costs to the social network and thus erode support over time (Krause & Rook, 2003). In the present case, financial difficulties may be of a more chronic nature, involving repeated requests for assistance. Moreover, the higher proportion of kin in the social networks of African Americans (Ajrouch, Antonucci, & Janevic, 2001), and their overall smaller social networks (compared to Whites) (Barnes, Mendes de Leon, Bienias & Evans, 2004), may significantly limit both the availability and range of supportive resources.
The present investigation demonstrated that different types of problematic situations (i.e., financial strain and traumatic events) elicit different responses from social networks. Although persons experiencing traumatic events were just as likely as those with financial difficulties to indicate that they experienced negative interactions with relatives, experiencing economic problems was associated with less social support from relatives. In essence, economic problems were characterized by lower levels of social support, coupled with negative interactions with relatives. In contrast, although traumatic events were associated with increased negative interactions with relatives, persons experiencing them were no different from those who did not with respect to social support from relatives.
The literature suggests that given the greater severity and long-term effects of traumatic events, network members may find it difficult to provide and sustain social support to members who have experienced these events. Further, repeated requests for support may adversely effect ongoing social interactions and generate negative interactions. Our findings partially supported these theoretical speculations, in that the experience of these major traumatic events did not “activate” respondents’ social networks in terms of providing higher levels of social support from relatives (a significant positive coefficient) nor were they associated with lower levels of social support (a significant negative coefficient), which might signify a withdrawal of support. Consistent with theory and previous findings, however, traumatic events were associated with negative interactions with relatives. Future studies should investigate how particular characteristics of stressors may be associated with responses from one’s social network. For example, although on face value traumatic events are severe occurrences, the chronic nature of economic difficulties may be no less important in terms of the quality of interactions with one’s social network.
The direct effect of traumatic events on depressive symptoms is consistent with previous studies (Breslau et al., 1995) and further demonstrates the extreme effect of such events on mental health outcomes. Additionally, the relationship between traumatic events and negative interactions suggests that these stressors have a negative influence on social relations as well as deleterious effects on mental health. As noted earlier, because traumatic events were not associated with social support from relatives, support did not mediate the effects of trauma on depressive symptoms (either attenuating or exacerbating effects).
Interpretation of these findings should be considered within the context of the study’s strengths and limitations. First, the cross-sectional nature of the data limits the ability to determine the temporal order of the constructs. For example, although the model suggests that social support and negative interactions precede depressive symptoms, depressive symptoms may actually distort perceptions of social relationships. Although previous longitudinal analyses support the temporal ordering of the relationships tested here (Rook, 2001), longitudinal data are needed to determine the causal order of the specific constructs examined in this present model. The lack of a mediating effect for social support (i.e., social support mediating the effect of financial strain and traumatic events) may be a reflection of the particular measure or number of items used in this study. It is possible that another type of social support would have produced different results. For example, direct economic assistance (as opposed to emotional support) might mediate the effect of financial strain on depressive symptoms (Neighbors & LaVeist, 1989).
Another limitation involves the referent for the measures of social support and negative interactions. The social support and negative interaction questions are asked about relatives in general (excluding spouse), rather than specific family members. Respondents may receive support from some relatives, but not from others. The multiplex nature of extended families among African Americans poses some challenges to the measures of social support and negative interaction in this sample. Moreover, although not tested in this analysis, it is possible that positive relationships with others such as friends may offset negative relationships with family members.
In conclusion, this study represents an initial attempt to examine the relationships among social status factors, stress, social interactions, and mental health status among African Americans. It incorporates important innovations in addressing these issues including the use of a representative sample of African Americans, structural equation modeling, and measures of negative interactions and traumatic events. Taken as a whole, these findings suggest a number of interesting avenues for future study. First, in keeping with the process of social stress theory, this work highlights the need to identify the sociodemographic factors and conditions under which different types of stress lead to changes in social relations (both social support and negative interactions) among African Americans. Such an approach would allow us to examine the stress process within a context that is fully informed by social structure and to determine how social status factors shape both the experience of stress and the resources available to meet these challenges.
In this study, no significant relationships between negative interaction with relatives and depressive symptoms were found. It is quite possible, however, that our three indicators failed to capture the full range of psychologically distressing feelings one could experience. Moreover, the limited assessment of social support and negative interactions may have failed to capture the complexities of those experiences as well. Consequently, research should employ a wider range of measures and dimensions of mental health and social interaction. In addition, studies of how African Americans respond and adapt to stressful situations are needed, along with investigations that allow for the systematic assessment of the operation of informal social networks. Finally, the study findings give further credence to the notion that positive and negative aspects of social relationships are distinctive with respect to social factor and stress correlates and predictive relationships with depressive symptoms. These analyses demonstrated that the positive aspects of social relationships (i.e., perceptions of being understood, appreciated, and being able to rely on relatives) were evident across the sample, irrespective of social status. In contrast, however, negative interactions with relatives (i.e., relatives make respondent feel tense, criticize them, and get on their nerves) were only associated with being female and unmarried—social status factors that are most noticeably associated with the existence and quality of social and family roles, expectations, and relationships. Further, both financial strain and traumatic events predicted negative interactions, whereas only financial strain was associated with lower levels of social support. Finally, the findings indicated that social support predicted fewer depressive symptoms, whereas negative interactions were unrelated to this outcome. The collection of findings provides a number of provocative departures from previous research on these issues conducted primarily on White samples. By examining the distinctive and important role of social networks in the lives of African Americans, future studies can gain important insights into social interaction processes and how social networks contribute to mental health.
Note
The data for this study were made available by the Inter-University Consortium for Political and Social Research. The authors bear sole responsibility for the present analysis. The preparation of this manuscript was supported by grants from the Hartford Foundation and the National Institute of Mental Health (K01-MH69923-01) to K.D.L. and grants from the National Institute on Aging to L.M.C., R.J.T., and Ellison (R01-AG18782) and to R.J.T. (P30-AG15281).
Contributor Information
Karen D. Lincoln, University of Washington
Linda M. Chatters, University of Michigan.*
Robert Joseph Taylor, University of Michigan.**.
References
- Abbey A, Abramis DJ, Caplan RD. Effects of different sources of social support and social conflict on emotional well-being. Basic and Applied Social Psychology. 1985;6:111–129. [Google Scholar]
- Ajrouch, K. J., Antonucci, T. C., & Janevic, M. R. (2001, November). Close relationships and social networks: A Black-White comparison Paper presented at the annual meeting of the Gerontological Society of America, Chicago, IL.
- Almeida DM, Kessler RC. Everyday stressors and gender differences in daily distress. Journal of Personality and Social Psychology. 1998;75:670–680. doi: 10.1037//0022-3514.75.3.670. [DOI] [PubMed] [Google Scholar]
- Barnes LL, Mendes de Leon CF, Bienias JL, Evans DA. A longitudinal study of Black-White differences in social resources. Journal of Gerontology: Social Sciences. 2004;59B:S146–S153. doi: 10.1093/geronb/59.3.s146. [DOI] [PubMed] [Google Scholar]
- Barrera M. Distinctions between social support concepts, measures, and models. American Journal of Community Psychology. 1986;14:413–445. [Google Scholar]
- Billingsley, A. (1992). Climbing Jacob’s ladder: Enduring legacy of African American families New York: Simon & Schuster.
- Breslau N, Davis GC, Andreski P. Risk factors for PTSD-related traumatic events: A prospective analysis. American Journal of Psychiatry. 1995;152:529–535. doi: 10.1176/ajp.152.4.529. [DOI] [PubMed] [Google Scholar]
- Broman CL. The health consequences of racial discrimination. Ethnicity and Disease. 1996;6:148–153. [PubMed] [Google Scholar]
- Brown DR, Gary LE. Stressful life events, social support networks and the physical and mental health of urban Black adults. Journal of Human Stress. 1987;13:165–174. doi: 10.1080/0097840X.1987.9936810. [DOI] [PubMed] [Google Scholar]
- Brown DR, Gary LE, Greene AD, Milburn NG. Patterns of social affiliation as predictors of depressive symptoms among urban Blacks. Journal of Health and Social Behavior. 1992;33:242–253. [PubMed] [Google Scholar]
- Chatters, L. M., & Taylor, R. J. (1990). Social integration. In Z. Havel, E. A. McKinney, & M. Williams (Eds.), Black aged: Understanding diversity and service needs (pp. 82–99). Newbury Park, CA: Sage.
- Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychological Bulletin. 1985;98:310–357. [PubMed] [Google Scholar]
- Davidson JRT, Hughes D, Blazer D, George LK. Post-traumatic stress disorder in the community: An epidemiological study. Psychological Medicine. 1991;21:713–721. doi: 10.1017/s0033291700022352. [DOI] [PubMed] [Google Scholar]
- Dressler WW. Extended family relationships, social support, and mental health in a Southern Black community. Journal of Health and Social Behavior. 1985;26:39–48. [PubMed] [Google Scholar]
- Gray, B. A., & Keith, V. (2003). The benefits and costs of social support for African American women. In D. R. Brown & V. M. Keith (Eds.), In and out of our right minds: African American women and mental health (pp. 242–257). New York: Columbia University Press.
- Green BL, Grace MD, Lindy JD, Leonard AC. Race differences in response to combat stress. Journal of Traumatic Stress. 1990;3:379–393. [Google Scholar]
- Hobfoll, S. E. (1985). Limitations of social support in the stress process. In I. G. Sarason & B. R. Sarason (Eds.), Social support: Theory, research, and applications Dordrecht, The Netherlands: Martinus Nijhoff.
- Hunt MO. The individual, society, or both? A comparison of Black, Latino, and White beliefs about the causes of poverty. Social Forces. 1996;75:293–332. [Google Scholar]
- Hunt MO, Jackson PB, Powell B, Steelman LC. Color-blind: The treatment of race and ethnicity in social psychology. Social Psychology Quarterly. 2000;63:352–364. [Google Scholar]
- Jöreskog, K., & Sörbom, D. (2002). LISREL 8.53 and PRELIS 2.30 Chicago: Scientific Software International.
- Kessler RC, Michelson KD, Williams DR. The prevalence, distribution and mental health correlates of perceived discrimination in the United States. Journal of Health and Social Behavior. 1999;40:208–230. [PubMed] [Google Scholar]
- Kessler RC, Nelson CB, McGonagle KA, Liu J, Schwartz M, Blazer DG. Comorbidity of DSM-III-R major depressive disorder in the general population: Results from the U.S. National Comorbidity Survey. British Journal of Psychiatry. 1996;168:17–30. [PubMed] [Google Scholar]
- Krause N, Rook KS. Negative interaction in late life: Issues in the stability and generalizability of conflict across relationships. Journals of Gerontology: Psychological Sciences. 2003;58B:P88–P99. doi: 10.1093/geronb/58.2.p88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lakey B, Tardiff TA, Drew JB. Negative social interactions: Assessment and relations to social support, cognition, and psychological distress. Journal of Social and Clinical Psychology. 1994;13:42–62. [Google Scholar]
- Lepore SJ. Social conflict, social support, and psychological distress: Evidence of cross-domain buffering effects. Journal of Personality and Social Psychology. 1992;63:857–867. doi: 10.1037//0022-3514.63.5.857. [DOI] [PubMed] [Google Scholar]
- Lincoln KD. Social support, negative social interactions, and psychological well-being. Social Service Review. 2000;74:231–252. doi: 10.1086/514478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lincoln KD, Taylor RJ, Chatters LM. Correlates of emotional support and negative interaction among Black Americans. Journals of Gerontology: Social Sciences. 2003;53B:S225–S233. doi: 10.1093/geronb/58.4.s225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manne SL, Zautra AJ. Spouse criticism and support: Their association with coping and psychological adjustment among women with rheumatoid arthritis. Journal of Personality and Social Psychology. 1989;56:608–617. doi: 10.1037//0022-3514.56.4.608. [DOI] [PubMed] [Google Scholar]
- Neighbors, H. W. (1997). Husbands, wives, family, and friends: Sources of stress, sources of support. In R. J. Taylor, J. S. Jackson, & L. M. Chatters (Eds.), Family life in Black America (pp. 227–292). Newbury Park, CA: Sage.
- Neighbors HW, LaVeist TA. Socioeconomic status and psychological distress: The impact of financial aid on economic problem severity. Journal of Primary Prevention. 1989;10:149–165. doi: 10.1007/BF01324970. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Davis CG. “Thanks for sharing that”: Ruminators and their social support networks”. Journal of Personality and Social Psychology. 1999;77:801–814. doi: 10.1037//0022-3514.77.4.801. [DOI] [PubMed] [Google Scholar]
- Okun MA, Keith VM. Effects of positive and negative social exchanges with various sources on depressive symptoms in younger and older adults. Journal of Gerontology: Psychological Sciences. 1998;53B:P4–P20. doi: 10.1093/geronb/53b.1.p4. [DOI] [PubMed] [Google Scholar]
- Pearlin LI, Lieberman MA, Menaghan EG, Mullan JT. The stress process. Journal of Health and Social Behavior. 1981;22:337–356. [PubMed] [Google Scholar]
- Rook KS. The negative side of social interaction: Impact on psychological well-being. Journal of Personality and Social Psychology. 1984;46:1097–1108. doi: 10.1037//0022-3514.46.5.1097. [DOI] [PubMed] [Google Scholar]
- Rook, K. S. (1990). Stressful aspects of older adults’ social relationships: Current theory and research. In M. A. P. Stephens (Ed.), Stress and coping in later-life families (pp. 173–192). New York: Hemisphere.
- Rook KS. Emotional health and positive versus negative social exchanges: A daily diary analysis. Applied Developmental Science. 2001;5:86–97. [Google Scholar]
- Ruelman LS, Karoly P. With a little flak from my friends: Development and preliminary validation of the test of negative social exchange. Psychological Assessment. 1991;3:97–104. [Google Scholar]
- Schuster TL, Kessler RC, Aseltine RH. Supportive interactions, negative interactions, and depressed mood. American Journal of Community Psychology. 1990;18:423–438. doi: 10.1007/BF00938116. [DOI] [PubMed] [Google Scholar]
- Swindle R, Heller K, Frank M. Differentiating the effects of positive and negative social transactions in HIV illness. Journal of Community Psychology. 2000;28:35–50. [Google Scholar]
- Taylor RJ, Chatters LM, Celious A. Extended family households among Black Americans. African American Research Perspectives. 2003;1:133–151. [Google Scholar]
- Taylor, R. J., Chatters, L. M., & Jackson, J. S. (1997). Changes over time in support network involvement among Black Americans. In R. J. Taylor, J. S. Jackson, & L. M. Chatters (Eds.), Family life in Black America (pp. 293–316). Thousand Oaks, CA: Sage.
- Turner, R. J., Frankel, G., & Levin, D. M. (1983). Social support: Conceptualization, measurement, and implications for mental health. In J. R. Greenley & R. G. Simmons (Eds.), Research in community and mental health (pp. 67–111). Greenwich, CT: JAI Press.
- Vinokur AD, Price RH, Caplan RD. Hard times and hurtful partners: How financial strain affects depression and relationship satisfaction of unemployed persons and their spouses. Journal of Personality and Social Psychology. 1996;71:166–179. doi: 10.1037//0022-3514.71.1.166. [DOI] [PubMed] [Google Scholar]
- Wethington E, Kessler RC. Perceived support, received support, and adjustment to stressful life events. Journal of Health and Social Behavior. 1986;27:78–89. [PubMed] [Google Scholar]
- Wheaton B. Models of the stress-buffering functions of coping resources. Journal of Health and Social Behavior. 1985;26:352–364. [PubMed] [Google Scholar]
- Wolff AC, Ratner PA. Stress, social support, and sense of coherence. Western Journal of Nursing Research. 1999;21:182–197. doi: 10.1177/01939459922043820. [DOI] [PubMed] [Google Scholar]
- Wortman CB. Social support and the cancer patient. Cancer. 1984;53:2339–2362. doi: 10.1002/cncr.1984.53.s10.2339. [DOI] [PubMed] [Google Scholar]