

Abstract
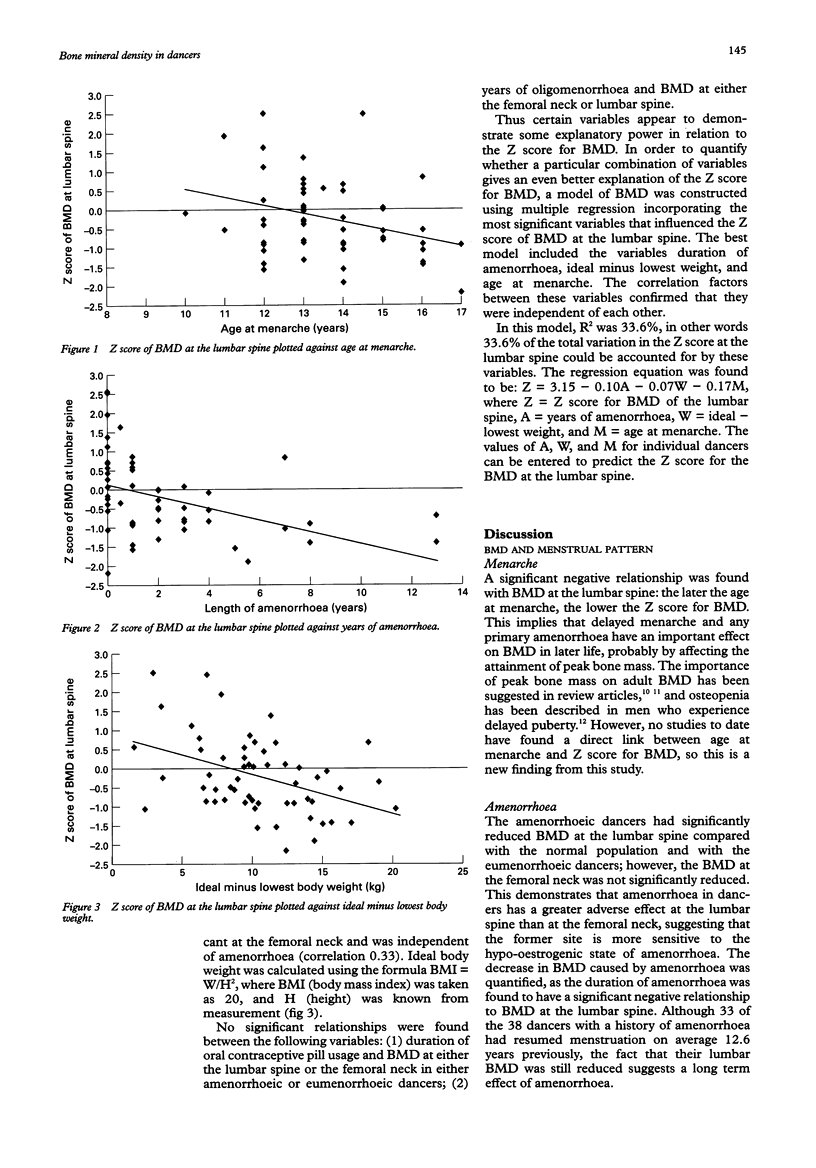
OBJECTIVES: To measure the long term effects of dance training and the contribution of the timing and duration of any menstrual disruption on bone mineral density (BMD). DESIGN: Measurement of BMD in 57 premenopausal, previously professionally dance trained women and the relationship to menstrual and training history. MAIN OUTCOME MEASURES: Bone density measurements at lumbar spine and femoral neck by dual energy x-ray absorptiometry. RESULTS: The average Z score for BMD at the lumbar spine in the amenorrhoeic dancers was significantly below that for the normal population. The average Z score for BMD at the femoral neck in the eumenorrhoeic dancers was significantly above that for the normal population. There was a significant difference between the average Z score for BMD at both the lumbar spine and femoral neck between the amenorrhoeic and eumenorrhoeic dancers. Significant negative relationships were found between BMD at the lumbar spine and (1) age at menarche, (2) duration of amenorrhoea, (3) BMD at the femoral neck, and (4) the variable of ideal minus lowest weight, which was independent of amenorrhoea. No significant relationships were found between duration of oral contraceptive pill usage and BMD at either the lumbar spine or the femoral neck in eumenorrhoeic or amenorrhoeic dancers. In order to quantify the effect of a combination of these significant factors, a model of BMD was constructed using multiple regression incorporating the variables duration of amenorrhoea, age at menarche, and ideal minus lowest body weight. In this model R2 was 33.6%, in other words 33.6% of the total variation in the Z score for BMD at the lumbar spine could be accounted for by these factors. CONCLUSION: Professional female dancers with a history of delayed menarche and amenorrhoea have been identified as another group of premenopausal women potentially at risk of developing osteoporosis because of a decrease in BMD at the lumbar spine. The femoral neck in dancers with a history of amenorrhoea was partially protected from loss of BMD by virtue of being the major weight bearing site in previous dance training, and in eumenorrhoeic dancers BMD was significantly increased at this site.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Compston J. E., Cooper C., Kanis J. A. Bone densitometry in clinical practice. BMJ. 1995 Jun 10;310(6993):1507–1510. doi: 10.1136/bmj.310.6993.1507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper C., Eastell R. Bone gain and loss in premenopausal women. BMJ. 1993 May 22;306(6889):1357–1358. doi: 10.1136/bmj.306.6889.1357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Drinkwater B. L., Nilson K., Chesnut C. H., 3rd, Bremner W. J., Shainholtz S., Southworth M. B. Bone mineral content of amenorrheic and eumenorrheic athletes. N Engl J Med. 1984 Aug 2;311(5):277–281. doi: 10.1056/NEJM198408023110501. [DOI] [PubMed] [Google Scholar]
- Drinkwater B. L., Nilson K., Ott S., Chesnut C. H., 3rd Bone mineral density after resumption of menses in amenorrheic athletes. JAMA. 1986 Jul 18;256(3):380–382. [PubMed] [Google Scholar]
- Finkelstein J. S., Neer R. M., Biller B. M., Crawford J. D., Klibanski A. Osteopenia in men with a history of delayed puberty. N Engl J Med. 1992 Feb 27;326(9):600–604. doi: 10.1056/NEJM199202273260904. [DOI] [PubMed] [Google Scholar]
- Gulekli B., Davies M. C., Jacobs H. S. Effect of treatment on established osteoporosis in young women with amenorrhoea. Clin Endocrinol (Oxf) 1994 Sep;41(3):275–281. doi: 10.1111/j.1365-2265.1994.tb02545.x. [DOI] [PubMed] [Google Scholar]
- Jonnavithula S., Warren M. P., Fox R. P., Lazaro M. I. Bone density is compromised in amenorrheic women despite return of menses: a 2-year study. Obstet Gynecol. 1993 May;81(5 ):669–674. [PubMed] [Google Scholar]
- Karlsson M. K., Johnell O., Obrant K. J. Bone mineral density in professional ballet dancers. Bone Miner. 1993 Jun;21(3):163–169. doi: 10.1016/s0169-6009(08)80227-9. [DOI] [PubMed] [Google Scholar]
- Seeman E. Reduced bone density in women with fractures: contribution of low peak bone density and rapid bone loss. Osteoporos Int. 1994;4 (Suppl 1):15–25. doi: 10.1007/BF01623430. [DOI] [PubMed] [Google Scholar]
- Snow-Harter C. M. Bone health and prevention of osteoporosis in active and athletic women. Clin Sports Med. 1994 Apr;13(2):389–404. [PubMed] [Google Scholar]
- Wilson J. H., Wolman R. L. Osteoporosis and fracture complications in an amenorrhoeic athlete. Br J Rheumatol. 1994 May;33(5):480–481. doi: 10.1093/rheumatology/33.5.480. [DOI] [PubMed] [Google Scholar]
- Wolman R. L. ABC of sports medicine. Osteoporosis and exercise. BMJ. 1994 Aug 6;309(6951):400–403. doi: 10.1136/bmj.309.6951.400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolman R. L., Clark P., McNally E., Harries M., Reeve J. Menstrual state and exercise as determinants of spinal trabecular bone density in female athletes. BMJ. 1990 Sep 15;301(6751):516–518. doi: 10.1136/bmj.301.6751.516. [DOI] [PMC free article] [PubMed] [Google Scholar]