

Abstract
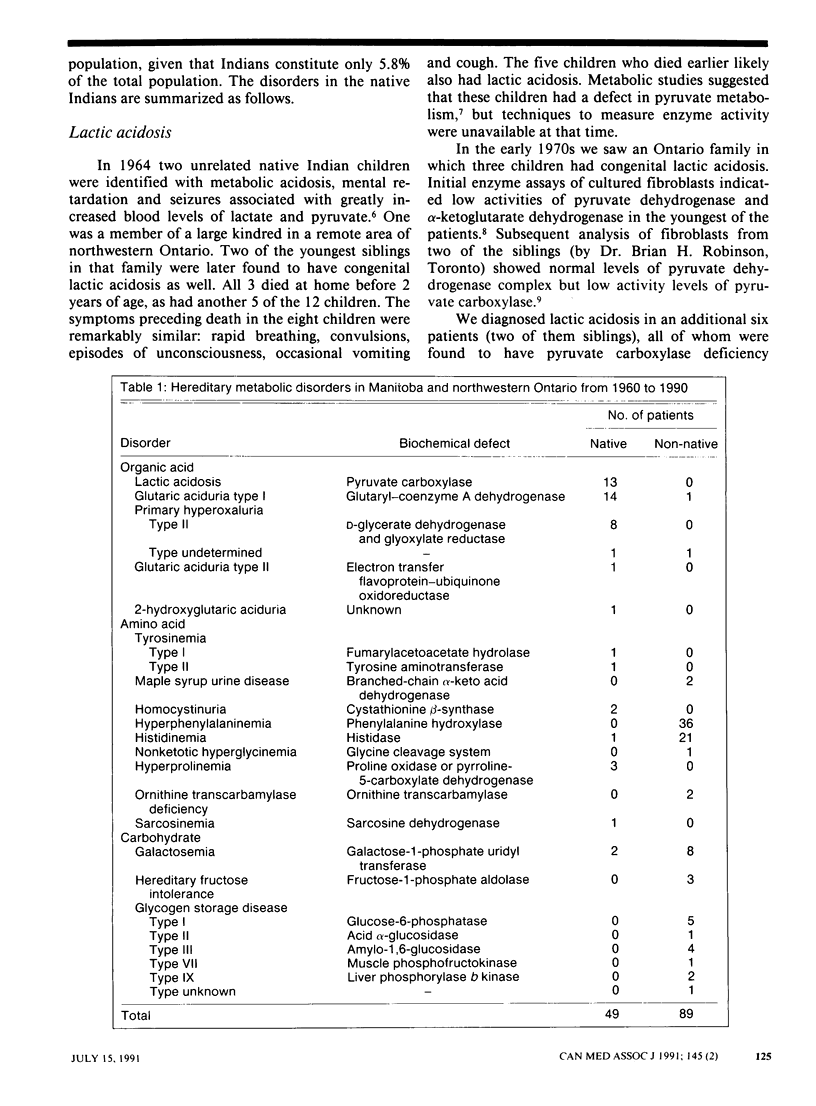
OBJECTIVE: To compare the prevalence of hereditary metabolic diseases in the native and non-native populations of Manitoba and northwestern Ontario. DESIGN: Retrospective analysis. SETTING: Children's Hospital, Winnipeg. PATIENTS: Patients were selected by three methods: laboratory tests designed to screen patients suspected of having a metabolic disease, laboratory investigation of newborn infants with abnormalities detected through screening, and investigation of near relatives of probands with disease. RESULTS: A total of 138 patients with organic acid, amino acid and carbohydrate disorders were seen from 1960 to 1990. Of these, 49 (36%) were native Indians (Algonkian linguistic group). This was in sharp contrast to the proportion of native Indians in the total study population (5.8%). Congenital lactic acidosis due to pyruvate carboxylase deficiency (13 patients), glutaric aciduria type I (14 patients) and primary hyperoxaluria type II (8 patients) were the most common disorders detected. Other rare disorders included glutaric aciduria type II (one patient), 2-hydroxyglutaric aciduria (one patient) and sarcosinemia (one patient). Underreporting, especially of glutaric aciduria type I and hyperoxaluria type II, was likely in the native population. CONCLUSIONS: Hereditary metabolic diseases are greatly overrepresented in the native population of Manitoba and northwestern Ontario. We recommend that native children who present with illnesses involving disturbances of acid-base balance or with neurologic, renal or liver disease of unknown cause by investigated for a possible metabolic disorder.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Chalmers R. A., Tracey B. M., Mistry J., Griffiths K. D., Green A., Winterborn M. H. L-Glyceric aciduria (primary hyperoxaluria type 2) in siblings in two unrelated families. J Inherit Metab Dis. 1984;7 (Suppl 2):133–134. doi: 10.1007/978-94-009-5612-4_41. [DOI] [PubMed] [Google Scholar]
- Duran M., Kamerling J. P., Bakker H. D., van Gennip A. H., Wadman S. K. L-2-Hydroxyglutaric aciduria: an inborn error of metabolism? J Inherit Metab Dis. 1980;3(4):109–112. doi: 10.1007/BF02312543. [DOI] [PubMed] [Google Scholar]
- Enzensberger R., Braun W., July C., Helm E. B., Doerr H. W. Prevalence of antibodies to human herpesviruses and hepatitis B virus in patients at different stages of human immunodeficiency virus (HIV) infection. Infection. 1991 May-Jun;19(3):140–145. doi: 10.1007/BF01643233. [DOI] [PubMed] [Google Scholar]
- Fox J. G. Experience of the Manitoba Perinatal Screening Program, 1965-85. CMAJ. 1987 Nov 15;137(10):883–888. [PMC free article] [PubMed] [Google Scholar]
- Haworth J. C., Booth F. A., Chudley A. E., deGroot G. W., Dilling L. A., Goodman S. I., Greenberg C. R., Mallory C. J., McClarty B. M., Seshia S. S. Phenotypic variability in glutaric aciduria type I: Report of fourteen cases in five Canadian Indian kindreds. J Pediatr. 1991 Jan;118(1):52–58. doi: 10.1016/s0022-3476(05)81843-8. [DOI] [PubMed] [Google Scholar]
- Haworth J. C., Ford J. D., Younoszai M. K. Familial chronic acidosis due to an error in lactate and pyruvate metabolism. Can Med Assoc J. 1967 Sep 23;97(13):773–779. [PMC free article] [PubMed] [Google Scholar]
- Haworth J. C., Miller J. R., Scriver C. R. Screening, counselling and treatment of hereditary metabolic disease; a survey of resources in Canada. Can Med Assoc J. 1974 Nov 16;111(10):1147-50, 1153. [PMC free article] [PubMed] [Google Scholar]
- Haworth J. C., Perry T. L., Blass J. P., Hansen S., Urquhart N. Lactic acidosis in three sibs due to defects in both pyruvate dehydrogenase and alpha-ketoglutarate dehydrogenase complexes. Pediatrics. 1976 Oct;58(4):564–572. [PubMed] [Google Scholar]
- Haworth J. C., Robinson B. H., Perry T. L. Lactic acidosis due to pyruvate carboxylase deficiency. J Inherit Metab Dis. 1981;4(2):57–58. doi: 10.1007/BF02263589. [DOI] [PubMed] [Google Scholar]
- ISRAELS S., HAWORTH J. C., GOURLEY B., FORD J. D. CHRONIC ACIDOSIS DUE TO AN ERROR IN LACTATE AND PYRUVATE METABOLISM. REPORT OF TWO CASES. Pediatrics. 1964 Sep;34:346–356. [PubMed] [Google Scholar]
- Loehr J. P., Goodman S. I., Frerman F. E. Glutaric acidemia type II: heterogeneity of clinical and biochemical phenotypes. Pediatr Res. 1990 Mar;27(3):311–315. doi: 10.1203/00006450-199003000-00024. [DOI] [PubMed] [Google Scholar]
- Moon A., Rhead W. J. Complementation analysis of fatty acid oxidation disorders. J Clin Invest. 1987 Jan;79(1):59–64. doi: 10.1172/JCI112808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perry T. L., Hardwick D. F., Lowry R. B., Hansen S. Hyperprolinaemia in two successive generations of a North American Indian family. Ann Hum Genet. 1968 May;31(4):401–407. doi: 10.1111/j.1469-1809.1968.tb00573.x. [DOI] [PubMed] [Google Scholar]
- Robinson B. H., Oei J., Sherwood W. G., Applegarth D., Wong L., Haworth J., Goodyer P., Casey R., Zaleski L. A. The molecular basis for the two different clinical presentations of classical pyruvate carboxylase deficiency. Am J Hum Genet. 1984 Mar;36(2):283–294. [PMC free article] [PubMed] [Google Scholar]
- Williams H. E., Smith L. H., Jr L-glyceric aciduria. A new genetic variant of primary hyperoxaluria. N Engl J Med. 1968 Feb 1;278(5):233–238. doi: 10.1056/NEJM196802012780502. [DOI] [PubMed] [Google Scholar]
- deGroot G. W., Dakshinamurti K., Allan L., Haworth J. C. Defect in soluble tyrosine aminotransferase in skin fibroblasts of a patient with tyrosinemia. Pediatr Res. 1980 Jul;14(7):896–898. doi: 10.1203/00006450-198007000-00013. [DOI] [PubMed] [Google Scholar]