

Abstract
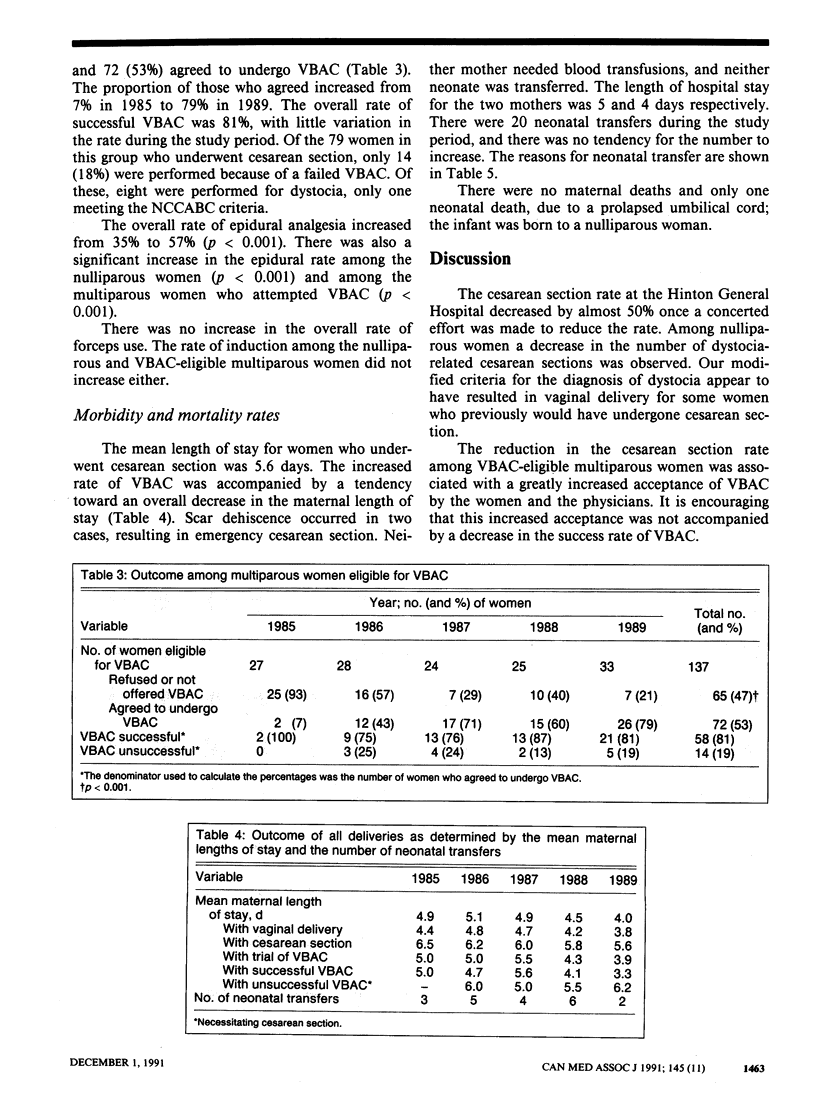
OBJECTIVE: To determine the success of a program designed to reduce the cesarean section rate in a rural community hospital, to identify reasons for any reduction in the rate and to identify any accompanying increases in the maternal and neonatal morbidity and mortality rates. DESIGN: Longitudinal study of modes of delivery. SETTING: A 44-bed community hospital with a medical staff of nine family physicians serving a population of 9000. PATIENTS: All 1161 women who gave birth at the hospital from Jan. 1, 1985, to Dec. 31, 1989. Routinely recorded data were manually extracted from medical charts and entered into a computer database. INTERVENTION: The guidelines of the National Consensus Conference on Aspects of Cesarean Birth (NCCACB) for vaginal birth after cesarean section (VBAC), management of breech presentation and the diagnosis of dystocia requiring cesarean section were introduced at the hospital in 1985. OUTCOME MEASURES: The annual overall cesarean section rates and the rates among nulliparous women, multiparous women eligible for VBAC and multiparous women ineligible for VBAC. RESULTS: The overall cesarean section rate decreased from 23% in 1985 to 13% in 1989 (p = 0.001). Among the nulliparous women the rate decreased from 23% to 12%, but the difference was insignificant (p = 0.069); this decrease was due to a drop in the number of dystocia-related cesarean sections. The rate among VBAC-eligible multiparous women decreased from 93% to 36% (p less than 0.001) because of an increased acceptance of VBAC by the patients and the physicians. The rate among multiparous women ineligible for VBAC was virtually unchanged. There were 20 neonatal transfers to an intensive care unit, with no tendency toward an increase over the study period. None of the mothers died; one newborn, of a nulliparous woman, died from a prolapsed umbilical cord. CONCLUSIONS: The program was accompanied by a significant decrease in the cesarean section rate. Rural hospitals with facilities and personnel for emergency cesarean sections should consider the introduction of a similar program.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anderson G. M., Lomas J. Recent trends in cesarean section rates in Ontario. CMAJ. 1989 Nov 15;141(10):1049–1053. [PMC free article] [PubMed] [Google Scholar]
- Flamm B. L., Lim O. W., Jones C., Fallon D., Newman L. A., Mantis J. K. Vaginal birth after cesarean section: results of a multicenter study. Am J Obstet Gynecol. 1988 May;158(5):1079–1084. doi: 10.1016/0002-9378(88)90224-4. [DOI] [PubMed] [Google Scholar]
- Goldman G., Pineault R., Bilodeau H., Blais R. Effects of patient, physician and hospital characteristics on the likelihood of vaginal birth after previous cesarean section in Quebec. CMAJ. 1990 Nov 15;143(10):1017–1024. [PMC free article] [PubMed] [Google Scholar]
- Mehta C. R., Patel N. R., Tsiatis A. A. Exact significance testing to establish treatment equivalence with ordered categorical data. Biometrics. 1984 Sep;40(3):819–825. [PubMed] [Google Scholar]
- Myers S. A., Gleicher N. A successful program to lower cesarean-section rates. N Engl J Med. 1988 Dec 8;319(23):1511–1516. doi: 10.1056/NEJM198812083192304. [DOI] [PubMed] [Google Scholar]
- Notzon F. C., Placek P. J., Taffel S. M. Comparisons of national cesarean-section rates. N Engl J Med. 1987 Feb 12;316(7):386–389. doi: 10.1056/NEJM198702123160706. [DOI] [PubMed] [Google Scholar]
- Saunders L. D., Flowerdew G. Cesarean sections in Alberta from April 1979 to March 1988. CMAJ. 1991 May 15;144(10):1243-9, 1252. [PMC free article] [PubMed] [Google Scholar]
- van Amerongen D. Vaginal birth after cesarean section. Experience in a community-based practice. J Reprod Med. 1989 Aug;34(8):531–534. [PubMed] [Google Scholar]