

Abstract
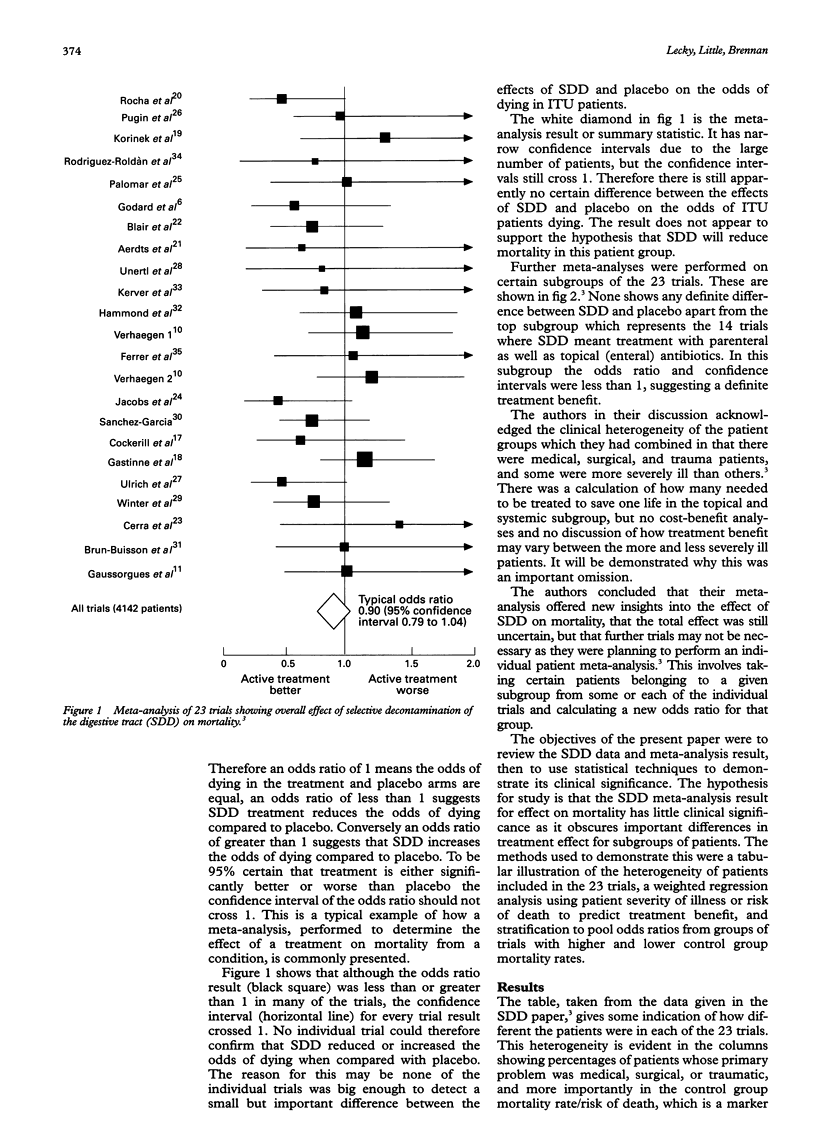
OBJECTIVE: To demonstrate how the results of a meta-analysis can confuse rather than clarify therapeutic dilemmas if clinical heterogeneity among trials is ignored. Then to further discuss the qualities emergency physicians should expect from published meta-analyses if they are to affect clinical practice. SUBJECTS AND METHODS: The data and results were examined from 23 randomised controlled trials of selective decontamination of the digestive tract (SDD), which have been combined in a previous meta-analysis. These were reviewed to take account of clinical heterogeneity, particularly with regard to severity of patient illness. RESULTS: Severity of patient illness predicts degree of reduction in mortality with SDD in a regression analysis: log odds ratio (OR) of death with SDD = -0.0074 - (0.0035 x control group mortality rate), P = 0.017. This is also true when trials are stratified into more and less severely ill patients: pooled OR (a) for CMR > 41% = 0.69 (0.54 to 0.89), with (b) CMR < 3% = 1.02 (0.86 to 1.21). This difference was not suggested by the original meta-analysis result. CONCLUSIONS: Failure to take account of clinical heterogeneity between trials can mean a meta-analysis result ignores important differences in the effect of a treatment on different groups of patients. The discussion indicates how emergency physicians might guard against basing clinical practice on misleading meta-analysis results.
Full text
PDF




Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Egger M., Smith G. D. Misleading meta-analysis. BMJ. 1995 Mar 25;310(6982):752–754. doi: 10.1136/bmj.310.6982.752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eysenck H. J. Meta-analysis and its problems. BMJ. 1994 Sep 24;309(6957):789–792. doi: 10.1136/bmj.309.6957.789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olson C. M. Understanding and evaluating a meta-analysis. Acad Emerg Med. 1994 Jul-Aug;1(4):392–398. doi: 10.1111/j.1553-2712.1994.tb02653.x. [DOI] [PubMed] [Google Scholar]
- Shapiro S. Meta-analysis/Shmeta-analysis. Am J Epidemiol. 1994 Nov 1;140(9):771–778. doi: 10.1093/oxfordjournals.aje.a117324. [DOI] [PubMed] [Google Scholar]
- Smith G. D., Song F., Sheldon T. A. Cholesterol lowering and mortality: the importance of considering initial level of risk. BMJ. 1993 May 22;306(6889):1367–1373. doi: 10.1136/bmj.306.6889.1367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson S. G. Why sources of heterogeneity in meta-analysis should be investigated. BMJ. 1994 Nov 19;309(6965):1351–1355. doi: 10.1136/bmj.309.6965.1351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yusuf S., Flather M. Magnesium in acute myocardial infarction. BMJ. 1995 Mar 25;310(6982):751–752. doi: 10.1136/bmj.310.6982.751. [DOI] [PMC free article] [PubMed] [Google Scholar]