

Abstract
OBJECTIVE: To compare intramuscular glucagon with intravenous glucose in the prehospital management of hypoglycaemia in adults. METHODS: In the first part of the trial all UK ambulance services were asked how their personnel treat prehospital episodes of hypoglycaemia. In the second part, two protocols for treating prehospital hypoglycaemia were studied. In phase 1, intramuscular glucagon 1 mg was used. In phase 2, intravenous glucose 25 g was used; if intravenous access was not possible, intramuscular glucagon was given. RESULTS: 33 out of 43 respondent ambulance services (76.7%) only use glucagon for prehospital hypoglycaemia; the remaining services use glucose and glucagon. In the second part of the study the median duration from diagnosis to full orientation (Glasgow coma score 15) was 28 minutes (95% confidence interval 18 to 49 minutes) in phase 1 and 11 minutes (95% confidence interval 8 to 19 minutes) in phase 2. This difference is statistically significant (P < 0.005). On-scene times were not significantly different. CONCLUSIONS: Intravenous glucose is the treatment of choice in prehospital hypoglycaemia but glucagon should also be available for intramuscular use when intravenous access is not possible.
Full text
PDF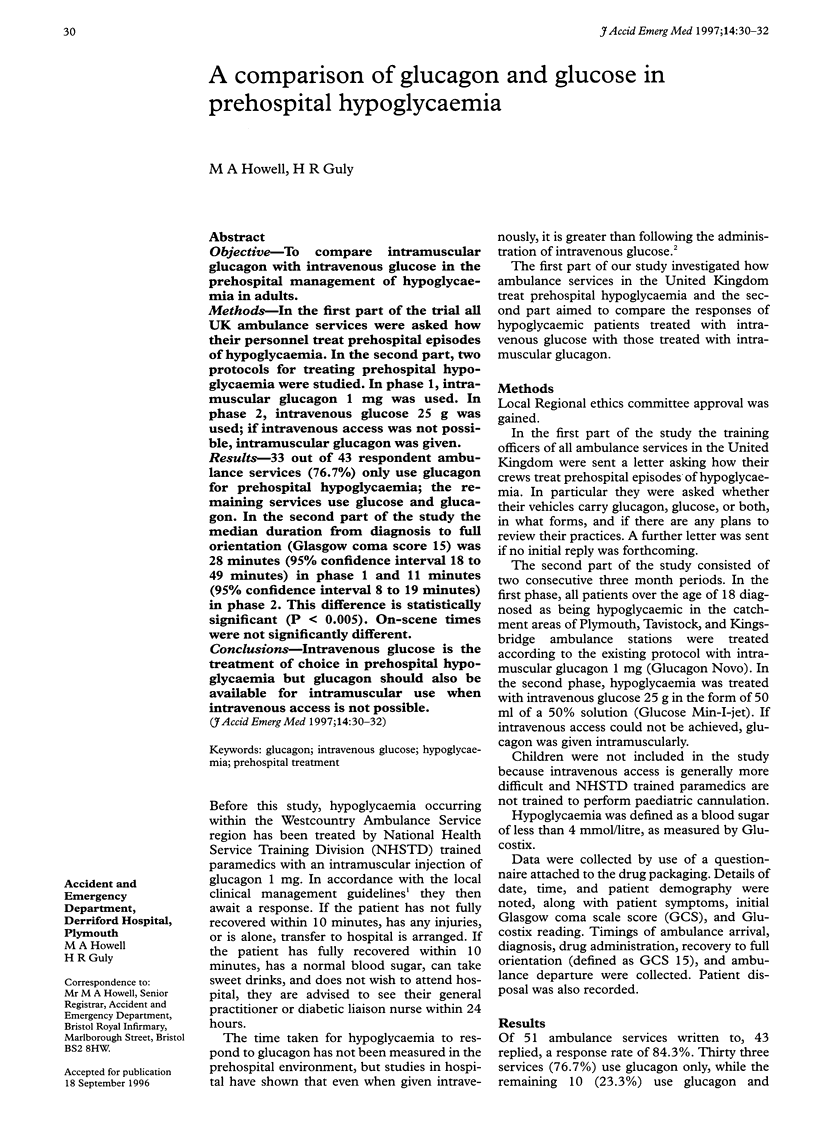
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Collier A., Steedman D. J., Patrick A. W., Nimmo G. R., Matthews D. M., MacIntyre C. C., Little K., Clarke B. F. Comparison of intravenous glucagon and dextrose in treatment of severe hypoglycemia in an accident and emergency department. Diabetes Care. 1987 Nov-Dec;10(6):712–715. doi: 10.2337/diacare.10.6.712. [DOI] [PubMed] [Google Scholar]
- Donovan P. J., Cline D. M., Whitley T. W., Foster C., Outlaw M. Prehospital care by EMTs and EMT-Is in a rural setting: prolongation of scene times by ALS procedures. Ann Emerg Med. 1989 May;18(5):495–500. doi: 10.1016/s0196-0644(89)80831-5. [DOI] [PubMed] [Google Scholar]
- Johnson G. S., Guly H. R. The effect of pre-hospital administration of intravenous nalbuphine on on-scene times. J Accid Emerg Med. 1995 Mar;12(1):20–22. doi: 10.1136/emj.12.1.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones S. E., Nesper T. P., Alcouloumre E. Prehospital intravenous line placement: a prospective study. Ann Emerg Med. 1989 Mar;18(3):244–246. doi: 10.1016/s0196-0644(89)80405-6. [DOI] [PubMed] [Google Scholar]
- McSwain G. R., Garrison W. B., Artz C. P. Evaluation of resuscitation from cardiopulmonary arrest by paramedics. Ann Emerg Med. 1980 Jul;9(7):341–345. doi: 10.1016/s0196-0644(80)80108-9. [DOI] [PubMed] [Google Scholar]
- O'Gorman M., Trabulsy P., Pilcher D. B. Zero-time prehospital i.v. J Trauma. 1989 Jan;29(1):84–86. [PubMed] [Google Scholar]
- Rouse A. Do ambulance crews triage trauma patients? Arch Emerg Med. 1991 Sep;8(3):185–191. doi: 10.1136/emj.8.3.185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weston C., Stephens M. Hypoglycaemic attacks treated by ambulance personnel with extended training. BMJ. 1990 Apr 7;300(6729):908–909. doi: 10.1136/bmj.300.6729.908-a. [DOI] [PMC free article] [PubMed] [Google Scholar]