

Cyclooxygenase-2 (COX-2) inhibitors are a group of nonsteroidal anti-inflammatory drugs (NSAIDs) that may reduce the incidence of gastrointestinal side effects associated with nonselective NSAIDs.1,2 The COX-2 inhibitors celecoxib (Celebrex) and rofecoxib (Vioxx) were first listed on the Ontario Drug Benefit (ODB) formulary on Apr. 17, 2000, as “limited use” products. Limited use means that these products are covered as a benefit only if the prescribing physician completes a form indicating that previous NSAID therapy failed or was not tolerated by the patient or that the patient has a documented history of clinically significant gastrointestinal bleeding or ulcer. This paper provides information on the impact of the ODB listing of COX-2 inhibitors on the costs and quantity of overall NSAID prescriptions and describes some characteristics of patients who received COX-2 inhibitors as compared with those who received nonselective NSAIDs. The analysis uses claims routinely submitted by pharmacies for all prescription drugs provided under the universal ODB plan for elderly patients in Ontario, physician claims submitted to the Ontario Health Insurance Plan (OHIP) and census data.
We used ODB claims data for individuals aged 65 years and older to describe drug use and costs before and after the listing of COX-2 inhibitors. The combined number of prescription claims for COX-2 inhibitors and nonselective NSAIDs increased 68% between March and November 2000, from 44 to 74 per 1000 eligible individuals. Combined monthly expenditures on NSAIDS increased 153% over this period, from $2.3 million to $5.9 million. Time series analysis showed that COX-2 inhibitors were responsible for this growth (Fig. 1). COX-2 inhibitors accounted for 48% of prescriptions and 66% of expenditures for NSAIDs in the post-listing period (Apr. 18 to Nov. 30, 2000).
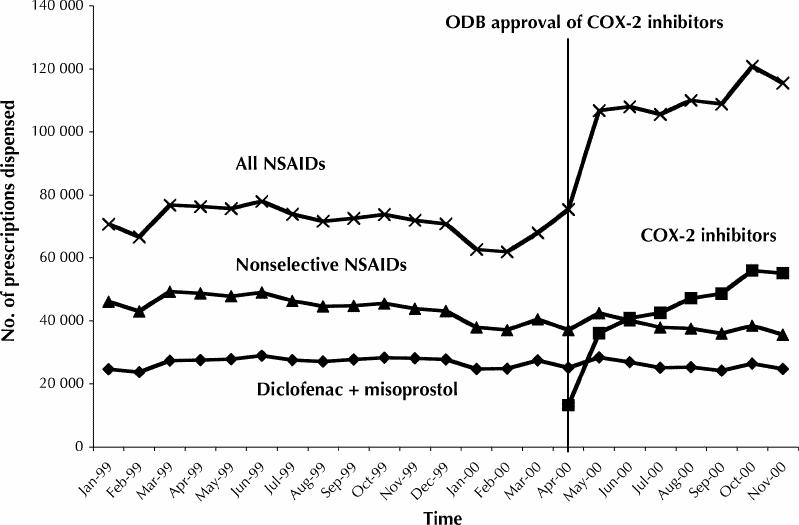
Fig. 1: Prescription use of nonsteroidal anti-inflammatory drugs (NSAIDS) by Ontario residents aged ≥ 65 years before and after initial listing of cyclooxygenase-2 (COX-2) inhibitors. ODB = Ontario Drug Benefit.
We performed a patient-level analysis of a cohort of individuals aged 70 years and older dispensed NSAIDs from Apr. 17, 2000, through July 17, 2000, using ODB claims for the preceding 5-year period to identify previous NSAID use. In addition, we used OHIP claims over the same period to identify previous gastrointestinal endoscopy or upper gastrointestinal radiological examinations as a marker of earlier significant upper gastrointestinal events or ulcers. Users of 3 categories of prescription NSAIDs (COX-2 inhibitors, diclofenac sodium and misoprostol, and other nonselective NSAIDS) were defined on the basis of an index prescription for one of the 3 categories within 90 days following the listing of COX-2 inhibitors. We analyzed differences between groups using the Kruskall–Wallis test for continuous variables and the χ2 test for categorical variables.
About three-quarters of the initial cohort of COX-2 inhibitor users did not have a prescription claim for a nonselective NSAID in the 120 days before their first COX-2 inhibitor prescription, and nearly 20% did not have a prescription for a nonselective NSAID in the previous 5 years. The COX-2 inhibitor users had a similar age distribution to that of patients receiving nonselective NSAIDs. However, about 30% of COX-2 inhibitor users had a claim for an upper gastrointestinal diagnostic examination in the previous 5 years, as compared with about 20% of those patients who were taking nonselective NSAIDs (Table 1).
Table 1
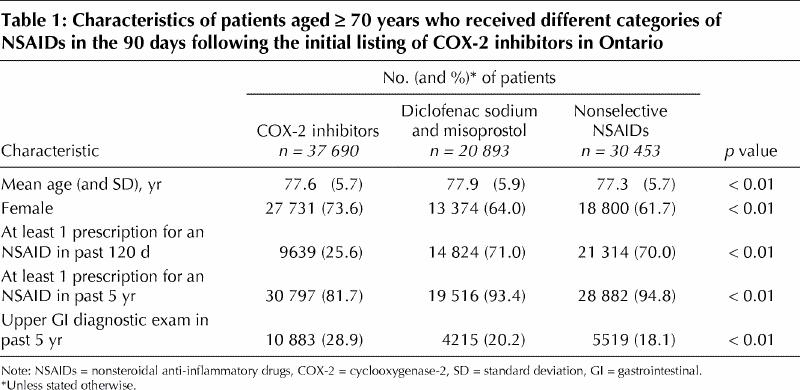
The listing of COX-2 inhibitors had a substantial and immediate impact on expenditures on NSAIDs in Ontario. Although the ODB drug claims used in our analysis did not provide data on over-the-counter NSAID use, it appears that the increase was primarily driven by the use of COX-2 inhibitors in a cohort of patients who were not switched directly from treatment with other less expensive nonselective NSAIDs. A recent cost–effectiveness analysis concluded that COX-2 inhibitors are cost-effective relative to nonselective NSAIDs when used by very elderly patients with an average risk of significant upper gastrointestinal events or ulcers or by younger patients with a high risk of significant upper gastrointestinal events or ulcers.3 The initial cohort of elderly COX-2 inhibitor users in Ontario had a similar age distribution to that of the cohort using nonselective agents. COX-2 inhibitor users were more likely to have a marker of significant earlier gastrointestinal disease, that is, previous gastrointestinal endoscopy or upper gastrointestinal radiological examinations, than other NSAID users. However, the majority did not.
The substantial impact of COX-2 inhibitors on drug expenditures combined with the need for their cost-effective use (by those who are most likely to benefit) will be an important challenge to drug-plan managers and policy- makers. Further research on the clinical characteristics of COX-2 inhibitor users and the effect of COX-2 inhibitor use is warranted.
β See related article page 1131
Footnotes
This article has been peer reviewed.
Contributors: Dr. Mamdani initiated the conception and design of the project, wrote the first draft and contributed to subsequent revisions. Drs. Rochon, Laupacis and Anderson each participated in conception and design. Drs. Rochon and Laupacis contributed to revisions of the text. Dr. Anderson took the lead in revising the first draft of the manuscript. All authors approved the final version.
Competing interests: None declared.
Correspondence to: Dr. Muhammad Mamdani, Institute for Clinical Evaluative Sciences, Rm. G215, 2075 Bayview Ave., Toronto ON M4N 3M5; fax 416 480-6048; muhammad.mamdani@ices.on.ca
References
- 1.Silverstein FE, Faich G, Goldstein JL, Simon LS, Pincus T, Whelton A, et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: a randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA 2000;284:1247-55. [DOI] [PubMed]
- 2.Bombardier C, Laine L, Reicin A, Shapiro D, Burgos-Vargas R, Davis B, et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. N Engl J Med 2000;343:1520-8. [DOI] [PubMed]
- 3.Maetzel A, Krahn M, Naglie G. The cost-effectiveness of celecoxib and rofecoxib in patients with osteoarthritis or rheumatoid arthritis. Ottawa: Canadian Coordinating Office for Health Technology Assessment; 2001. Technology report no. 23.