

A 22-year-old man presented with a low-grade fever, headache and vomiting for 2 months, and 2 days of confusion and disorientation. He was diagnosed with tubercular meningitis after computed tomography (CT) of the cranium (Fig. 1) revealed mild hydrocephalus with dilatation of the third ventricle and the frontal and temporal horns of the lateral ventricles, in addition to mild periventricular ooze around the frontal horns of the lateral ventricles. A lumbar puncture was found to contain 0.64 g/L of protein and 710 white blood cells/mL with 74% lymphocytes. However, no acid-fast bacilli were seen on Ziehl-Neelsen staining. His chest radiograph was normal. He was admitted to hospital and started on antitubercular therapy (rifampicin, isoniazid, ethambutol and pyrazinamide). Although the results of his cardiac examination were unremarkable, an electrocardiogram performed routinely at the time of admission revealed multiple premature ventricular complexes. Two-dimensional echocardiography demonstrated an immobile, sessile mass along the right ventricular free wall (Fig. 2, arrow), which was also seen on the CT scan of the chest (Fig. 3). The patient declined an endomyocardial biopsy. Over the next 3 weeks, the patient became totally oriented and afebrile, and his headaches stopped. He was discharged home on the same 4-drug antitubercular therapy. Repeat echocardiography 6 months later revealed complete resolution of the mass, and his arrythmia was found to be resolved, thus suggesting a diagnosis of tuberculoma of the right ventricle.

Figure 1. Photo: Images courtesy Dr. Amitabh Monga
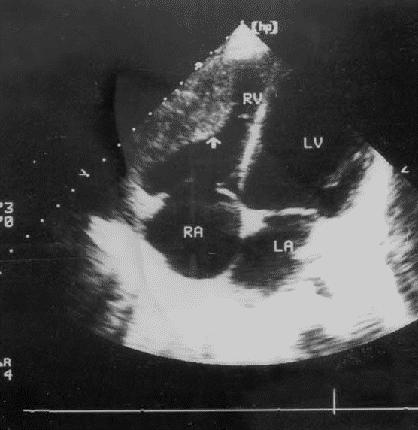
Figure 2. Photo: Images courtesy Dr. Amitabh Monga
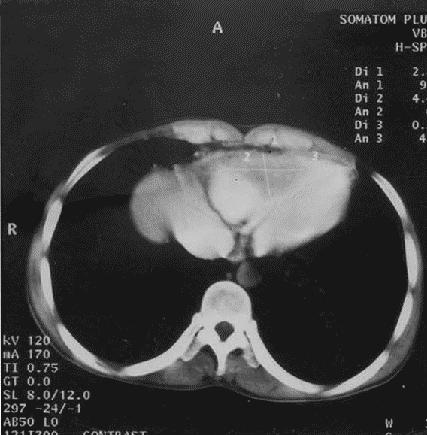
Figure 3. Photo: Images courtesy Dr. Amitabh Monga
Although tuberculosis (TB) primarily involves the lungs, 15%–20% of all cases are extrapulmonary, the most common sites being the lymph nodes, pleura, abdomen and central nervous system.1 Involvement of the heart (apart from the pericardium) is extremely rare and was first reported by Morgagni in 1761.2 Involvement of the myocardium occurs due to direct extension from the pericardium or spread from mediastinal lymph nodes or hematogenous dissemination. Three distinct histological forms of myocardial TB are recognized: diffuse infiltrating (the most common form, characterized microscopically by giant cells and lymphocytes), miliary (resulting from hematogenous spread) and nodular (characterized by central caseation).3,4,5 Ziehl-Neelsen staining of the endomyocardial biopsy specimens often fails to reveal acid-fast bacilli and definitive diagnosis rests on seeing typical histological changes.6 There are no specific features of a tuberculoma on a 2-dimensional echocardiogram or CT scan to distinguish it from other intracardiac masses.
Cardiac tuberculomas have been reported post mortem in fewer than 0.3% of all TB patients.2,7 Isolated cardiac tuberculomas are very rare.8 Single or multiple cardiac tuberculomas are most often observed in the right heart chambers, particularly in the wall of the right atrium. They are usually well circumscribed and sharply demarcated from the surrounding parenchyma. They may erode the underlying myocardium, resulting in ulcers that in turn cause thrombus formation and subsequent embolism. This may also result in hematogenous seeding and disseminated tuberculosis.9 Clinically, tuberculomas may be asymptomatic or may present with arrhythmias,5 complete heart block,8,10 congestive heart failure,11 superior vena caval obstruction,12 right ventricular outflow obstruction,13 aortic insufficiency14 and sudden cardiac death.15 In general, the prognosis is good and, as happened with our patient, resolution of the intracardiac mass and arrhythmias usually occurs after several months of antitubercular treatment.
Although cardiac tuberculomas are rare, they should be suspected in patients with arrhythmias or intracardiac masses who have been exposed to tuberculosis. With timely diagnosis, almost all these patients can be successfully treated with standard antitubercular therapy, though the exact duration of treatment that is required is still unclear.6
Amitabh Monga Anju Arora Ravinder Pal Singh Makkar Ajay K. Gupta Department of Internal Medicine Sitaram Bhartia Institute of Science and Research New Delhi, India
References
- 1.Fanning A. Tuberculosis: 6. Extrapulmonary disease. CMAJ 1999;160:1597-1603. [PMC free article] [PubMed]
- 2.Horn H, Saphir O. The involvement of myocardium in tuberculosis: a review of literature and a report of three cases. Am Rev Tuber 1935; 32: 492-504.
- 3.Gaultier Y, Alou A, Cenac A, Develoux M, Vetter JM. Tuberculome du coeur. Arch Mal Coeur 1987; 80:1413-6. [PubMed]
- 4.Baretti R, Eckel L, Beyersdorf F. Submitral left ventricular tuberculoma. Ann Thorac Surg 1995; 60 (1):81-2. [PubMed]
- 5.O'Neill PG, Rokey R, Greenberg S, Pacifico A. Resolution of ventricular tachycardia and endocardial tuberculoma following antituberculous therapy. Chest 1991;100(5):1467-9. [DOI] [PubMed]
- 6.Schnitzer R. Myocardial tuberculosis with paroxysmal ventricular tachycardia. Br Heart J 1947; 9:213-9. [DOI] [PMC free article] [PubMed]
- 7.Gaultier Y, Alou A, Cenac A, Develoux M, Vetter JM. Tuberculoma of the heart. Contribution of echography. Apropos of a case. Arch Mal Coeur Vaiss 1987;80(9):1413-6. [PubMed]
- 8.Wren C, Stovin PG. Isolated interventricular septal tuberculoma causing complete heart block. Thorax 1982;37(2):149-50. [DOI] [PMC free article] [PubMed]
- 9.Batra R, Trehan V, Salwan R, Krishan A, Nigam M, Malhotra V, et al. Antemortem diagnosis of cardiac tuberculoma. Indian Heart J 1998; 50(1): 87-9. [PubMed]
- 10.Kinare SG, Deshmukh MM. Complete atrioventricular block due to myocardial tuberculosis. Arch Pathol 1969;88:684-7. [PubMed]
- 11.Krishnaswami H, Cherian G. Right atrial tuberculoma: report of a case with complete recovery. Thorax 1984;39(7):550-1. [DOI] [PMC free article] [PubMed]
- 12.Kapoor OP, Mascarenhas E, Rananaware MM, Gadgil RK. Tuberculoma of the heart. Report of 9 cases. Am Heart J 1973;86(3):334-40. [DOI] [PubMed]
- 13.Rawls WJ, ShufordWH, Logan WD, Hurst JW, Schlant RC. Right ventricular outflow tract obstruction produced by a myocardial abscess in a patient with tuberculosis. Am J Cardiol 1968;21: 738-45. [DOI] [PubMed]
- 14.Soyer R, Brunet A, Chevallier B, Leroy J, Morere M, Redonnet M. Tuberculous aortic insufficiency: report of a case with successful surgical treatment. J Thorac Cardiovasc Surg 1981; 82: 254-6. [PubMed]
- 15.Behr G, Palin HC, Temperley JM. Myocardial tuberculosis. BMJ 1977;1:951. [DOI] [PMC free article] [PubMed]