

Abstract
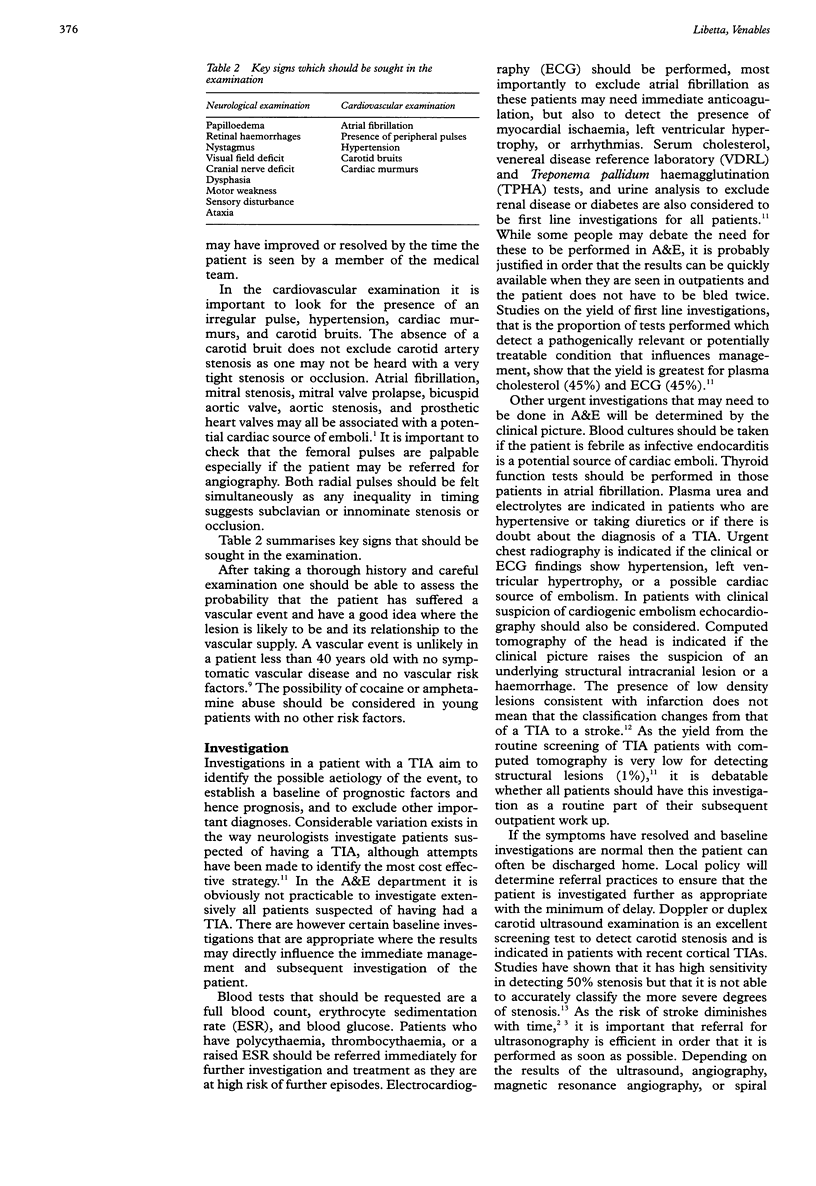
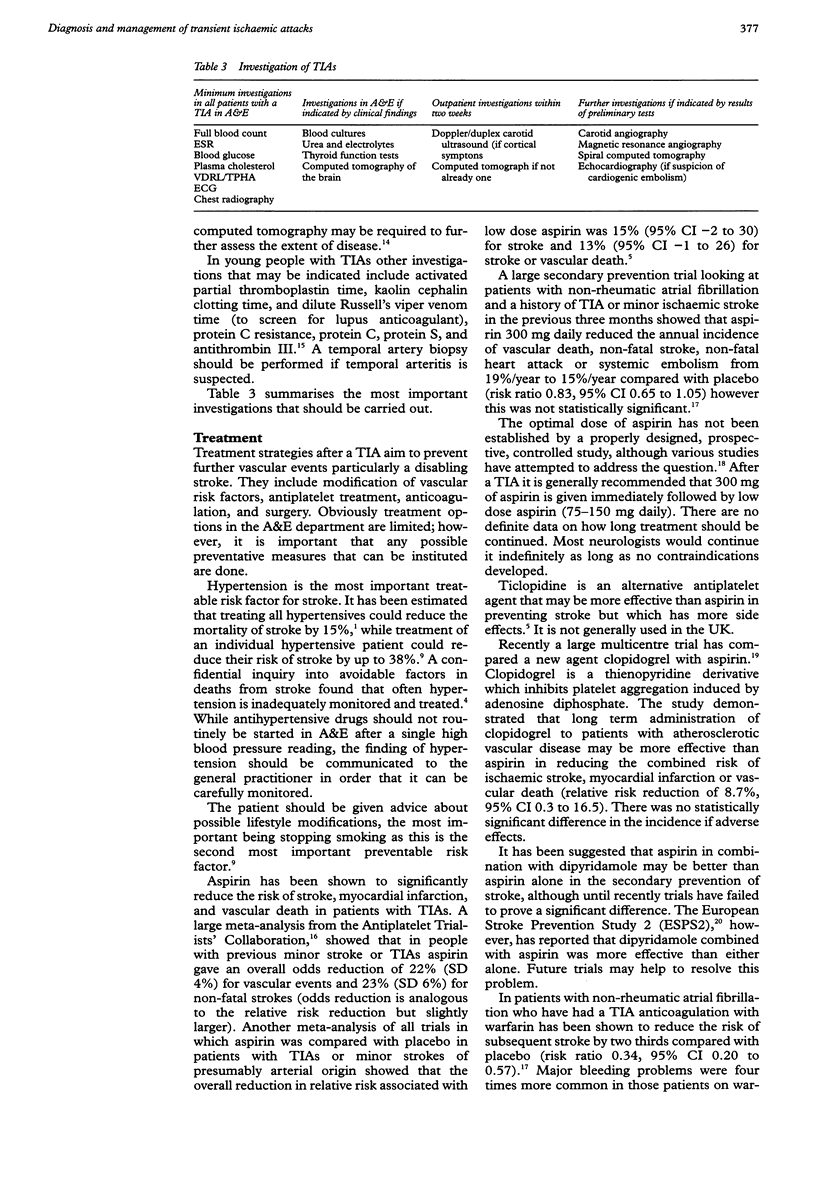
Stroke is an important cause of morbidity and mortality. Often the first presentation of cerebrovascular disease is a TIA which will present to the A&E department. Patients who have had a TIA are at increased risk of stroke, myocardial infarction, and vascular death. The risk of stroke after a TIA is greatest in the first year (approximately 11.6%) with a risk of approximately 5.9% per year over the first five years. As the risk is highest in the first months following a TIA it is important that the patients are diagnosed accurately, investigated promptly, and referred appropriately for treatment in order that valuable time is not lost. For this reason A&E physicians have a valuable role in the initial assessment and management of the patient. It has been advocated that patients should be seen by a neurologist or physician with an interest in cerebrovascular disease within days of their symptoms and be prepared for surgery within two weeks after a TIA. While it is usually not possible to achieve this ideal, improved cooperation between A&E physicians and these neurologists, general physicians, and geriatricians should lead to the implementation of speedy efficient referral procedures which can only improve patient care. When you next see a patient with a TIA in the A&E department remember what they have to lose. Three questions relating to this article are: (1) How are TIAs subdivided and what clinical features allow this differentation? (2) What are the initial investigations that should be performed in A&E? (3) When are the risks of completed stroke greatest after a TIA? Enumerate these risks. How effective is aspirin at reducting this risks?
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Barnett H. J., Eliasziw M., Meldrum H. E. Drugs and surgery in the prevention of ischemic stroke. N Engl J Med. 1995 Jan 26;332(4):238–248. doi: 10.1056/NEJM199501263320408. [DOI] [PubMed] [Google Scholar]
- Dennis M., Bamford J., Sandercock P., Molyneux A., Warlow C. Computed tomography in patients with transient ischaemic attacks: when is a transient ischaemic attack not a transient ischaemic attack but a stroke? J Neurol. 1990 Jul;237(4):257–261. doi: 10.1007/BF00314630. [DOI] [PubMed] [Google Scholar]
- Dennis M., Bamford J., Sandercock P., Warlow C. Prognosis of transient ischemic attacks in the Oxfordshire Community Stroke Project. Stroke. 1990 Jun;21(6):848–853. doi: 10.1161/01.str.21.6.848. [DOI] [PubMed] [Google Scholar]
- Diener H. C., Cunha L., Forbes C., Sivenius J., Smets P., Lowenthal A. European Stroke Prevention Study. 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996 Nov;143(1-2):1–13. doi: 10.1016/s0022-510x(96)00308-5. [DOI] [PubMed] [Google Scholar]
- Greaves M. Coagulation abnormalities and cerebral infarction. J Neurol Neurosurg Psychiatry. 1993 May;56(5):433–439. doi: 10.1136/jnnp.56.5.433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hankey G. J. Transient ischaemic attacks. Med J Aust. 1995 Mar 6;162(5):260–263. [PubMed] [Google Scholar]
- Hankey G. J., Warlow C. P. Cost-effective investigation of patients with suspected transient ischaemic attacks. J Neurol Neurosurg Psychiatry. 1992 Mar;55(3):171–176. doi: 10.1136/jnnp.55.3.171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Humphrey P. R. Management of transient ischaemic attacks and stroke. Postgrad Med J. 1995 Oct;71(840):577–584. doi: 10.1136/pgmj.71.840.577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Intracranial tumours that mimic transient cerebral ischaemia: lessons from a large multicentre trial. The UK TIA Study Group. J Neurol Neurosurg Psychiatry. 1993 May;56(5):563–566. doi: 10.1136/jnnp.56.5.563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kraaijeveld C. L., van Gijn J., Schouten H. J., Staal A. Interobserver agreement for the diagnosis of transient ischemic attacks. Stroke. 1984 Jul-Aug;15(4):723–725. doi: 10.1161/01.str.15.4.723. [DOI] [PubMed] [Google Scholar]
- Lord R. S. Non-invasive testing for cerebrovascular disease. Cardiovasc Surg. 1996 Aug;4(4):424–437. doi: 10.1016/0967-2109(96)00002-6. [DOI] [PubMed] [Google Scholar]
- Payne J. N., Milner P. C., Saul C., Bowns I. R., Hannay D. R., Ramsay L. E. Local confidential inquiry into avoidable factors in deaths from stroke and hypertensive disease. BMJ. 1993 Oct 23;307(6911):1027–1030. doi: 10.1136/bmj.307.6911.1027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sellar R. J. Imaging blood vessels of the head and neck. J Neurol Neurosurg Psychiatry. 1995 Sep;59(3):225–237. doi: 10.1136/jnnp.59.3.225. [DOI] [PMC free article] [PubMed] [Google Scholar]