

Abstract
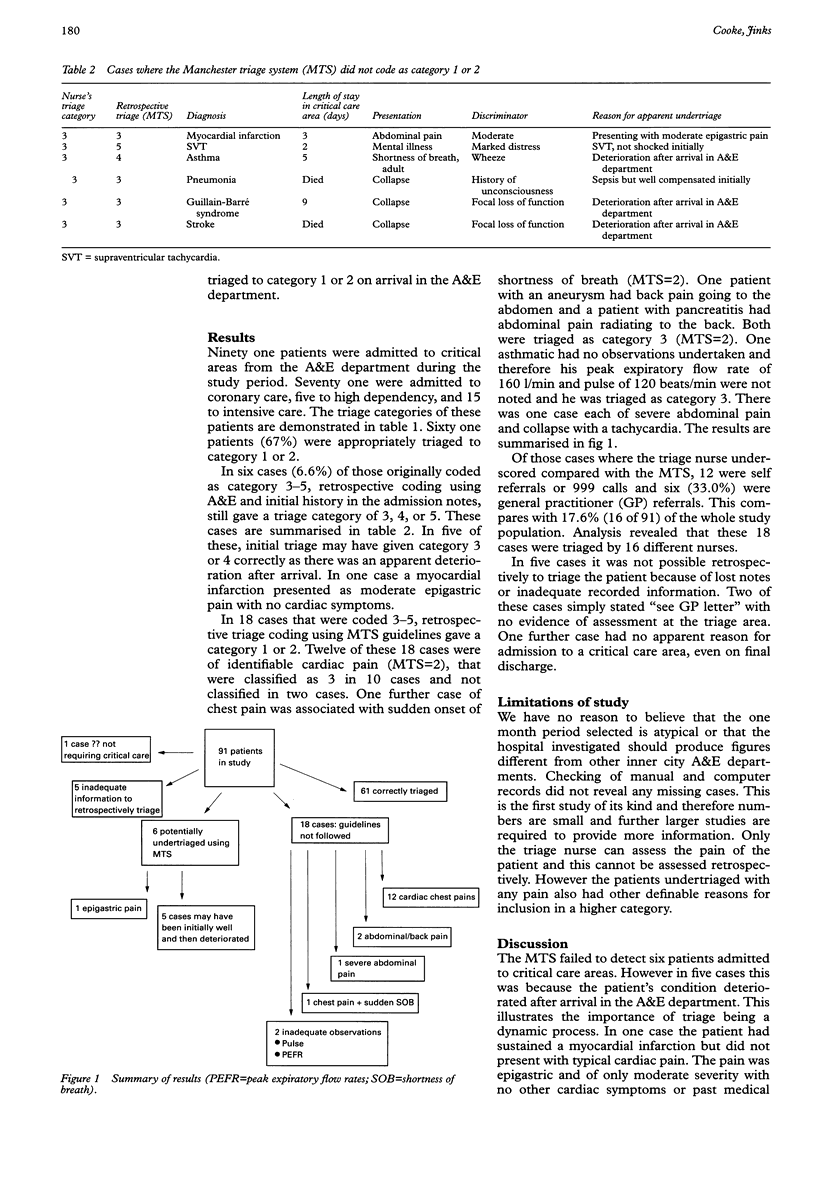
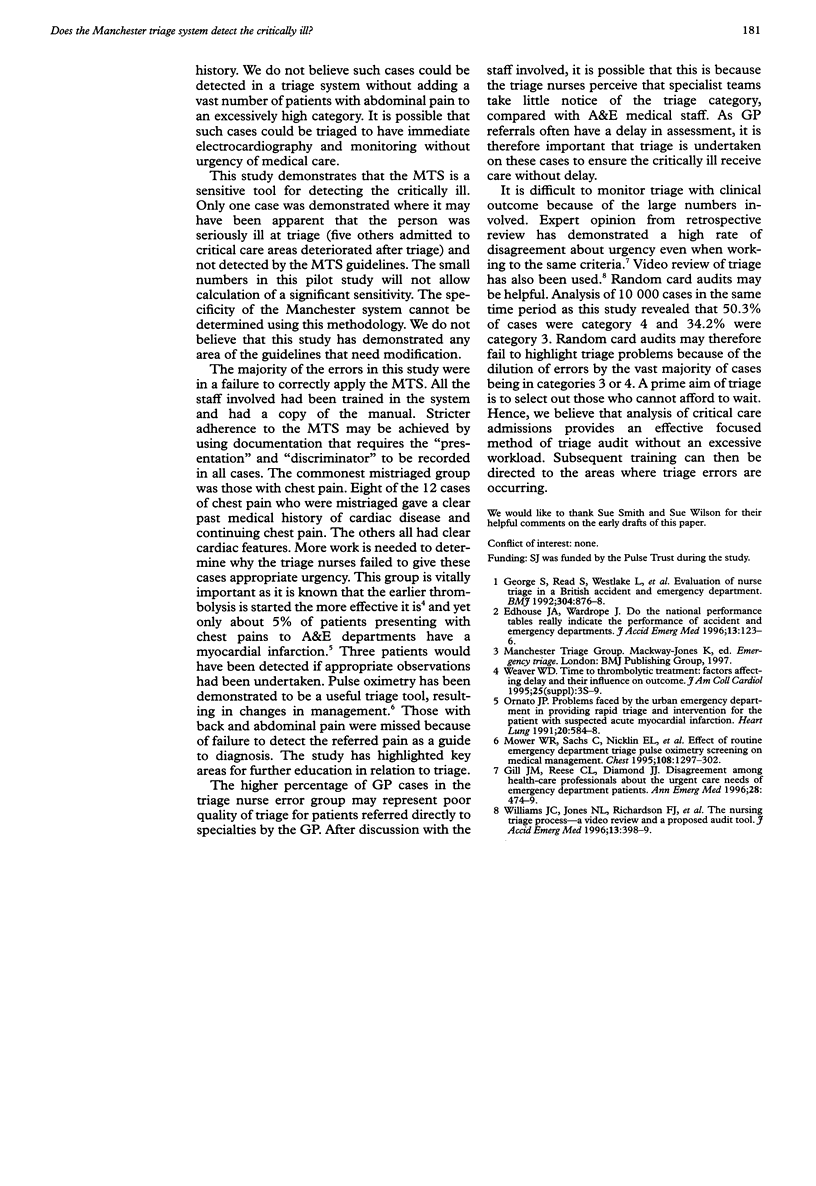
BACKGROUND: The Manchester triage system (MTS) is now widely used in UK accident and emergency (A&E) departments. No clinical outcome studies have yet been published to validate the system. Safety of triage systems is related to the ability to detect the critically ill, which has to be balanced with resource implications of overtriage. OBJECTIVES: To determine whether the MTS can reliably detect those subsequently needing admission to critical care areas. METHODS: Analysis of emergency admissions to critical care areas and comparison with original A&E triage code by a nurse using the MTS at time of presentation. Retrospective coding of all cases according to the MTS by experts and case analysis to determine whether any non-urgent coding was due to the system or to incorrect coding. RESULTS: Sixty one (67%) of the patients admitted to a critical care area were given triage category 1 or 2 (that is, to be seen within 10 minutes of arrival). Eighteen cases given lower priority were due to incorrect coding by the triage nurse. Six cases were correctly coded by the MTS, of which five deteriorated after arrival in the A&E department. Only one case was critically ill on arrival and yet was coded as able to wait for up to one hour. CONCLUSIONS: The MTS is a sensitive tool for detecting those who subsequently need critical care and are ill on arrival in the A&E department. It did fail to detect some whom deteriorated after arrival in A&E. Most errors were due to training problems rather than the system of triage. Analysis of critically ill patients allows easy audit of sensitivity of the MTS but cannot be used to calculate specificity.
Full text
PDF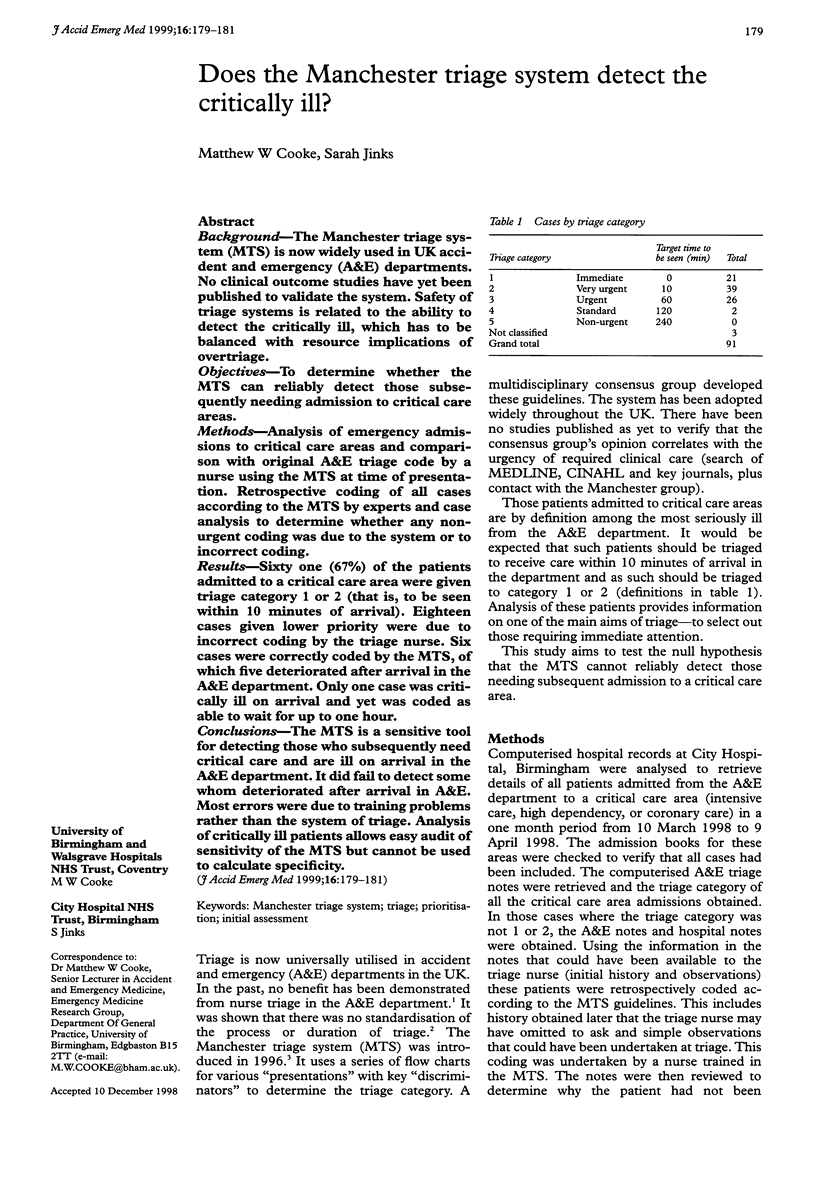
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Edhouse J. A., Wardrope J. Do the national performance tables really indicate the performance of accident and emergency departments? J Accid Emerg Med. 1996 Mar;13(2):123–126. doi: 10.1136/emj.13.2.123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- George S., Read S., Westlake L., Williams B., Fraser-Moodie A., Pritty P. Evaluation of nurse triage in a British accident and emergency department. BMJ. 1992 Apr 4;304(6831):876–878. doi: 10.1136/bmj.304.6831.876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gill J. M., Reese C. L., 4th, Diamond J. J. Disagreement among health care professionals about the urgent care needs of emergency department patients. Ann Emerg Med. 1996 Nov;28(5):474–479. doi: 10.1016/s0196-0644(96)70108-7. [DOI] [PubMed] [Google Scholar]
- Mower W. R., Sachs C., Nicklin E. L., Safa P., Baraff L. J. Effect of routine emergency department triage pulse oximetry screening on medical management. Chest. 1995 Nov;108(5):1297–1302. doi: 10.1378/chest.108.5.1297. [DOI] [PubMed] [Google Scholar]
- Ornato J. P. Problems faced by the urban emergency department in providing rapid triage and intervention for the patient with suspected acute myocardial infarction. Heart Lung. 1991 Sep;20(5 Pt 2):584–588. [PubMed] [Google Scholar]
- Weaver W. D. Time to thrombolytic treatment: factors affecting delay and their influence on outcome. J Am Coll Cardiol. 1995 Jun;25(7 Suppl):3S–9S. doi: 10.1016/0735-1097(95)00108-g. [DOI] [PubMed] [Google Scholar]
- Williams J. C., Jones N. L., Richardson F. J., Jones C., Richmond P. W. The nursing triage process: a video review and a proposed audit tool. J Accid Emerg Med. 1996 Nov;13(6):398–399. doi: 10.1136/emj.13.6.398. [DOI] [PMC free article] [PubMed] [Google Scholar]