

Abstract
The present study assesses the interrelation among domains of ethnic factors, the individual’s sense of well-being, personality/attitudes/behaviors, sibling and peer smoking, and adolescent smoking behavior. The sample consisted of 1,468 South African adolescents selected from four ethnic groups self-identified as defined by current South African usage: Black (mainly Zulu and Xhosa), Indian, White, and Coloured (mixed ancestry). In accordance with Family Interactional Theory, there was a sequence of patterning from ethnic factors and the individual’s sense of well-being to adolescent personality/attitudes/behaviors and models of smoking. All of the four domains in the model also had a direct effect on adolescent smoking behavior. The findings suggest four possible targets of therapeutic or preventive intervention with regard to adolescent smoking: ethnic factors, the individual’s sense of well-being, personality/attitudes/behaviors, and smoking within the peer group.
Keywords: Adolescent smoking, Ethnicity, South Africa, Sense of well-being, Personality
According to the World Health Report 2002 (World Health Organization, 2002), tobacco use was responsible for 4.1% of disability adjusted life years (DALYs) lost in 2000. Most (61%) of the DALYs occurred in the 15–59 year old age group, with a further 39% occurring for those aged 60 years and older (World Health Organization, 2002). In that same year, 4.9 million premature deaths were attributable to smoking (World Health Organization, 2002).
During the past decade, South Africa has made substantial advances in the policy arena and currently has one of the most comprehensive tobacco control policies in the world (Malan & Leaver, 2003). A number of studies have shown that there have been significant reductions there in rates of lifetime smoking among adults (e.g., 33% to 27% between 1993 and 2000; van Walbeek, 2002). For South African adolescent high school students, according to the results of the Global Youth Tobacco Survey conducted in 1999 and repeated in 2002, there was a decrease from 46.7% (95% CI = 41.8% to 51.6%) to 37.6% (95% CI = 34.4% to 40.8%) in lifetime smoking rates, and decreases were also observed between the two years in the proportions of frequent smokers in the samples (Reddy & Swart, 2003). In order for these gains to be sustained, however, they need to be part of a comprehensive tobacco control strategy, which also involves implementation of empirically-derived demand reduction interventions. However, thus far, there has been a paucity of risk factor studies from which comprehensive, multi-level intervention approaches for adolescents can be developed.
This paper examines a model of smoking behavior (depicted in Figure 1) derived from Family Interactional Theory (Brook, Brook, Gordon, Whiteman, & Cohen, 1990), in which the roles of various psychosocial risk factors found to predict adolescent smoking behavior in the United States of America (U.S.A.) are examined among adolescents in South Africa. The key domains of risk factors include ethnic factors, the individual’s sense of well-being, peer, sibling and significant other smoking, and personality/attitudes/behaviors. The proposed model posits that two domains of constructs: (1) personality/attitudes/behaviors, and (2) peer, sibling, and significant other smoking are each direct predictors of smoking behavior, as well as being mediators of less immediate predictors of smoking behaviors, namely, the individual’s sense of well-being, and ethnic factors. The association between these various psychosocial factors and adolescent smoking behavior is described for each domain in turn.
Figure 1.
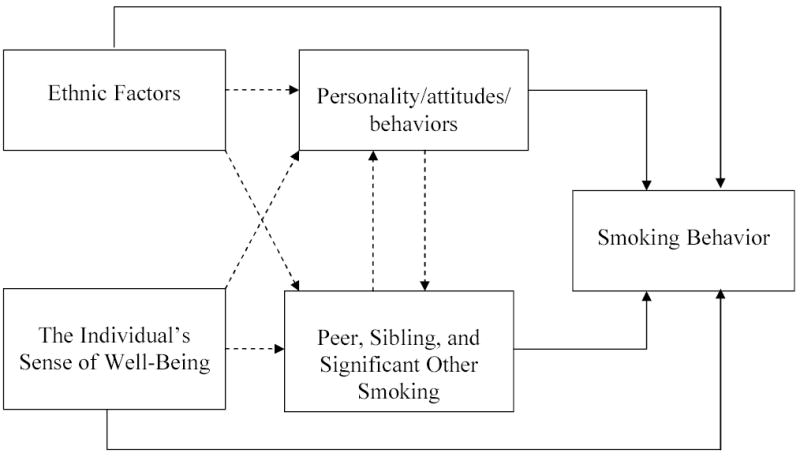
The interrelation of ethnic factors, sense of well-being, personality/attitudes/behaviors, and peer, sibling, and significant other smoking behavior with adolescent smoking.
Ethnic Factors
The past decade has seen a growing awareness among academic scholars and policy makers of the importance of ethnic identification in the development of children and adolescents. Research conducted primarily in the United States (Brook, Balka, Brook, Win, Gursen, & Rosenberg, 1998) has shown that adolescents with a secure sense of belonging to a specific ethnic group tend to have more positive health outcomes, including being less likely to be involved in tobacco use than do those with an insecure sense of ethnic identification. Brook and colleagues have recently argued that the importance of ethnic identification is not limited to the United States (Brook, Brook, & Pahl, in press). Nevertheless, at the present time, there is a dearth of empirically-based literature focusing on the relationship between ethnic identification and smoking behavior, both in the U.S. and in other countries. Due to the possible importance of such cultural factors in smoking, the current study attempts to document the relationship between adolescents’ ethnic identification and their smoking behavior in a cohort of South African adolescents, and specifically, the manner in which ethnic identification predicts smoking behavior both directly and indirectly.
Being a member of a specific ethnic group encompasses many different experiences, some of which may be considered protective factors (e.g., ethnic identity achievement), while others (e.g., the experience of discrimination) may serve as risk factors for the use of tobacco, as has been found in previous studies (e.g., Guthrie, Young, Williams, Boyd, & Kintner, 2002). In a recent study conducted in the U.S., Brook and colleagues demonstrated that ethnic identification served as a protective factor to offset risk conditions (such as sibling tobacco use and low maternal identification) associated with smoking behavior (Brook, Pahl, Balka, & Fei, in press). They investigated an important aspect of ethnic identification which concerns the individual’s attachment and feeling of belonging to his or her own ethnic group (Cheung, 1993; Phinney, Chavira, & Williamson, 1992). There is also some evidence that such aspects of ethnic identification (as measured by a sense of affirmation, belonging, and knowledge of one’s ethnic background) are associated with adaptive psychological adjustment (Phinney & Kohatsu, 1999).
A second aspect of ethnic group membership, which is associated with negative health outcomes among adolescents, is discrimination (Kwate, Valdimarsdottir, Guevarra, & Bovbjerg, 2003; Williams, 1999). Individuals who experience greater levels of discrimination become more prone to use of cigarettes and other drugs as a way of coping with the experience of bias and discrimination against them (Guthrie et al., 2002).
Therefore, we hypothesize that for adolescents in South Africa, ethnic factors will also be an important predictor of their smoking behavior, since in the U.S. there exists both a direct and an indirect association with such behavior. For the latter case, we hypothesize that the association of ethnic factors with smoking will be mediated by the following domains: (a) adolescent personality, attitudes, and behaviors; and (b) peer, sibling, and significant other smoking behavior.
Sense of Well-Being
We hypothesize that a second domain, the individual’s sense of well-being, will also have an indirect association with adolescent smoking behavior. Adolescents who do not have a strong sense of well-being are particularly likely to experience stress (Shek, 2003). Self-perceived quality of life, defined broadly as an amalgam of both internal (e.g., self-esteem) and external factors (e.g., neighborhood influences), has also been found to be associated with adolescent health risk behavior (e.g., Topolski et al., 2001), as those adolescents who feel that their lives have lesser value (relative to societal expectations) are more willing to take risks with their health. The domain of the individual’s sense of well-being is expected to have indirect effects on smoking behavior, mediated through the domains of adolescent personality/attitudes/behaviors and peer, sibling, and significant other smoking. Adolescents who are dissatisfied with themselves and their environment will likely act to sow discontent and dissatisfaction in their siblings, potentially leading them toward increased smoking behavior. In addition, adolescents who lack a sense of well-being are more likely to select peers and significant others who are also disgruntled, and thus are more likely to be smokers (potentially mediated by their own personality traits). Conversely, we hypothesize strong sense of well-being will be associated with choosing more conventional and positive peers and significant others who will likely refrain from smoking. Thus, the individual’s sense of well-being is expected to be inversely related to deviance-prone personality/attitudes/behaviors (such as rebelliousness), and positively associated with conventional attributes (such as being accepting of conventional roles). To the best of our knowledge, researchers have not investigated the relationship between the individual’s sense of well-being and smoking behavior among adolescents in South Africa.
Smoking Behavior by Peers, Siblings, and Significant Others
Having peers and/or significant others (e.g., romantic partners) who smoke predicts adolescent smoking behavior (Panday, Reddy, & Bergstrom, 2003; Jackson, 1997). We combined smoking by peers, siblings, and significant others into one domain, since use by all three groups represents models of drug use for adolescents. While smoking by peers and significant others is expected to have a direct association with adolescent smoking through modeling, the relationship between smoking by peers and significant others also is expected to have an indirect pathway to smoking, mediated by the adolescent’s personality vulnerabilities (Unger & Chen, 1999). Thus, having siblings and peers (including significant others) who smoke will be associated with having unconventional personality attributes, which will, in turn, be associated with smoking behavior. Numerous studies conducted among adolescents in South Africa confirm that adolescents whose siblings and peers smoke are more likely to be smokers than are those with predominantly non-smoking peers and family members (King et al., 2003; Peltzer, in press).
Personality/Attitudes/Behaviors
We hypothesize that the domain of tobacco-prone personality/attitudes/behaviors will be directly associated with smoking and will also serve to mediate the relationship between the domains of ethnic factors, the individual’s sense of well-being, peer, sibling, and significant other smoking, and adolescent smoking behavior. Adolescents who are unconventional (e.g., rebellious, tolerant of deviant behavior, or who engage in deviant behavior), are more likely to smoke (Andrews & Duncan, 1997), as are those who have difficulty controlling their impulses (Mitchell, 1999), and those who experience symptoms of depression (Breslau, 1995; McCaffery, Niaura, Swan, & Carmelli, 2002). While tobacco-prone personality/attitudes/behaviors are expected to have a direct association with smoking behavior, they are also expected to have indirect effects through the peer, sibling, and significant other smoking domains. Rose, Chassin, Presson, Clark, and Sherman (1999) demonstrated that adolescents with tobacco-prone personality attributes were more likely to select peers who smoke, which is in turn related to the adolescents’ own smoking behavior.
Pathways to Adolescent Tobacco Use
We are not aware of any studies conducted in South Africa that systematically trace the experience of discrimination and low ethnic identification to the development of health-compromising behaviors, such as tobacco use. On the basis of the empirical and theoretical work available on this topic, we hypothesize a mediational model according to which ethnic factors (specifically, low levels of ethnic identification and high levels of discrimination) and the individual’s reduced sense of well-being are related to tobacco-prone personality, attitudes, and behaviors, and peer, sibling, and significant other smoking behavior, both of which are in turn related to tobacco use. Such a model suggests that the proximal factors (personality, attitudes, and behaviors, and peer, sibling, and significant other smoking) have stronger correlations with smoking behavior than the more distal domains of ethnic factors and sense of well-being. The primary aim of the study is to examine whether the proposed mediational model (depicted in Figure 1) reflects the relationships among the four psychological domains involving: (1) ethnic factors, (2) the individual’s sense of well-being, (3) personality/attitudes/behaviors, and (4) peer, sibling, and significant other smoking in accounting for smoking behavior among an ethnically heterogeneous sample of adolescents in South Africa.
Method
Participants
This study examines a sample of 1468 adolescents, drawn from two cities in South Africa, Durban and Cape Town in 2001–2002. The sample is 45% male and 55% female. The subjects are divided into four ethnic groups: 660 (45%) are African/Black (mainly Zulu and Xhosa); 204 (14%) are Indian; 289 (20%) are White; 311 (21%) are Coloured (a South African term for people of mixed ancestry). The adolescents range in age from 12 to 17 years, with a mean of 14.7 years (SD=1.9). The first languages spoken include the following: 22% spoke Zulu, 21% Xhosa, 24% Afrikaans, and 31% spoke English (the remaining 2% reported other languages as first languages). Religious backgrounds varied as well, with 8% being Hindu, 5% Muslim, and the remainder of the sample belonging to various forms of Christianity. In terms of the home environment, 62% of the subjects lived with the biological father, and 84% with the biological mother. Fourteen percent of the subjects lived with a male guardian instead of the biological father, 12% with a female guardian instead of the biological mother, and 3.5% lived with no biological parent or legal guardian. The overlap noted is due to the fact that some parents/surrogates may appear in two categories.
Procedure
A stratified, random sampling approach was employed for obtaining the sample. We used a multi-stage sampling procedure in which the sample was stratified by race and socioeconomic status, based on the 1996 population census (the census data allowed us to select appropriate census enumerator areas). Socioeconomic status for the enumerator areas was determined through employment rates listed for the head of household. Note that the 1996 census only determined if the head of household was employed, not the type of position and associated compensation (if any) that the individual received. The adolescent respondents were recruited from households within the selected census enumerator areas. A starting point was designated randomly for each area, and every tenth household was visited to determine if an eligible adolescent resided there. Eligible adolescents were defined as those between the ages of 12 and 17 years, inclusive. When more than one adolescent in a household qualified for the study, we used a random selection procedure to determine which one to include. Over 85% of the adolescents approached agreed to take part in the study.
The instrument was translated from English into three languages, Afrikaans, Xhosa, and Zulu. In order to guarantee that the questionnaires retained their meaning after translation, all instruments were translated back into English and checked against the original English version. All discrepancies were corrected.
Individual, in-person interviews were conducted by trained interviewers after obtaining informed consent. Informed written consent was obtained from a parent or guardian, prior to getting assent in writing from the adolescent. After obtaining consent, a private location was found to administer the questionnaire. This was either a room in the subject’s residence, or an outdoor location far enough away from anyone else to ensure privacy. Whenever possible, interviewers and subjects were matched on gender and ethnicity, and subjects were administered the questionnaire in their language of choice. Subjects who did agree to participate overwhelmingly completed all of the questions within the instrument (i.e., the rate of missing data was approximately 1%).
The interviewer read the questionnaire aloud to the subject and recorded her/his responses. For questions of a sensitive nature (e.g., smoking behavior), participants were given the instrument and requested to record the answers themselves. The questionnaire took approximately one hour to complete. At the end of the interviews the subjects were offered a resource list of treatment centers but did not receive any monetary incentive for their participation. A Certificate of Confidentiality was obtained from the National Institute on Drug Abuse to ensure confidentiality. All procedures and consent forms were approved both by the Ethics Committee of the Medical Research Council of South Africa, and by the New York University School of Medicine’s Institutional Review Board.
Measures
The questionnaire administered to the participants included measures assessing the adolescents’ personality, attitudinal, and behavioral attributes, their siblings, a significant other, and peer groups’ smoking behaviors, the individual’s sense of well-being, ethnic identification, and demographic factors. The instrument was adapted mainly from measures that have proven to be predictive of risk behaviors in previous studies conducted in the U.S., South Africa, and South America. In addition, similar measures have shown both concurrent validity and predictive validity in studies conducted in South America (Brook, Brook, De La Rosa, Whiteman, Johnson, & Montoya, 2001; Brook, Brook, Pahl, & Montoya, 2002; Brook, Brook, Rosen, & Montoya, 2002), and in several samples collected in the U.S. (Brook, Pahl, et al., in press; Brook, Brook, Rubenstone, Zhang, Singer, & Duke, 2003; Brook, Brook, & Whiteman, 2000; Fagan, Brook, Rubenstone, & Zhang, in press). Measures collected in these settings have shown consistent relationships with both smoking and other health-risk behaviors. Instrument development was based on focus groups which were conducted in South Africa in order to ensure that the adapted measures were appropriate for use in South Africa, and on a pre-test of a pilot questionnaire among samples of adolescents. Items assessing cultural practices were developed to be both comprehensive and inclusive.
The dependent variable used in the analysis was a dichotomized measure of self-reported current smoking. The two groups included current smoking, ranging from a few cigarettes a week to smoking more than a pack a day (14.9%) and no smoking (85.1%). This measure was derived from a question regarding current smoking frequency. Smoking frequency was assessed with the following item: “How many cigarettes do you smoke?” Responses to the presented categories ranged from 1 (“none”) to 6 (“more than a pack a day”). This measure has been validated in other studies, both in the U.S. as well as in South Africa (Brook, Whiteman, Czeisler, Shapiro, & Cohen, 1997; Reddy & Swart, 2003).
Measures from four domains were used as independent variables for this study: (1) personality/attitudes/behaviors, (2) ethnic factors, (3) the individual’s sense of well-being, and (4) peer, sibling, and significant other smoking. Table 1 presents the scale names, number of items, sample questions, and Cronbach’s alphas for all the measures.
Table 1.
Predictors of Smoking: Domains, Sample Items, and Cronbach’s Alphas
| Measure (no. of items) | Sample Item | Source | Chronbach’s Alpha |
|---|---|---|---|
| Personality/attitudes/behaviors Domain | |||
| Rebelliousness (5) | When rules get in your way you sometimes ignore them. | Smith & Fogg (1979) | 0.62 |
| Impulsivity (5) | I often act on the spur of the moment without thinking. | Jackson (1974) | 0.43 |
| Depressive symptoms (5) | How much are you bothered by feeling no interest in things? | Derogatis (1974) | 0.76 |
| Self-Deviance (5) | How often have you cheated at school or work? | Jessor & Jessor (1977) | 0.72 |
| Tolerance of deviance (6) | How wrong is it to fake an excuse from home? | Jackson (1974) | 0.83 |
| Peer, sibling, and significant other Smoking Domain | |||
| Sibling smoking (1) | How many of your biological brothers and sisters, including half brothers and sisters, have ever smoked regularly? | Brook et al. (1990) | --- |
| Peer smoking (1) | How many of your friends smoke on a regular basis? | Brook et al. (1990) | --- |
| Significant other smoking (1) | Has your boyfriend/girlfriend ever used cigarettes? | Original | --- |
| Ethnic Factors Domain | |||
| Experienced discrimination (4) | How much have you experienced discrimination by the police or security guards? | Original | 0.74 |
| Ethnic identification achievement (4) | How much time have you spent trying to learn about your ethnic group? | Phinney (1992) | 0.82 |
| Affirmation and belonging (4) | You have a strong sense of belonging to your own ethnic group. | Phinney (1992) | 0.86 |
| The Domain of the Individual’s Sense of Well-Being | |||
| Satisfaction with one’s self (3) | How satisfied are you with how clever you are? | Original | 0.79 |
| Satisfaction with material things (6) | How satisfied are you with how you spend your free time? | Original | 0.85 |
| Satisfaction with social Support (3) | How satisfied are you with the friends you have? | Original | 0.78 |
| Satisfaction with school (6) | Do you find your studies stimulating? | Original | 0.83 |
Statistical Analysis
First we examined the relationship of the dichotomized smoking measure and five demographic factors, namely, gender, ethnicity, age, living situation, and socioeconomic status (SES). Second, odds ratios were computed examining the magnitude of the influence of each of the variables in the domains of personality/attitudes/behaviors, peer, sibling, and significant other smoking, ethnic factors, and the individual’s sense of well-being as they relate to current smoking. Third, we employed hierarchical logistic regression analysis to test a model of the interrelationship of domains (Cohen, Cohen, West, & Aiken, 2003). When using this model, domains of predictors are first examined in multiple logistic regression analyses where each measure of a domain is placed simultaneously into a single regression equation, and a measure of fit (Nagelkerke’s pseudo R2) is determined. Second, the domains are tested controlling for potential mediating domains. If a mediational model were operative, at least two conditions would need to be met. First, without control, each of the domains should have a significant relationship to adolescent smoking behavior. Second, the more distal domains (ethnic identification and the individual’s sense of well-being) should be related to smoking through the more proximal domains. In such cases, the goodness of fit of the distal and proximal domains combined in a multiple regression model is not significantly greater than that of the proximal domain alone, as determined by an F-test. This follows the outline for testing mediational models as suggested by Baron and Kenny (1986).
Results
We first examined whether each of five demographic factors were associated with current smoking behavior. Three of the five demographic variables had a significant association. Gender was significant ( χ2=22.4, d.f.=1, p<.001), with males being significantly more likely to smoke cigarettes than females. Ethnicity also had a significant effect (χ2=38.7, d.f.=3, p<.001). Smoking rates by ethnic group were; 24.8% of the “Coloured” sample were current smokers, 10.7% of the black sample, 17.6% of the white sample, and 9.8% of the Indian sample. Age was also significantly associated with current smoking (t=11.05, d.f.=353.4, p<0.001) in that older adolescents smoked more frequently than younger adolescents. Living situation (living with both parents vs. with one or no parents) and SES (measured by the number of amenities present in the household) did not have a significant association with current smoking.
We then examined the interaction of the independent variables with the demographic factors (i.e., gender, ethnicity, and number of parents in the household). Less than 5% of the interactions were significant, and no discernible pattern emerged. Specifically, our examination for interaction terms revealed that gender and ethnicity did not interact. Due to the lack of significant interactions between the demographic variables and the independent variables, subsequent analyses were done with the combined sample.
Next, odds ratios were computed to examine the influence of each of the variables in the domains of personality/attitudes/behaviors, peer, sibling, and significant other smoking, ethnic factors, and the individual’s sense of well-being, as they relate to current smoking. Note that these analyses control for age, gender, ethnicity and SES, which was determined by proxy through a measure of amenities present in the home (e.g., a telephone, T.V., etc.). The findings (displayed in Table 2) indicate that smoking was significantly associated with all of the personality/attitude/behavior measures (e.g., rebelliousness, impulsivity, depressive symptoms, delinquent behavior, and tolerant attitudes toward delinquent behavior). Furthermore, adolescents who smoke tend to have peers, siblings, and significant others who also smoke. The results also suggest that adolescents who have a strong sense of well-being are less likely to smoke. Finally, adolescents who smoke are more likely to report experiencing discrimination and having a weaker identification with their own ethnic groups.
Table 2.
Odds Ratios of Psychosocial Measures for Current Smoking Behavior
| Measures | Odds Ratio | 95% C.I. |
|---|---|---|
| The Domain of Personality/Attitudes/Behavioral Attributes | ||
| Rebelliousness | 1.17*** | (1.12–1.23) |
| Impulsivity | 1.21*** | (1.15–1.28) |
| Depressive symptoms | 1.08*** | (1.04–1.12) |
| Self-deviance | 1.20*** | (1.16–1.25) |
| Tolerance of deviance | 1.20*** | (1.16–1.25) |
| The Domain of Peer, Sibling, and Significant Other Smoking Behavior | ||
| Sibling smoking | 1.40*** | (1.19–1.64) |
| Peer smoking | 2.31*** | (1.97–2.70) |
| Significant other smoking | 5.40*** | (3.77–7.74) |
| The Domain of Ethnic Factors | ||
| Experienced discrimination | 1.23*** | (1.15–1.31) |
| Ethnic identification achievement | 0.95* | (0.90–0.99) |
| Affirmation and belonging | 0.88*** | (0.85–0.91) |
| The Domain of the Individual’s Sense of Well-Being | ||
| Satisfaction with oneself | 0.82*** | (0.75–0.88) |
| Satisfaction with material things | 0.88*** | (0.84–0.91) |
| Measures | Current Smoking | |
| Satisfaction with social support | 0.83*** (0.76–0.90) | |
| Satisfaction with school | 0.90*** (0.85–0.91) | |
p<0.05;
p<0.001
To assess whether our data was consistent with our hypothesized mediational model, we performed hierarchical logistic regression analyses. We decided to employ Nagelkerke’s pseudo R2 as the metric for our models because its range {0, 1} is closest to the more familiar R2 metric determined by OLS. In order to ensure that there was not a bias associated with this particular pseudo R2 calculation, we rechecked our findings using the standard McFadden’s pseudo R2. In all cases the same pattern of results were obtained. In order to control for the main effects of the demographic variables, these analyses controlled for age, gender, ethnicity, and SES. We first examined the relationship between each domain (ethnic factors, personality/attitudes/behaviors, the individual’s sense of well-being, and peer, sibling, and significant other smoking behavior) and adolescent smoking behavior independently. All of the domains were significantly related to the adolescents’ smoking behavior (p<.001).
We then examined the relationship of each domain with smoking behavior, controlling for the other domains in the model (see Table 3). The domains of personality/attitudes/behaviors, and peer, sibling, and significant other smoking were most highly related to adolescent smoking. It should be noted that each of the domains had a direct effect on smoking behavior, even when controlling for a second domain. The domain of personality/attitudes/behaviors maintained a significant relationship with smoking when controlling for the domain of peer, sibling, and significant other smoking behavior; an 83% drop in pseudo R2 was observed. The percent drop in pseudo R2 was calculated by first subtracting the pseudo R2 for the peer, sibling, and significant other smoking behavior domain (0.3605) from the combined total pseudo R2 for the personality/attitudes/behaviors domain and the peer, sibling, and significant other smoking behavior domain combined (0.4341). This difference (0.0736) was then divided by the pseudo R2 for the combined domain (0.736/0.4341 = 0.1695), which, when converted to a percentage, provides the percent of the total explanatory power the partialled domain represents. Finally, this number was subtracted from 100%, which gives us a measure of the decrease in explanatory power of the personality/attitudes/behaviors domain when the explanatory power (pseudo R2) for the peer, sibling, and significant other smoking behavior domain is partialled out (100%–16.95% = 83.05%), which we then rounded to 83%. This implies that the effect of the domain of personality/attitudes/behaviors on adolescent smoking is partially mediated by the domain of peer, sibling, and significant other smoking behavior. At the same time, with control on the domain of personality/attitudes/behaviors, the pseudo R2 for the peer, sibling, and significant other smoking domain dropped by 91%. This implies a bi-directional relationship between the domains of personality/attitudes/behaviors and peer, sibling, and significant other smoking behavior.
Table 3.
Nagelkerke’s Pseudo R2 for the Domains and Current Smoking Behavior Among Adolescents
| With Control on the Following Domains
|
|||||
|---|---|---|---|---|---|
| Psychosocial Domain | Without Control | Personality Attributes | Peer, Sibling, Sig. Other Smoking | Ethnic Factors | The Individual’s Sense of Well-Being |
| Personality Attributes | 0.35* | --- | 0.07* | 0.13* | 0.10* |
| Peer, Sibling, Sig. Other Smoking | 0.36* | 0.04* | --- | 0.15* | 0.13* |
| Ethnic Factors | 0.23* | 0.01* | 0.03* | --- | 0.02* |
| The Individual’s Sense of Well-Being | 0.26* | 0.02* | 0.04* | 0.05* | --- |
All analyses control for age, gender, ethnicity, and SES.
p<0.001
The domain of the individual’s sense of well-being was also examined. As indicated in Table 3, this domain continued to be significantly related to adolescent tobacco use with control on the domains of peer, sibling, and significant other smoking behavior and ethnic factors. However, with control on the domain of personality/attitudes/behaviors, the pseudo R2 for the relation between the domain of the individual’s sense of well-being and the domain of smoking behavior dropped 96%, strongly implying partial mediation. Further, when the domain of peer, sibling, and significant other smoking was controlled for, a 91% reduction in pseudo R2 between the domain of the individual’s sense of well-being and smoking behavior was observed, implying partial mediation in this case.
We next examined the association between the domain of ethnic identification and current cigarette use while controlling for the domains of personality/attitudes/behaviors and peer, sibling, and significant other smoking behavior. The relation of the domain of ethnic identification and smoking behavior maintained statistical significance despite control on the domains of personality/attitudes/behaviors and peer, sibling, and significant other smoking behavior; nevertheless, there was a 96% reduction in the pseudo R2 in the first case, and a 93% reduction in the second, signifying partial mediation through both of these domains.
Discussion
The present study extends previous research in several important ways. First, the research was designed to study South African adolescents. Second, this investigation focuses on the influence of ethnic factors on smoking behavior and the mechanisms through which ethnic factors operate. Third, we assess several interrelated but distinctive domains: ethnic factors, adolescent personality/attitudes/behaviors, the individual’s sense of well-being, and peer, sibling, and significant other smoking.
In general, the risk factors related to tobacco use in South Africa are similar to the predictors of smoking in the U.S. (see Bachman, Wadsworth, O’Malley, Johnston, & Schulenberg, 1997; Jessor 1991). However, other factors (e.g., cultural) not assessed in this study may affect the relationship between the risk factors and smoking behavior. Empirical studies focusing on discrete cultural factors, using multi-method techniques, should help to identify both the universal and the specific factors implicated in cigarette use.
Although the sample used in this study contains a wide range of individuals (four ethnic groups drawn from two South African cities across a wide age range, 12–17), consistent relationships were found relating the examined factors to smoking behavior. Such results point to the fact that although the rates of health-compromising behaviors may vary across ethnicities, age groups, or regions, similar pathways leading to such behaviors exist for urban South African adolescents in general.
Also of interest is how these findings fit with current theories of health-risk behavior. Models such as the theory of planned behavior (Ajzen, 1991), and the attitudes-social influences-efficacy model (De Vries & Backbier, 1994; De Vries, Backbier, Kok, & Dijkstra, 1995; De Vries, Dijkstra, & Kuhlman, 1988), consider the effect of attitudes and social influences, as well as other factors such as self-efficacy and perceived behavioral control. This model found support for a relationship between at least one attitude factor, tolerance of deviance, and health-risk behavior, and considered the social influence of the peer group (as well as siblings and significant others) as models of acceptable behavior. Although these findings do not support one model over the other, they do shed light on how these and other psychosocial factors interact to affect one’s health-risk behavior.
Ethnic Identification
The findings of this study support a theoretically-derived model based on Family Interactional Theory (Brook et al., 1990). More specifically, the results indicate that the domain of ethnic identification and discrimination is directly related to adolescent tobacco use. Furthermore, the relationship between the domain of ethnic identification and discrimination and smoking is associated with tobacco-prone personality/attitudes/behaviors and peer, sibling, and significant other smoking, which, in turn, are associated with adolescent tobacco use (Figure 1). Thus, the domain of ethnic identification and discrimination is of great importance in that it has a powerful impact on adolescent personality/attitudes/behaviors, particularly in regard to tobacco use behavior. Similarly, ethnic factors are closely linked with sibling, peer and significant other smoking behavior. It may be that a strong ethnic identification and low levels of discrimination enable the adolescent to resist the impact of smoking behavior by siblings and peers. On the other hand, discrimination, a lack of attachment, and a lack of a sense of belonging to one’s own ethnic group may lead to the erosion of informal ties, which may create social alienation, stress, and a decrease in communication. This may then compromise informal social control of the adolescent’s behavior (Sampson, Raudenbush, & Earls, 1997). It is possible that adolescents who do not have a strong sense of belonging to their own ethnic groups do not receive as much monitoring from the family, and consequently become more prone to turn to those peers and significant others who reward unconventional norms and behavior, including smoking behavior. It should be noted that literature exists showing that unacculturated members of specific ethnic groups, especially those living in areas dominated by other cultures (e.g., immigrant groups), may have smoking rates far above the norm for that region (Markham, Aveyard, Thomas, Charlton, Lopez, & De Vries, 2004; Markham, Featherstone, Taket, Trenchard-Mabere, & Ross, 2001). Although smoking rates may differ by ethnicity, ethnic identification, as a measure of knowledge and pride in one’s ethnic group, is shown to be related to reduced smoking rates, both directly, and as mediated both through adolescent personality, as well as through peer and significant other selection.
Personality
As hypothesized, the domain of personality/attitudes/behaviors had a direct effect on adolescent smoking, as well as being mediated by the domain of smoking behavior by siblings and peers. As in the United States, there was a reciprocal relationship between the domain of personality/attitudes/behaviors and the domain of smoking behavior by siblings and peers (Ennett & Bauman, 1994). There is a reciprocal relationship between adolescent tobacco-prone personality traits and tobacco use by peers. Adolescents with tobacco-prone personality traits were more likely to associate with tobacco-using and deviant peers. Having friends who smoke was then linked with the adolescent having tobacco-prone personality traits. Consistent with findings reported in the United States, five personality dimensions appeared to be of importance in this regard: namely, difficulty in self-regulation (impulsivity), intrapersonal distress, rebelliousness, delinquent behavior, and tolerance of delinquent behavior (Brook et al., 1997; Jessor, 1991).
Peer, Sibling, and Significant Other Smoking
The domain of peer, sibling, and significant other smoking was also related to adolescent smoking. The present findings may help to identify the mechanisms accounting for transmission of nicotine use in families (Rohde et al., 2003). Modeling of smoking behavior by friends, significant others, and siblings also constitute important categories of social-influence variables. The findings of a dominant role of the domain of peer, sibling, and significant other smoking in the adolescents’ smoking behavior is consistent with the results of studies conducted by researchers in the United States (Biglan, Duncan, Ary, & Slomkowski, 1995; Brook et al., 1997). Since peers are the primary socializing agents of youth, it is not surprising that the peer, sibling, and significant other smoking domain contributed about as much to the variance in tobacco use as the domain of personality/attitudes/behaviors, and more than the domains of ethnic factors and the individual’s sense of well-being. In addition to having a direct effect on adolescent smoking, the domain of peer, sibling, and significant other smoking was mediated by the domain of personality/attitudes/behaviors. Obviously, the strength of the influence of smokers in the adolescent’s immediate environment on the adolescent’s smoking is mediated in part by the adolescent’s personality.
The Individual’s Sense of Well-Being
Another significant pathway is from the individual’s having a sense of well-being to adolescent smoking behavior. Not maintaining a sense of well-being that encompasses satisfaction with the self and aspects of the environment (i.e., social support, the school environment, material possessions) is associated with tobacco-prone personality, attitudes, and behaviors, and with peer, sibling, and significant other smoking behavior, which, in turn, are both related to adolescent smoking behavior.
Limitations
Several aspects of this study limit the generalizability of the results. First, the cross-sectional design of the study provides evidence of the relationship between the predictor variables and the adolescent’s tobacco use, but limits any implication of causality. In addition, the direction of the relationship between the variables cannot be established. Thus, some related factors both might influence adolescent tobacco use and be caused by adolescent tobacco use (Cleveland & Wiebe, 2003a & 2003b; Jessor, 1991). It is entirely conceivable that adolescents who smoke may select friends whom they know also smoke (the selection process). Second, data on adolescent tobacco use is based on self-report. Independent biochemical verification of the adolescents’ smoking behavior would be of help in future research, for example, by repeated cotinine measures. However, previous research has indicated a substantial correlation between self-report and biochemical evidence for smoking (Kentala, Utriainen, Pahkala, & Matilla, in press). Third, since the study was conducted in two cities in South Africa, we cannot generalize to adolescents living in other cities or rural areas in South Africa. Finally, a number of other important domains should be included in future work. Future research should include factors from multiple levels: both proximal factors, such as maternal and paternal smoking and peer pressure, and distal factors, such as the social environment (cultural norms and acceptability of smoking behavior), public policy, market mechanisms, biological vulnerabilities (including genetic factors), and pharmacological influences.
Clinical Implications
Despite the limitations, the study has important implications for smoking prevention and cessation interventions for adolescents. The effects that emerged in this study illustrate the importance of the pathways among the various domains (e.g., personality/attitudes/behaviors, peer, sibling, and significant other smoking, ethnic identification and discrimination, and the individual’s sense of well-being), and suggest which potential points of intervention are more proximal, and which are more distal to smoking behavior. In this way, we can become more sensitive to the interconnections among more proximal and more distal risk factors, which can result in more promising and effective interventions.
These findings add to the literature by demonstrating that some predictors of cigarette use are consistent across countries, even very different countries (see de Vries, Engels, Kremers, Wetzels, & Muddle, 2003; Leff et al., 2003; Mendis, 1990; Santi, Best, Brown, & Cargo, 1990–91). Such predictors include unconventional behavior, difficulty in emotional control, delinquency, and modeling of smoking behavior by siblings, peers, and a significant other. The degree of significance of the four domains (personality/attitudes/behaviors, peer, sibling, and significant other smoking behavior, ethnic identification and discrimination, and the individual’s sense of well-being) suggests the robustness of these risk factors, and also points to the suggestion that prevention and intervention strategies designed to reduce smoking behavior among American youth can be effective (assuming they take into account cultural influences) in South Africa.
Footnotes
This research was supported by Research Scientist Award DA 00244 to Dr. Judith S. Brook from the National Institute on Drug Abuse, National Institutes of Health, and grant TW 05391 to David W. Brook, M.D., from the Fogarty International Center.
Contributor Information
Judith S. Brook, New York University School of Medicine.
Neo K. Morojele, Medical Research Council Pretoria, South Africa
References
- Ajzen I. The theory of planned behavior. Organizational behavior and human decision processes. 1991;50:179–211. [Google Scholar]
- Andrews JA, Duncan SC. Examining the reciprocal relation between academic motivation and substance: Effects of family relationships, self-esteem, and general deviance. Journal of Behavioral Medicine. 1997;20(6):523–549. doi: 10.1023/a:1025514423975. [DOI] [PubMed] [Google Scholar]
- Bachman, J. G., Wadsworth, K. N., O’Malley, P. M., Johnston, L. D., & Schulenberg, J. E. (1997). Smoking, Drinking, and Drug Use in Young Adulthood. Lawrence Erlbaum Associates: Mahwah, NJ.
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51(6):1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Bierut LJ, Dinwiddie SH, Begleiter H. Familial transmission of substance dependence, alcohol, marijuana, cocaine, and habitual smoking: A report from the collaborative study on the genetics of alcoholism. Archives of General Psychiatry. 1998;55(11):982–988. doi: 10.1001/archpsyc.55.11.982. [DOI] [PubMed] [Google Scholar]
- Biglan A, Duncan TE, Ary DV, Smolkowski K. Peer and parental influences on adolescent tobacco use. Journal of Behavioral Medicine. 1995;18(4):315–330. doi: 10.1007/BF01857657. [DOI] [PubMed] [Google Scholar]
- Breslau N. Psychiatric comorbidity of smoking and nicotine dependence. Behavior Genetics. 1995;25(2):95–101. doi: 10.1007/BF02196920. [DOI] [PubMed] [Google Scholar]
- Brook DW, Brook JS, Pahl T, Montoya ID. The longitudinal relationship between drug use and risky sexual behaviors among Colombian adolescents. Archives of Pediatrics and Adolescent Medicine. 2002;156:1101–1107. doi: 10.1001/archpedi.156.11.1101. [DOI] [PubMed] [Google Scholar]
- Brook DW, Brook JS, Rosen Z, Montoya I. Correlates of marijuana use in Colombian adolescents: A focus on the impact of the ecological/cultural domain. Journal of Adolescent Health. 2002;31(3):286–298. doi: 10.1016/s1054-139x(02)00401-9. [DOI] [PubMed] [Google Scholar]
- Brook DW, Brook JS, Rubenstone E, Zhang C, Singer M, Duke MR. Alcohol use in adolescents whose fathers abuse drugs. Journal of Addictive Diseases, . 2003;22(1):11–34. doi: 10.1300/J069v22n01_02. [DOI] [PubMed] [Google Scholar]
- Brook JS, Balka EB, Brook DW, Win PT, Gursen MD, Rosenberg G. Drug use among African-Americans: Ethnic identity as a protective factor. Psychological Reports. 1998;83:1427–1446. doi: 10.2466/pr0.1998.83.3f.1427. [DOI] [PubMed] [Google Scholar]
- Brook JS, Brook DW, De La Rosa M, Whiteman M, Johnson E, Montoya I. Adolescent illegal drug use: The impact of personality, family, and environmental factors. Journal of Behavioral Medicine. 2001;24(2):183–203. doi: 10.1023/a:1010714715534. [DOI] [PubMed] [Google Scholar]
- Brook JS, Brook DW, Gordon AS, Whiteman M, Cohen P. The psychosocial etiology of adolescent drug use: A family interactional approach. Genetic, Social, and General Psychology Monographs. 1990;116(2):111–267. [PubMed] [Google Scholar]
- Brook, J. S., Brook, D. W. & Pahl, T. (in press). The developmental context for adolescent substance abuse intervention. In H.A. Liddle (ed.). Adolescent substance abuse: Intervention and Management. Treating Adolescent Substance Abuse: State of the Art Science Cambridge University Press.
- Brook JS, Brook DW, Whiteman M. The influence of maternal smoking during pregnancy on the toddler’s negativity. Archives of Pediatrics and Adolescent Medicine. 2000;154:381–385. doi: 10.1001/archpedi.154.4.381. [DOI] [PubMed] [Google Scholar]
- Brook, J. S., Pahl, T., Balka, E. B., & Fei, K. (in press). Smoking among New Yorican adolescents: Time 1 predictors of time 2 tobacco use. Journal of Genetic Psychology. [PubMed]
- Brook JS, Whiteman M, Czeisler LJ, Shapiro J, Cohen P. Cigarette smoking in young adults: Childhood and adolescent personality, familial, and peer antecedents. Journal of Genetic Psychology. 1997;158(2):172–188. doi: 10.1080/00221329709596660. [DOI] [PubMed] [Google Scholar]
- Brook JS, Whiteman M, Gordon AS, Brenden C. Older brother’s influence on younger sibling’s drug use. Journal of Psychology. 1983;114:83–90. doi: 10.1080/00223980.1983.9915400. [DOI] [PubMed] [Google Scholar]
- Chassin L, Presson CC, Todd M, Rose JS, Sherman SJ. Maternal socialization of adolescent smoking: the intergenerational transmission of parenting and smoking. Developmental Psychology. 1998;34(6):1189–1201. doi: 10.1037//0012-1649.34.6.1189. [DOI] [PubMed] [Google Scholar]
- Cheung YW. Ethnic identification and alcohol use among Canadian-born and foreign-born high school students in Toronto. International Journal of the Addictions. 1993;28(1):1095–1109. doi: 10.3109/10826089309056245. [DOI] [PubMed] [Google Scholar]
- Cleveland HH, Weibe RP. The moderation of adolescent-to-peer similarity in tobacco and alcohol use by school levels of substance use. Child Development. 2003a;74(1):279–291. doi: 10.1111/1467-8624.00535. [DOI] [PubMed] [Google Scholar]
- Cleveland HH, Weibe RP. The moderation of genetic and shared-environmental influences on adolescent drinking by levels of parental drinking. Journal of Studies on Alcohol. 2003b;62(2):182–194. doi: 10.15288/jsa.2003.64.182. [DOI] [PubMed] [Google Scholar]
- Cohen, J., Cohen, P., West, S. G., & Aiken, L. S. (2003). Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences (3rd ed.). Mahwah, NJ: Lawrence Erlbaum Associates.
- De Vries H, Backbier E. Self efficacy as an important determinant of quitting among pregnant women who smoke: The omega pattern. Preventive Medicine. 1994;23:167–174. doi: 10.1006/pmed.1994.1023. [DOI] [PubMed] [Google Scholar]
- De Vries H, Backbier E, Kok G, Dijkstra M. The impact of social influences in the context of attitude, self-efficacy, intention and previous behaviors as predictors of smoking onset. Journal of Applied Social Psychology. 1995;25:237–257. [Google Scholar]
- De Vries H, Kijkstra M, Kuhlman P. Self-efficacy the third factor besides attitude and subjective norm as a predictor of behavioural intention. Health Education Research. 1988;3:273–282. [Google Scholar]
- De Vries H, Engels R, Kremers S, Wetzels J, Mudde A. Parents’ and friends’ smoking status as predictors of smoking onset: findings from six European countries. Health Education Research. 2003;18(5):627–636. doi: 10.1093/her/cyg032. [DOI] [PubMed] [Google Scholar]
- Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L. The Hopkins Symptoms Checklist (HSCL): A self-report symptom inventory. Behavioral Science. 1974;19:1–15. doi: 10.1002/bs.3830190102. [DOI] [PubMed] [Google Scholar]
- Ennett ST, Bauman KE. The contribution of influence and selection to adolescent peer group homogeneity: The case of adolescent cigarette smoking. Journal of Personality and Social Psychology. 1994;67(4):653–663. doi: 10.1037//0022-3514.67.4.653. [DOI] [PubMed] [Google Scholar]
- Fagan, P., Brook, J. S., Rubenstone, E., & Zhang, C. (in press). Parental occupation, education, and smoking as predictors of offspring tobacco use in adulthood: A longitudinal study. Addictive Behaviors. [DOI] [PubMed]
- Griesler PC, Kandel DB. Ethnic differences in correlates of adolescent cigarette smoking. Journal of Adolescent Health. 1998;23(3):167–180. doi: 10.1016/s1054-139x(98)00029-9. [DOI] [PubMed] [Google Scholar]
- Guthrie BJ, Young AM, Williams DR, Boyd CJ, Kintner EK. African American girls’ smoking habits and day-to-day experiences with racial discrimination. Nursing Research. 2002;51(3):183–190. doi: 10.1097/00006199-200205000-00007. [DOI] [PubMed] [Google Scholar]
- Jackson, D. N. (1974). Personality research form. Goshen, NY: Research Psychologists Press.
- Jackson C. Initial and experimental stages of tobacco and alcohol use during late childhood: Relation to peer, parents, and personal risk factors. Addictive Behaviors. 1997;22(5):685–698. doi: 10.1016/s0306-4603(97)00005-1. [DOI] [PubMed] [Google Scholar]
- Jessor R. Risk behavior in adolescence: A psychosocial framework for understanding and action. Journal of Adolescent Health. 1991;12(8):597–605. doi: 10.1016/1054-139x(91)90007-k. [DOI] [PubMed] [Google Scholar]
- Jessor, R., & Jessor, S. L. (1977). Problem behavior and psychosocial development. New York: Academic Press.
- Kentala, J., Utriainen, P., Pahkala, K., & Matilla, K. (in press). Verification of adolescent self-reported smoking. Addictive Behaviors. [DOI] [PubMed]
- King G, Flisher AJ, Mallett R, Graham J, Lombard C, Rawson T, et al. Smoking in Cape Town: Community influence on adolescent tobacco use. Preventive Medicine. 2003;36:114–123. doi: 10.1006/pmed.2002.1128. [DOI] [PubMed] [Google Scholar]
- Kwate NO, Valdimarsdottir HB, Guevarra J, Bovbjerg DH. Experiences of racist events are associated with negative health consequences for African-American women. Journal of the National Medical Association. 2003;95(6):450–460. [PMC free article] [PubMed] [Google Scholar]
- Leff MK, Moolchan ET, Cookus BA, Spurgeon L, Evans LA, London ED, et al. Predictors of smoking initiation among at risk youth: A controlled study. Journal of Child and Adolescent Substance Abuse. 2003;13(1):59–76. [Google Scholar]
- Malan, M., & Leaver, R. (2003). Political change in South Africa: New tobacco control and public health policies. In J. de Beyer & L. Wverley Brigden (eds.), Tobacco control policy: Strategies, successes, and setbacks (pp. 121–153). Washington, D.C.: World Bank and Research for International Tobacco Control.
- Markham WA, Aveyard P, Thomas H, Charlton A, Lopez ML, De Vries H. What determines future smoking intentions of 12- to 13-year-old UK African-Caribbean, Indian, Pakistani and white young people? Health Education Research. 2004;19(1):15–28. doi: 10.1093/her/cyg008. [DOI] [PubMed] [Google Scholar]
- Markham WA, Featherstone K, Taket A, Trenchard-Mabere E, Ross M. Smoking amongst UK Bangladeshi adolescents aged 14–15. Health Education Research. 2001;16:143–156. doi: 10.1093/her/16.2.143. [DOI] [PubMed] [Google Scholar]
- McCaffery JM, Niaura R, Swan GE, Carmelli D. A study of depressive symptoms and smoking behavior in adult male twins from the NHLBI twin study. Nicotine and Tobacco Research. 2002;5(1):77–83. doi: 10.1080/14622200307259. [DOI] [PubMed] [Google Scholar]
- Mendis S. Tobacco use in a cohort of children in Sri Lanka. British Journal of Addiction. 1990;85(3):397–398. doi: 10.1111/j.1360-0443.1990.tb00656.x. [DOI] [PubMed] [Google Scholar]
- Mitchell SH. Measures of impulsivity in cigarette smokers and nonsmokers. Psychopharmacology. 1999;146(4):455–464. doi: 10.1007/pl00005491. [DOI] [PubMed] [Google Scholar]
- Panday S, Reddy SP, Bergstrom, E A qualitative study on the determinants of smoking behavior among adolescents in South Africa. Scandinavian Journal of Public Health. 2003;31(3):204–210. doi: 10.1080/14034940210164885. [DOI] [PubMed] [Google Scholar]
- Peltzer, K. (in press). Smokeless tobacco and cigarette use among black secondary school students in South Africa. Substance Use and Misuse. [DOI] [PubMed]
- Phinney JS. The multigroup ethnic identity measure: A new scale for use with diverse groups. Journal of Adolescent Research. 1992;7:156–176. [Google Scholar]
- Phinney JS, Chavira V, Williamson L. Acculturation attitudes and self-esteem among high school and college students. Youth and Society . 1992;23(93):299–312. [Google Scholar]
- Phinney, J. S., & Kohatsu, E. L. (1999). Ethnic and racial identity development and mental health. In J. Schulengerg, J. L. Maggs, & K. Hurrelmann (Eds.), Health risks and developmental transitions during adolescence (pp. 420–443). Cambridge, U.K.: Cambridge University Press.
- Reddy, P., & Swart, D. (2003, May). Preliminary report on Global Youth Tobacco Survey 2002. Prepared for World No Tobacco Day, Medical Research Council, KwaZulu-Natal, South Africa.
- Rohde P, Lewinsohn PM, Brown R. A. Gau, J. M, Kahler, C. W. Psychiatric disorders, familial factors and cigarette smoking: I. Associations with smoking initiation. Nicotine and Tobacco Research. 2003;5(1):85–98. doi: 10.1080/1462220031000070507. [DOI] [PubMed] [Google Scholar]
- Rose JS, Chassin L, Presson C. C. Clark, C. &, Sherman, S. J. Peer influences on adolescent cigarette smoking: A prospective sibling analysis. Merrill-Palmer Quarterly. 1999;45(1):62–84. [Google Scholar]
- Sampson RJ, Raudenbush SW, Earls F. Neighborhoods and violent crime: A multilevel study of collective efficacy. Science. 1997;277:918–924. doi: 10.1126/science.277.5328.918. [DOI] [PubMed] [Google Scholar]
- Santi S, Best JA, Brown KS, Cargo M. Social environment and smoking initiation. International Journal of the Addictions. 1990–91;25(7A8A):881–903. doi: 10.3109/10826089109071028. [DOI] [PubMed] [Google Scholar]
- Shek DTL. Economic stress, psychological well-being, and problem behavior in Chinese adolescents with economic disadvantage. Journal of Youth and Adolescence. 2003;32(4):259–266. [Google Scholar]
- Smith, G. M., & Fogg, C. P. (1979). Psychological antecedents of teenage drug use. In R. Simmons (Ed). Research in community and mental health: An annual compilation of research (Vol. 1, pp. 87–102). Greenwich, CT: JAI.
- Topolski TD, Patrick DL, Edwards TC, Huebner CE, Connell FA, Mount KK. Quality of life and health-risk behavior among adolescents. Journal of Adolescent Health. 2001;29:426–435. doi: 10.1016/s1054-139x(01)00305-6. [DOI] [PubMed] [Google Scholar]
- Unger JB, Chen X. The role of social networks and media receptivity in predicting age of smoking initiation: A proportional hazards model of risk and protective factors. Addictive Behaviors. 1999;24(3):371–381. doi: 10.1016/s0306-4603(98)00102-6. [DOI] [PubMed] [Google Scholar]
- van Walbeek, C. (2002). Personal communication. Cited in Malan, M., & Leaver, R. (2003). Political change in South Africa: New tobacco control and public health policies. In J. de Beyer & L. Wverley Brigden (eds.), Tobacco control policy: Strategies, successes, and setbacks (pp. 121–153). Washington, D.C.: World Bank and Research for International Tobacco Control.
- Williams DR. Race, socioeconomic status, and health. The added effects of racism and discrimination. Annals of the New York Academy of Sciences. 1999;896 :173–188. doi: 10.1111/j.1749-6632.1999.tb08114.x. [DOI] [PubMed] [Google Scholar]
- World Health Organization (2002). Reducing risks, promoting healthy life. Geneva, Switzerland: World Health Organization.