

Abstract
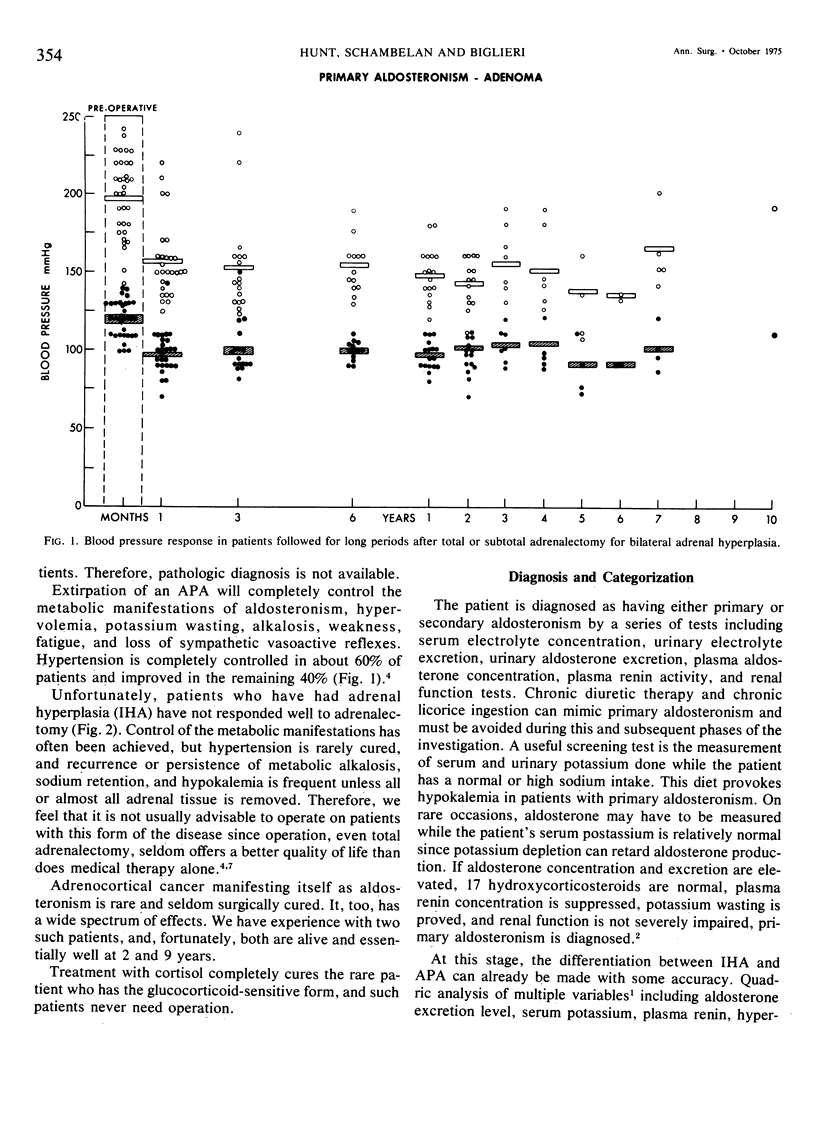
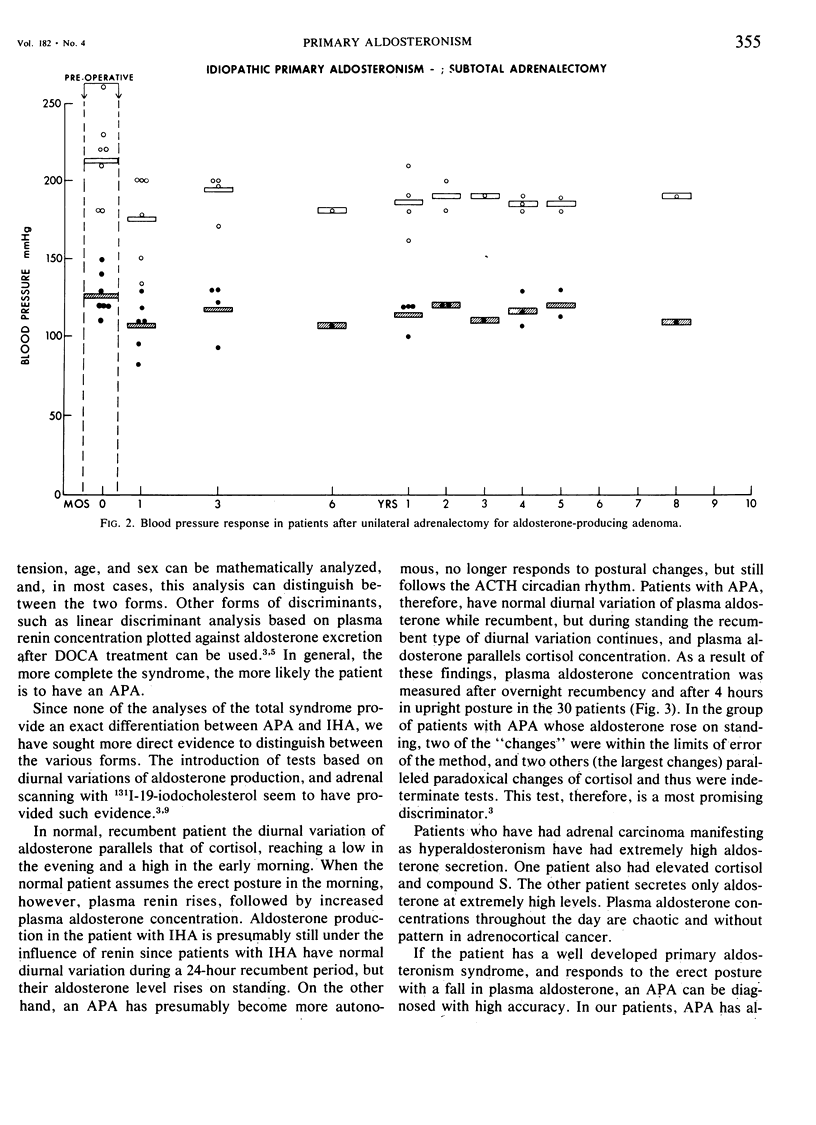
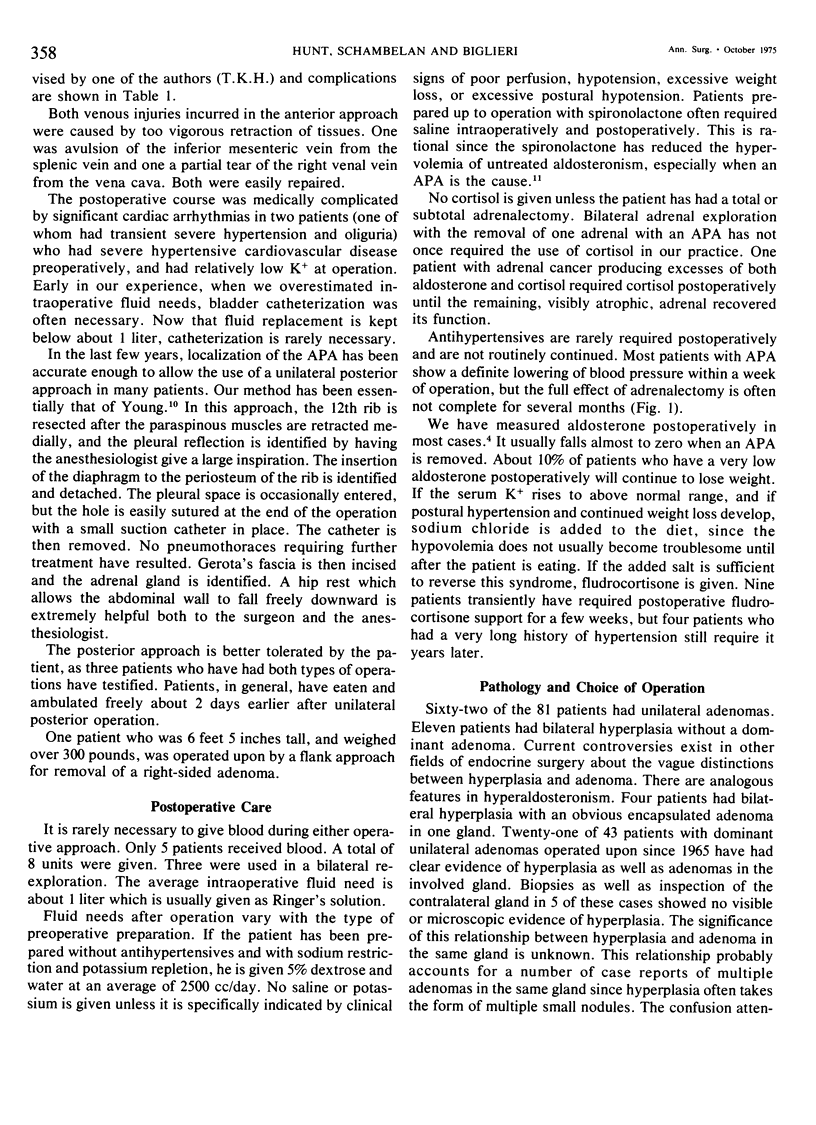
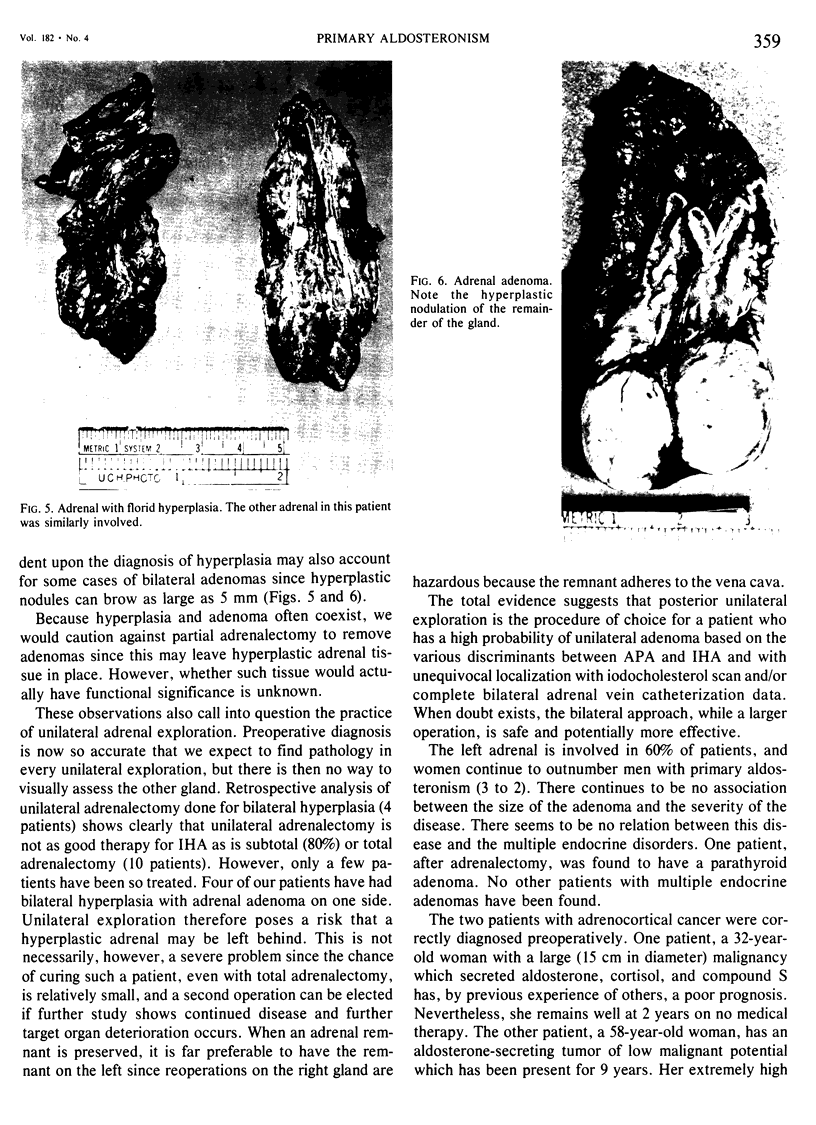
A system for discriminating between adrenal adenoma and hyperplasia based on the levels of aldosterone production, plasma renin concentration, severity of electrolyte disturbances, plasma aldosterone patterns during recumbency and after assuming erect posture, and 131I-19-iodocholesterol scan has been developed. Indicated for operation are patients with adenomas whose elevated blood pressure cannot be continuously controlled with usual doses of medication and patients with documented deterioration of target organ function. Adrenalectomy has been performed 83 times in 81 patients with a diagnosis of primary hyperaldosteronism. Results of excision of adrenal adenomas have been excellent with significant lowering of blood pressure in all cases and cure of hypertension in over 60%. Results of total or subtotal adrenalectomy for hyperplasia have been poor with almost all patients still requiring medication for hypertension. Adenomas have always been unilateral, and usually can be localized so that unilateral exploration is curative. Therefore, we have tried to distinguish preoperatively between adenoma and hyperplasia. Anterior transperitoneal adrenalectomy has been effective with few complications, and no postoperative hypercortisolism after unilateral adrenalectomy for adenoma. The unilateral extraperitoneal approach gives shorter morbidity and potentially fewer serious complications.
Full text
PDF
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aitchison J., Brown J. J., Ferriss J. B., Fraser R., Kay A. W., Lever A. F., Neville A. M., Symington T., Robertson J. I. Quadric analysis in the preoperative distinction between patients with and without adrenocortical tumors in hypertension with aldosterone excess and low plasma renin. Am Heart J. 1971 Nov;82(5):660–671. doi: 10.1016/0002-8703(71)90336-x. [DOI] [PubMed] [Google Scholar]
- Biglieri E. G., Schambelan M., Slaton P. E., Stockigt J. R. The intercurrent hypertension of primary aldosteronism. Circ Res. 1970 Jul;27(1 Suppl 1):195–202. [PubMed] [Google Scholar]
- Biglieri E. G., Stockigt J. R., Schambelan M. Adrenal mineralocorticoids causing hypertension. Am J Med. 1972 May;52(5):623–632. doi: 10.1016/0002-9343(72)90053-8. [DOI] [PubMed] [Google Scholar]
- Castleman B., Scully R. E., McNeely B. U. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 39-1972. N Engl J Med. 1972 Sep 28;287(13):656–663. doi: 10.1056/NEJM197209282871313. [DOI] [PubMed] [Google Scholar]
- Davis W. W., Newsome H. H., Jr, Wright L. D., Jr, Hammond W. G., Easton J., Bartter F. C. Bilateral adrenal hyperplasia as a cause of primary aldosteronism with hypertension, hypokalemia and suppressed renin activity. Am J Med. 1967 Apr;42(4):642–647. doi: 10.1016/0002-9343(67)90065-4. [DOI] [PubMed] [Google Scholar]
- Lieberman L. M., Beierwaltes W. H., Conn J. W., Ansari A. N., Nishiyama H. Diagnosis of adrenal disease by visualization of human adrenal glands with 131 I-19-iodocholesterol. N Engl J Med. 1971 Dec 16;285(25):1387–1393. doi: 10.1056/NEJM197112162852501. [DOI] [PubMed] [Google Scholar]
- Schambelan M., Howes E. L., Jr, Noakes C. A., Biglieri E. G. Role of renin and aldosterone in hypertension due to a renin-secreting tumor. Am J Med. 1973 Jul;55(1):86–92. doi: 10.1016/0002-9343(73)90153-8. [DOI] [PubMed] [Google Scholar]
- Silen W., Biglieri E. G., Slaton P., Galante M. Management of primary aldosteronism: evaluation of potassium and sodium balance, technic of adrenalectomy and operative results in 24 cases. Ann Surg. 1966 Oct;164(4):600–610. doi: 10.1097/00000658-196610000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]