

Abstract
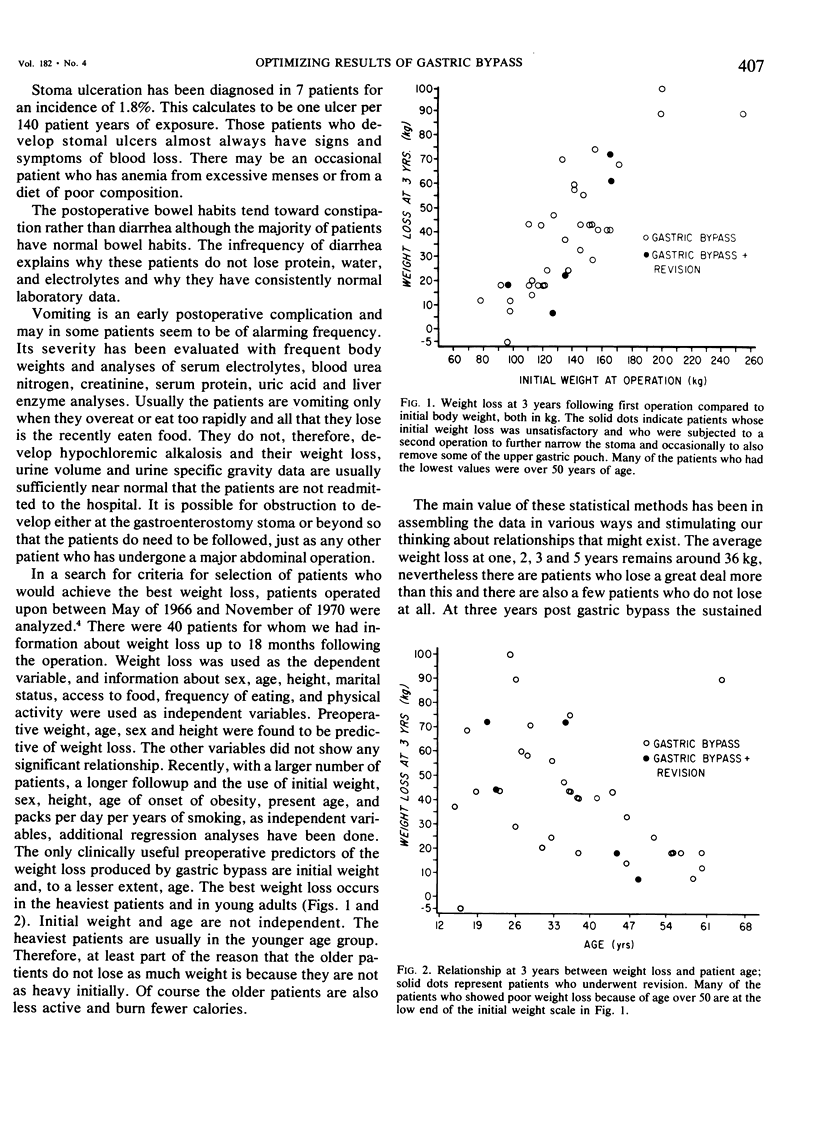
Gastric bypass is an extensive gastric exclusion operation used in patients who are more than twice their ideal weight. Most of the early postoperative deaths observed in 3% of 442 patients during the initial 9 years, could have been prevented by more attention to operative technique and early recognition and correction of leaks when they occurred. The best weight loss can be produced by adherence to three components of the operation: 1) Bypass of stomach and duodenum, 2) a small fundic segment and 3) a small (12 mm diameter) gastroenterostomy stoma. The average patient of 142 kg can expect to have a weight of around 107 kg at 1 year 103 kg at 5 years. Revision of a large stoma to a smaller (9 mm) diameter can induce further weight loss in some patients whose loss has been inadequate. The 1.8% incidence of stoma ulceration may be lowered with the present emphasis on a smaller fundic pouch, but could increase with longer observation. Presently stoma ulcers occur once in every 140 patient years at risk.
Full text
PDF







Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Blackburn G. L., Flatt J. P., Clowes G. H., Jr, O'Donnell T. F., Hensle T. E. Protein sparing therapy during periods of starvation with sepsis of trauma. Ann Surg. 1973 May;177(5):588–594. doi: 10.1097/00000658-197305000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freeman J. B., Meyer P. D., Printen K. J., Mason E. E., DenBesten L. Analysis of gallbladder bile in morbid obesity. Am J Surg. 1975 Feb;129(2):163–166. doi: 10.1016/0002-9610(75)90292-5. [DOI] [PubMed] [Google Scholar]
- Heimburger S. L., Steiger E., Lo Gerfo P., Biehl A. G., Williams M. J. Reversal of severe fatty hepatic infiltration after intestinal bypass for morbid obesity by calorie-free amino acid infusion. Am J Surg. 1975 Mar;129(3):229–235. doi: 10.1016/0002-9610(75)90229-9. [DOI] [PubMed] [Google Scholar]
- Ito C., Mason E. E., Besten L. D. Experimental studies on gastric bypass versus standard ulcer operations. Tohoku J Exp Med. 1969 Mar;97(3):269–277. doi: 10.1620/tjem.97.269. [DOI] [PubMed] [Google Scholar]
- Kongtahworn C., Foster E., Mason E. E., Printen K. J. Heparin-induced elevation of free fatty acids in diabetic patients. Surgery. 1973 Jul;74(1):30–33. [PubMed] [Google Scholar]
- Mason E. E., Gordy D. D., Chernigoy F. A., Printen K. J. Fatty acid toxicity. Surg Gynecol Obstet. 1971 Dec;133(6):992–998. [PubMed] [Google Scholar]
- Mason E. E., Ito C. Gastric bypass in obesity. Surg Clin North Am. 1967 Dec;47(6):1345–1351. doi: 10.1016/s0039-6109(16)38384-0. [DOI] [PubMed] [Google Scholar]
- Mason E. E., Ito C. Gastric bypass. Ann Surg. 1969 Sep;170(3):329–339. doi: 10.1097/00000658-196909010-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Printen K. J., Mason E. E. Gastric surgery for relief of morbid obesity. Arch Surg. 1973 Apr;106(4):428–431. doi: 10.1001/archsurg.1973.01350160046007. [DOI] [PubMed] [Google Scholar]
- Printen K. J., Paulk S. C., Liebschutz D., Mason E. E. Differential free fatty acid response to heparin in diabetics. Br J Surg. 1974 Mar;61(3):183–184. doi: 10.1002/bjs.1800610304. [DOI] [PubMed] [Google Scholar]
- Printen K. J., Paulk S. C., Mason E. E. Acute postoperative wound complications after gastric surgery for morbid obesity. Am Surg. 1975 Aug;41(8):483–485. [PubMed] [Google Scholar]
- Soper R. T., Mason E. E., Printen K. J., Zellweger H. Gastric bypass for morbid obesity in children and adolescents. J Pediatr Surg. 1975 Feb;10(1):51–58. doi: 10.1016/s0022-3468(75)80008-x. [DOI] [PubMed] [Google Scholar]
- Thomas J. W., Mason E. E. The effects of gastric exclusion operations on pancreatic exocrine secretion. Surgery. 1974 Mar;75(3):461–470. [PubMed] [Google Scholar]