

Abstract
A technique for repairing benign hilar hepatic duct strictures using transhepatic intubation with a large bore silastic stent is described. This procedure has been used in 10 patients. In 9 instances the stricture involved the common hepatic duct, and in one patient the right and left hepatic ducts. Nine of the strictures followed cholecystectomy; one followed the primary repair of a gun shot wound to the hepatic duct. Hepaticojejunostomies were created and the transhepatic silastic stent was left in place for 6 months in one patient, and for 12 months in 8 patients. In one patient the silastic stents are still in place. There have been no treatment failures. All patients are healthy and at full activity from one year, 3 months to 6 years, 6 months from the time of repair (average 3 years, 5 months). In the 9 patients whose stents have been removed, the serum bilirubin levels are normal There have been no episodes of cholangitis following repair. This method of repair using long term transhepatic silastic stents is recommended for all high hilar hepatic duct strictures.
Full text
PDF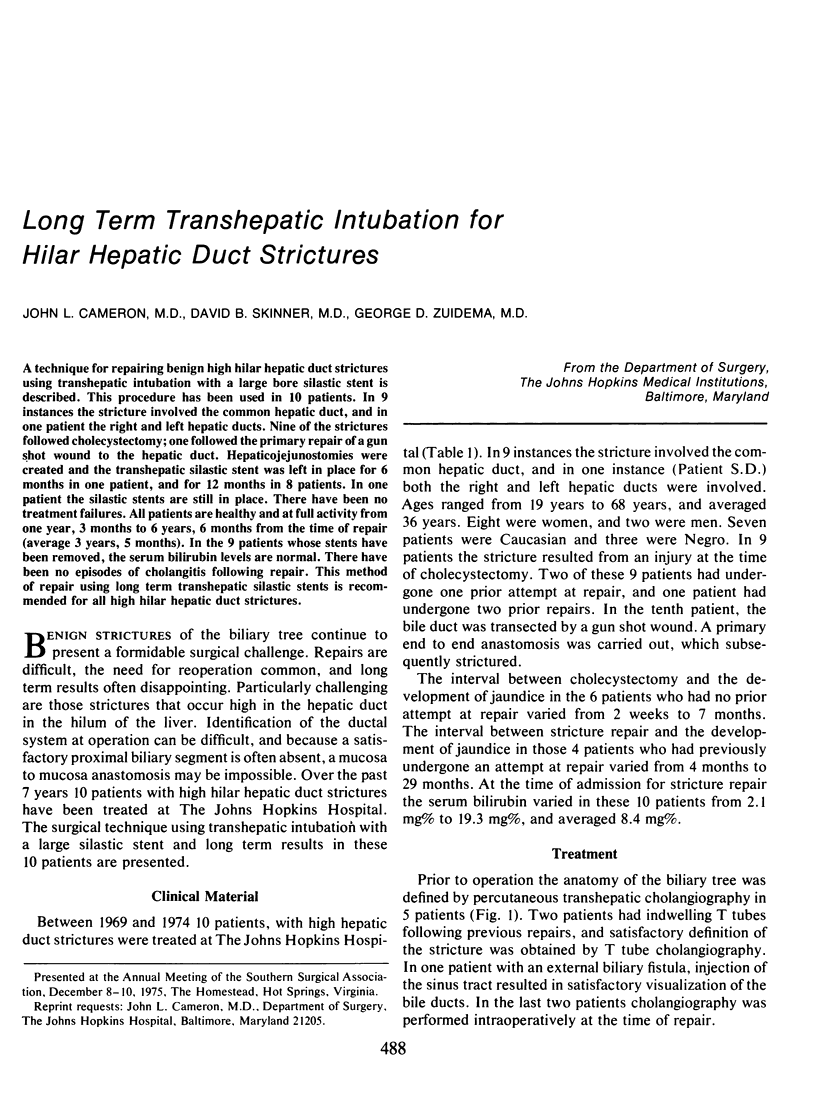
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Hertzer N. R., Gray H. W., Hoerr S. O., Hermann R. E. The use of T-tube splints in bile duct repairs. Surg Gynecol Obstet. 1973 Sep;137(3):413–418. [PubMed] [Google Scholar]
- Lane C. E., Sawyers J. L., Riddle D. H., Scott H. W., Jr Long-term results of Roux-en-Y hepatocholangiojejunostomy. Ann Surg. 1973 Jun;177(6):714–722. doi: 10.1097/00000658-197306000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Longmire W. P., Jr, Tompkins R. K. Lesions of the segmental and lobar hepatic ducts. Ann Surg. 1975 Oct;182(4):478–495. doi: 10.1097/00000658-197510000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SMITH R. HEPATICOJEJUNOSTOMY WITH TRANSHEPATIC INTUBATION: A TECHNIQUE FOR VERY HIGH STRICTURES OF THE HEPATIC DUCTS. Br J Surg. 1964 Mar;51:186–194. doi: 10.1002/bjs.1800510307. [DOI] [PubMed] [Google Scholar]
- WALTERS W., NIXON J. W., Jr, HODGINS T. E., RAMSDELL J. A. Strictures of the common and hepatic bile ducts; a study of more than four hundred operations, with one-to twenty-five-year follow-up. AMA Arch Surg. 1959 Jun;78(6):908–915. [PubMed] [Google Scholar]
- Warren K. W., Mountain J. C., Gray L. W., Jr Use of the modified Y tube splint in the repair of biliary strictures. Surg Gynecol Obstet. 1972 Apr;134(4):665–668. [PubMed] [Google Scholar]
- Warren K. W., Mountain J. C., Midell A. I. Management of strictures of the biliary tract. Surg Clin North Am. 1971 Jun;51(3):711–731. doi: 10.1016/s0039-6109(16)39447-6. [DOI] [PubMed] [Google Scholar]
- Way L. W., Dunphy J. E. Biliary stricture. Am J Surg. 1972 Aug;124(2):287–295. doi: 10.1016/0002-9610(72)90026-8. [DOI] [PubMed] [Google Scholar]
- Williams G. R. Experiences with surgical reconstruction of hepatic duct. Ann Surg. 1974 May;179(5):540–548. doi: 10.1097/00000658-197405000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]