

Abstract
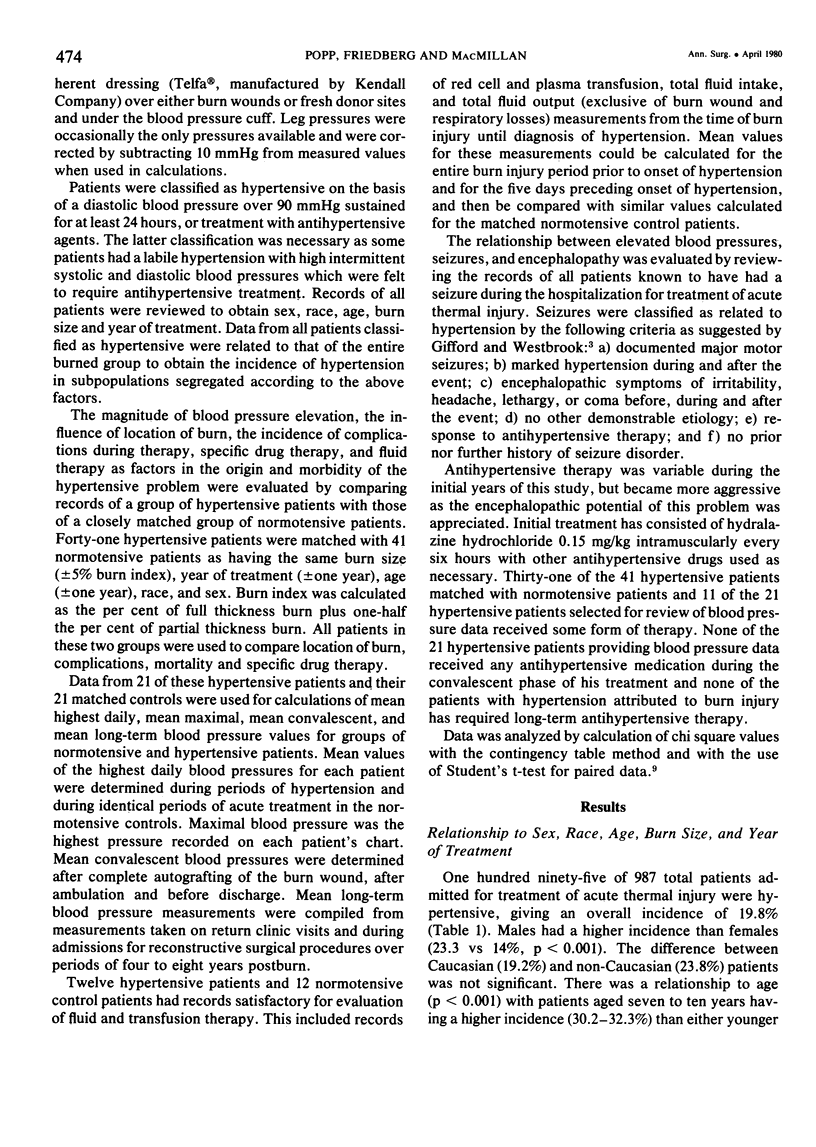
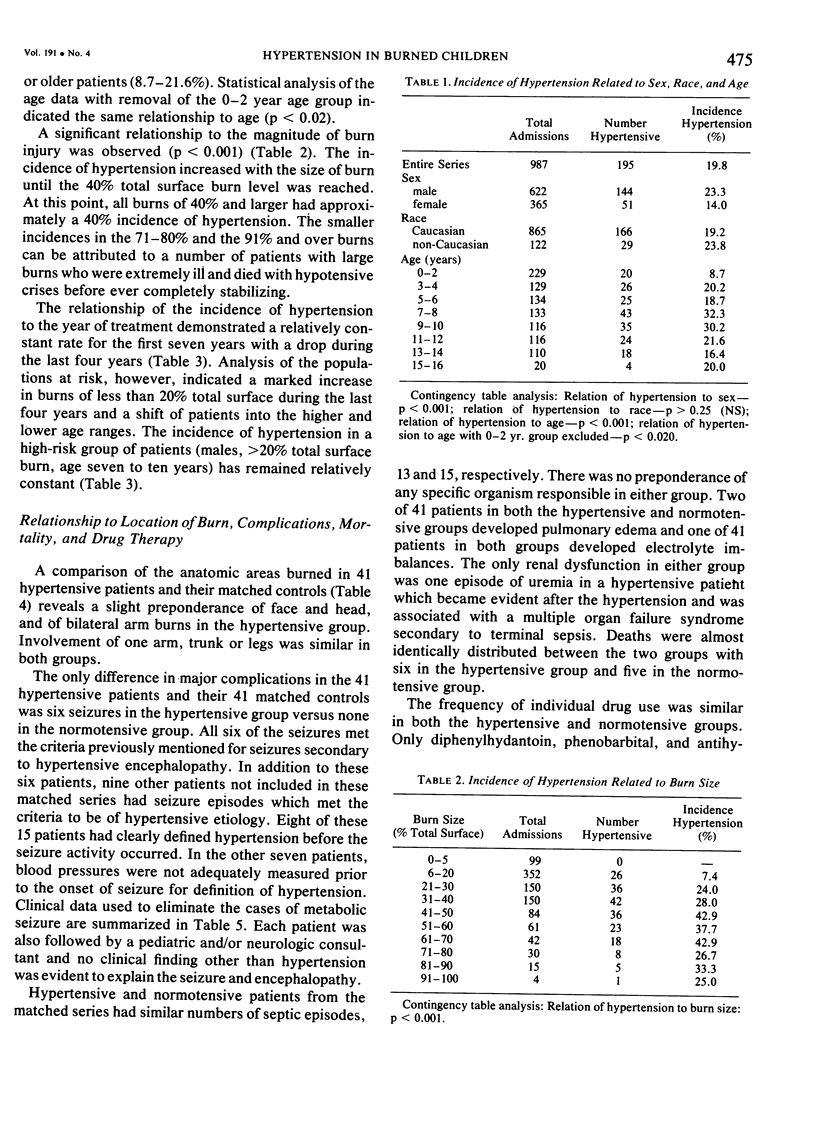
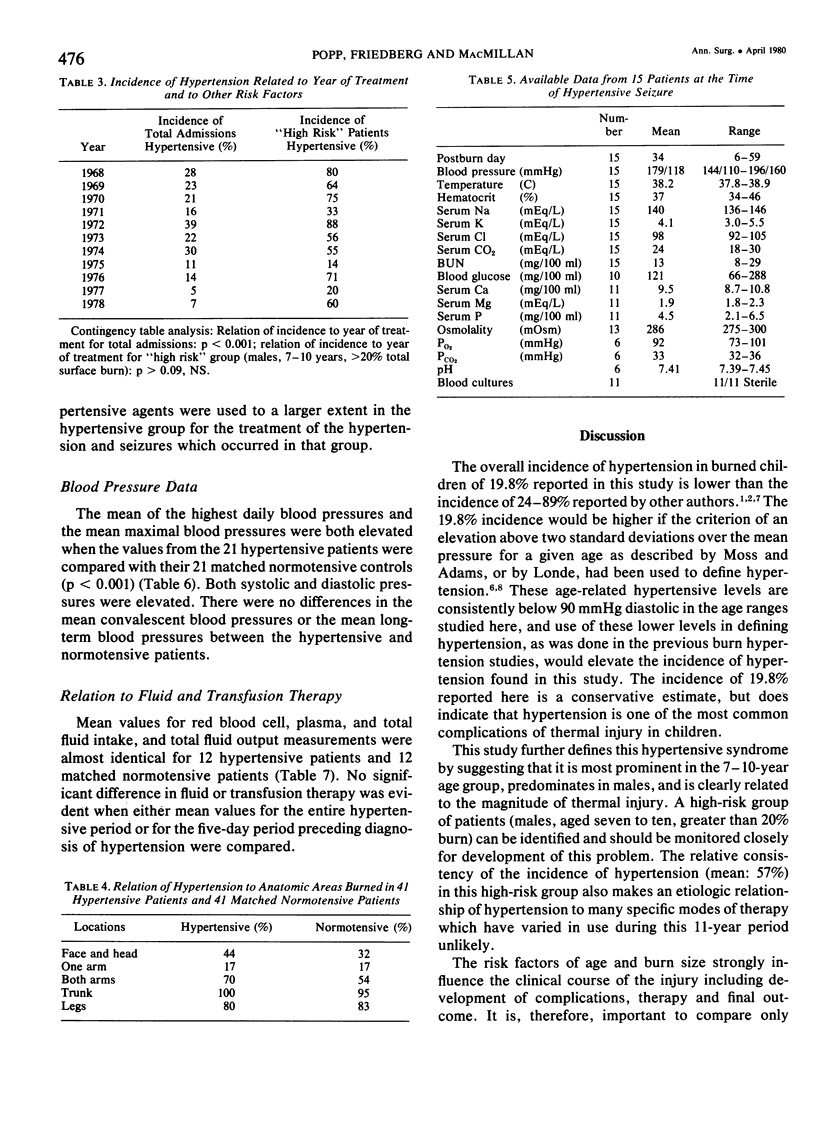
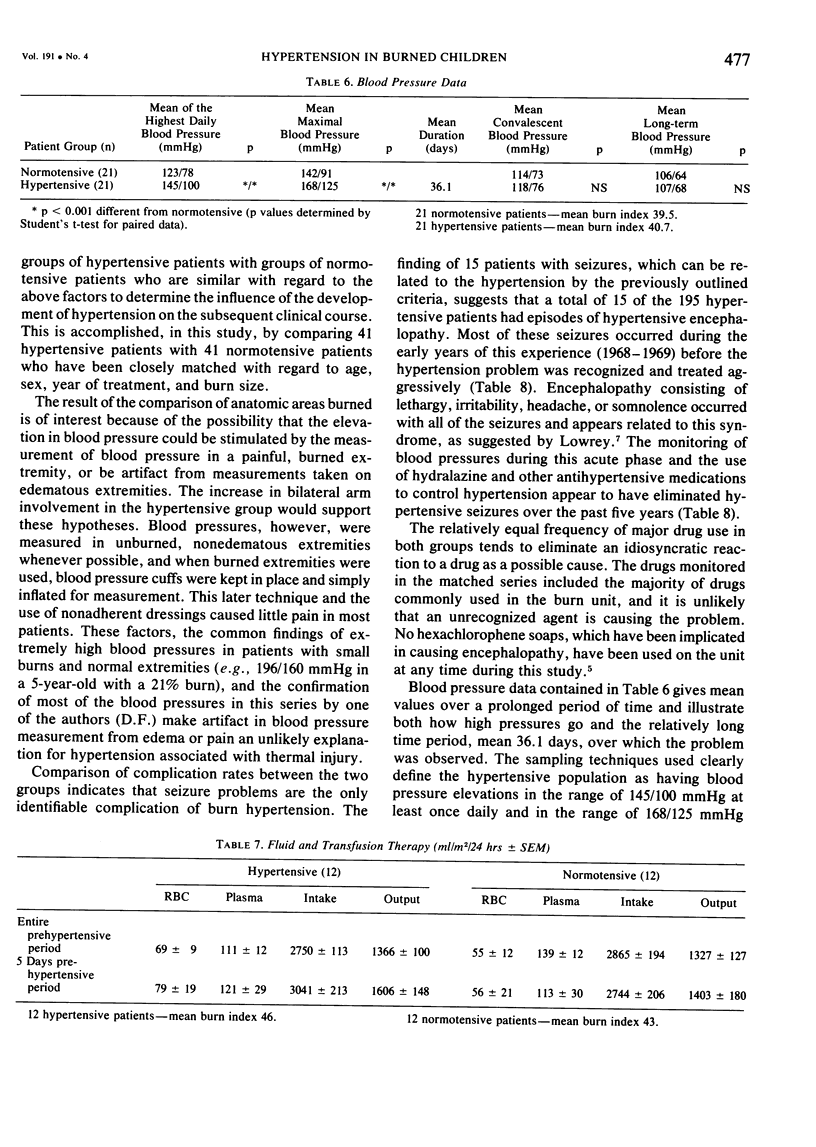
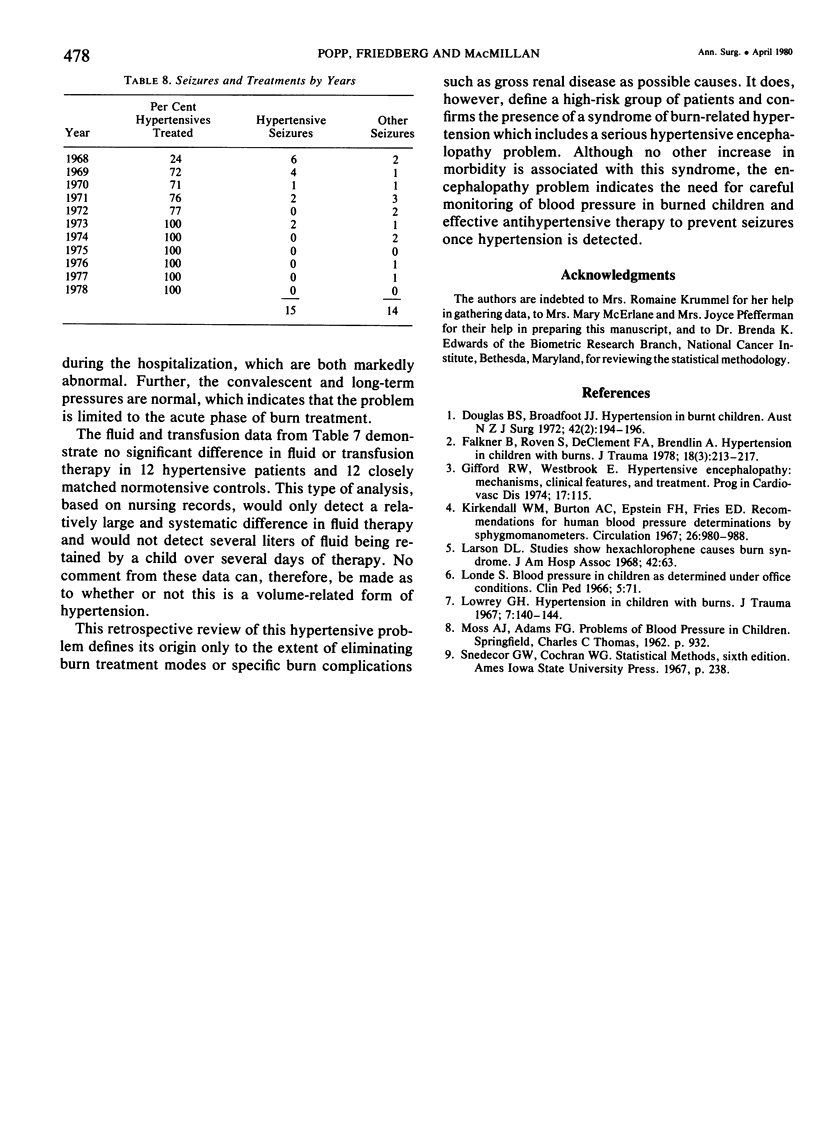
Although systemic arterial hypertension has been recognized as a common complication of thermal injury in children, its clinical characteristics have not been defined. This review of 987 burned children, treated over an 11-year period, documents development of hypertension in 195 patients (19.8%). The problem occurs most frequently in males and in the 7--10-year age group, but does not correlate with racial origin. Incidence increases with burn severity up to a 40% total surface burn. The incidence did not vary with the year of treatment when changes in patient population were eliminated. Fifteen of the 195 patients had hypertensive encephalopathy and seizure problems. No other complication or change in mortality could be related to hypertension. The problem could not be related to location of the burn wound, drug treatment, or differences in transfusion and fluid therapy. Comparison of the highest daily blood pressure measurements between matched hypertensive and normotensive groups demonstrated that the hypertensive and normotensive groups demonstrated that the hypertension is limited to the acute phase of burn wound treatment and that blood pressures are normal after complete autografting. The encephalopathy and seizure problems indicate the need for careful blood pressure monitoring and effective antihypertensive therapy in the treatment of burned children.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Douglas B. S., Broadfoot M. J. Hypertension in burnt children. Aust N Z J Surg. 1972 Nov;42(2):194–196. doi: 10.1111/j.1445-2197.1972.tb06778.x. [DOI] [PubMed] [Google Scholar]
- Falkner B., Roven S., DeClement F. A., Bendlin A. Hypertension in children with burns. J Trauma. 1978 Mar;18(3):213–217. doi: 10.1097/00005373-197803000-00011. [DOI] [PubMed] [Google Scholar]
- Gifford R. W., Jr, Westbrook E. Hypertensive encephalopathy: Mechanisms, clinical features, and treatment. Prog Cardiovasc Dis. 1974 Sep-Oct;17(2):115–124. doi: 10.1016/0033-0620(74)90026-7. [DOI] [PubMed] [Google Scholar]
- Kirkendall W. M., Burton A. C., Epstein F. H., Freis E. D. Recommendations for human blood pressure determination by sphygmomanometers. Circulation. 1967 Dec;36(6):980–988. doi: 10.1161/01.cir.36.6.980. [DOI] [PubMed] [Google Scholar]
- Larson D. L. Studies show hexachlorophene causes burn syndrome. Hospitals. 1968 Dec 16;42(24):63–64. [PubMed] [Google Scholar]
- Londe S. Blood pressure in children as determined under office conditions. Clin Pediatr (Phila) 1966 Feb;5(2):71–78. doi: 10.1177/000992286600500204. [DOI] [PubMed] [Google Scholar]
- Lowrey G. H. Sixth National Burn Seminar. Hypertension in children with burns. J Trauma. 1967 Jan;7(1):140–144. [PubMed] [Google Scholar]
- MOSS A. J. Blood pressure in children with diabetes mellitus. Pediatrics. 1962 Dec;30:932–936. [PubMed] [Google Scholar]