

Abstract
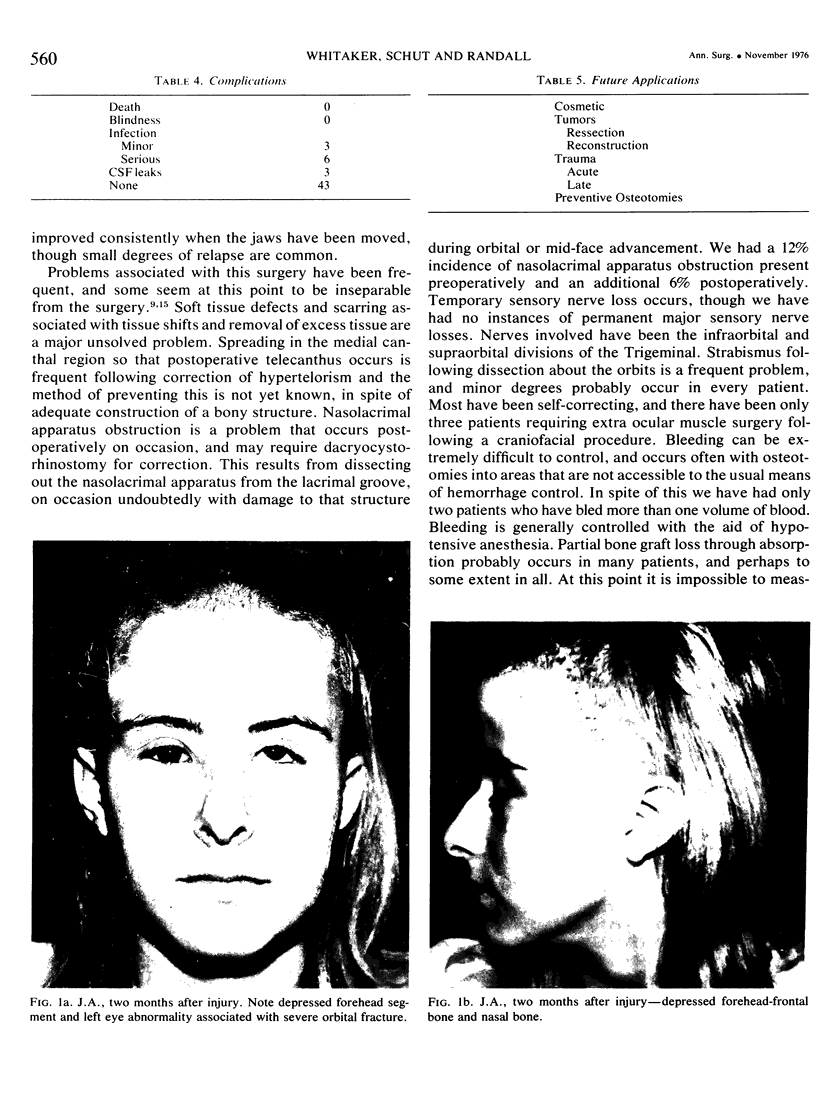
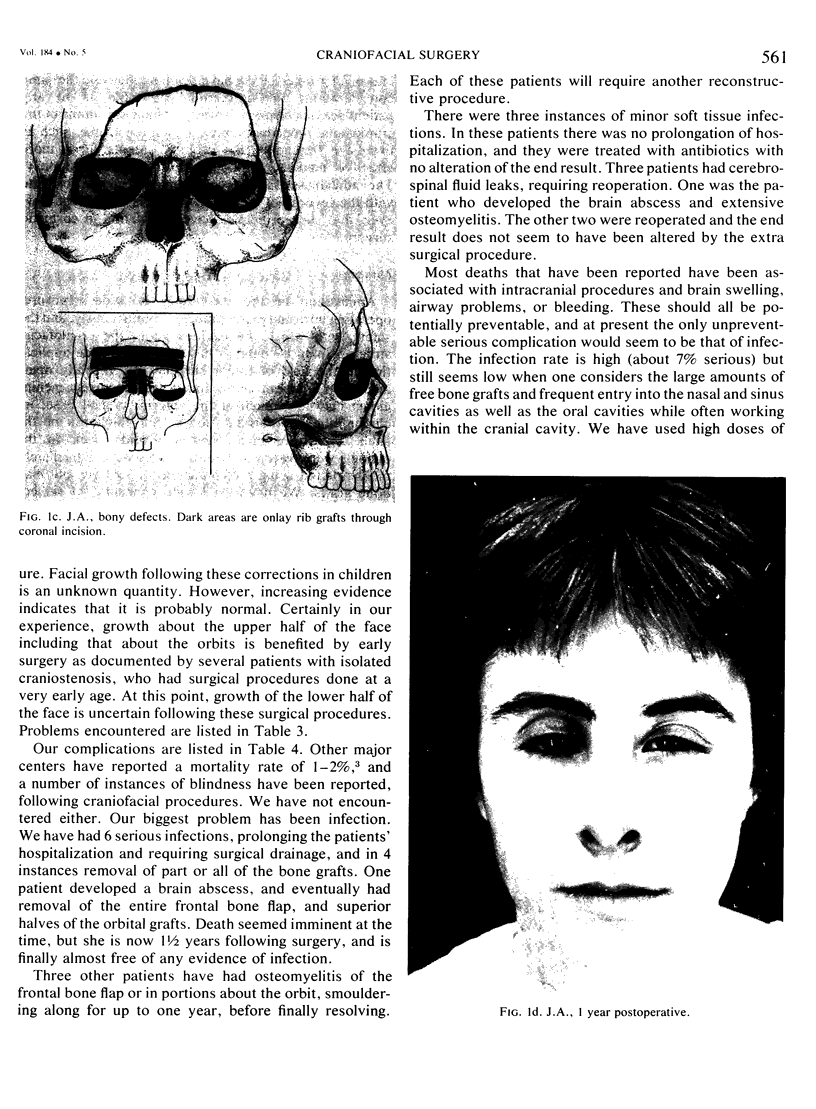
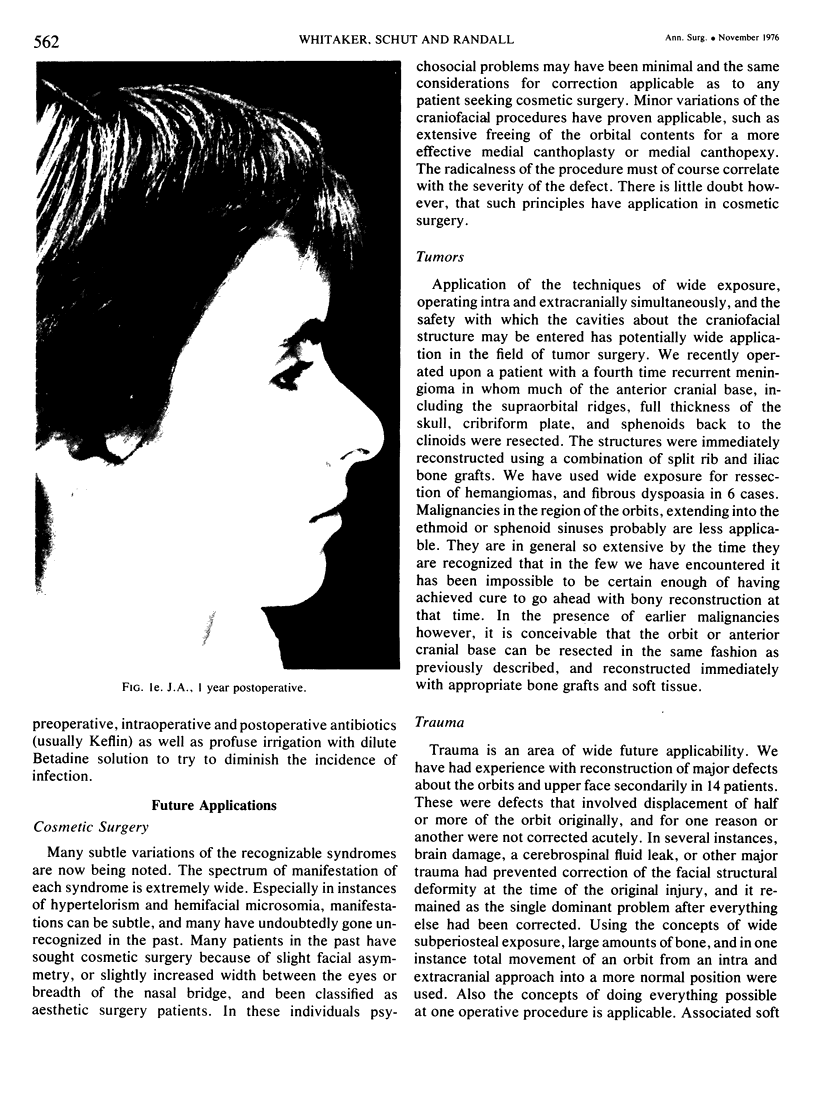
The possibilities for radical craniofacial restructuring have increased dramatically in the past 6 years with the development of craniofacial surgery. The field developed from a background of patients with major craniofacial birth defects allowing orderly planning and expansion to correction of a multitude of other craniofacial structural problems. The procedures concentrate upon changing the skeletal structures using extensive subperiostial dissection of soft tissue, and adding bone to fill in areas of deficiency. There are three grades of complexity in craniofacial procedures. After extensive soft tissue sub-periostial stripping about the orbits and upper face, the simplest form consists of onlay bone grafts. The next most complicated involves osteotomies to shift the face into a more normal position. In its most complicated form, abnormal proportions of bone are removed and the orbits or cranium are shifted into a new or normal position. We have had experience with 69 patients since September, 1972. Thirty-six have had intracranial procedures. Infection has been the most serious problem, and there have been no instances of death or blindness. A number of lesser problems occur. Future applications of craniofacial surgery are appearing with great frequency as more experience is gained with its uses. It has particular application in acute and late reconstruction of patients with traumatic defects about the face. Preventive osteotomies are an area with great potential, by releasing stenotic areas of bone and allowing the developing brain to mold the upper face and orbits. There is also applicability in surgery of tumors about the craniofacial structure and in cosmetic surgery.
Full text
PDF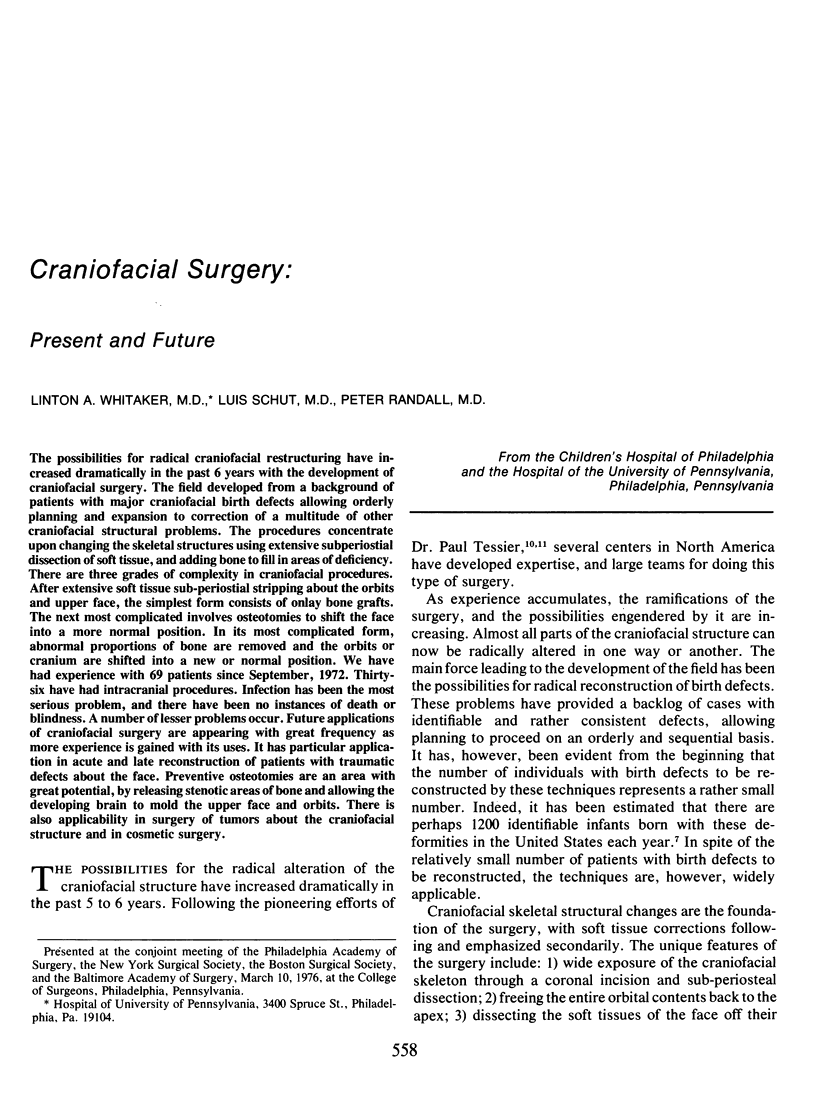



Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Converse J. M., Horowitz S. L., Coccaro P. J., Wood-Smith D. The corrective treatment of the skeletal asymmetry in hemifacial microsomia. Plast Reconstr Surg. 1973 Sep;52(3):221–232. doi: 10.1097/00006534-197309000-00001. [DOI] [PubMed] [Google Scholar]
- Converse J. M., Wood-Smith D., McCarthy J. G., Coccaro P. J. Craniofacial surgery. Clin Plast Surg. 1974 Jul;1(3):499–557. [PubMed] [Google Scholar]
- Converse J. M., Wood-smith D., McCarthy J. G. Report on a series of 50 craniofacial operations. Plast Reconstr Surg. 1975 Mar;55(3):283–293. [PubMed] [Google Scholar]
- Munro I. R. Orbito-cranio-facial surgery: the team approach. Plast Reconstr Surg. 1975 Feb;55(2):170–176. doi: 10.1097/00006534-197502000-00006. [DOI] [PubMed] [Google Scholar]
- Murray J. E., Swanson L. T. Mid-face osteotomy and advancement for craniosynostosis. Plast Reconstr Surg. 1968 Apr;41(4):299–306. doi: 10.1097/00006534-196804000-00001. [DOI] [PubMed] [Google Scholar]
- Tessier P. Experiences in the treatment of orbital hypertelorism. Plast Reconstr Surg. 1974 Jan;53(1):1–18. doi: 10.1097/00006534-197401000-00001. [DOI] [PubMed] [Google Scholar]
- Tessier P. The definitive plastic surgical treatment of the severe facial deformities of craniofacial dysostosis. Crouzon's and Apert's diseases. Plast Reconstr Surg. 1971 Nov;48(5):419–442. doi: 10.1097/00006534-197111000-00002. [DOI] [PubMed] [Google Scholar]
- Tessier P. Total osteotomy of the middle third of the face for faciostenosis or for sequelae of Le Fort 3 fractures. Plast Reconstr Surg. 1971 Dec;48(6):533–541. doi: 10.1097/00006534-197112000-00003. [DOI] [PubMed] [Google Scholar]