

Abstract
Small intestinal obstruction caused by 2 fibrous bands was found in a steer. Distended small intestine was palpable per rectum. Each band was located bilaterally between the caudal abdominal wall and the pelvic inlet. The compromised portion of intestine was considered nonviable and the animal was euthanized.
Résumé
Étranglement intestinal bilatéral chez un bouvillon castré. Une obstruction du petit intestin causée par 2 bandes fibreuses a été retrouvée chez un bouvillon. Le petit intestin distendu était palpable par le rectum. Chacune des bandes était située bilatéralement entre la paroi abdominale caudale et l’orifice pelvien. La portion lésée de l’intestin a été considérée non viable et l’animal a été euthanasié.
(Traduit par Docteur André Blouin)
Gut-tie or pelvic hernia, is a recognized condition in cattle practice. It refers to an obstruction that is thought to result from recoil of the spermatic cord following castration by traction in growing cattle (1–4). The presentation of cattle with obstructive intestinal disease often presents a diagnostic challenge and may have immediate life-threatening consequences. Several conditions may lead to obstruction of the flow of ingesta through the intestinal tract. Signs of obstructive intestinal disease include a reduction in the volume of, or failure to pass, feces; progressive abdominal distension with areas of tympanitic resonance on the right side of the abdomen; and colic (5). Differentiation of the causes of abdominal pain is primarily accomplished by physical examination, coupled with a skillfully obtained history. Clinical laboratory f indings may provide additional information. In some cases, exploratory surgery is necessary for a definitive diagnosis (6). This report describes the clinical presentation, the surgical approach, and the postmortem findings in a case of bilateral ‘gut-tie’ in a 6-month-old steer that was castrated by manual traction of the spermatic cord.
Case description
A 6-month-old, 246 kg Simmental steer was presented to the Atlantic Veterinary College, with a 5-day history of colic, depression, anorexia, and failure to pass feces. The steer had been castrated at approximately 2 mo of age by manual traction. The animal was healthy prior to the onset of this illness.
Upon presentation, the steer was anxious and uncomfortable. Examination revealed a heart rate of 140 beats/min, respiratory rate of 24 breaths/min, and a rectal temperature of 38.7°C. He was estimated to be 5% dehydrated. Bilateral abdominal distension was present, with the distension being more evident over the right paralumbar fossa. On abdominal auscultation, no ruminal contractions were heard over 3 min, and no other intestinal sounds could be detected. Fluid was audible by succussion of the right flank. Simultaneous auscultation and percussion of the abdomen yielded an area of tympanitic resonance, or ping, on the right side, which was consistent with fluid and gas accumulation. The ping occupied a well-delineated area about 8 cm in diameter, under the 13th rib. A rectal examination revealed an absence of feces in the rectum, and multiple distended loops of small intestine in the dorsocaudal part of the abdomen. It was not possible to examine the rest of the abdominal cavity via rectum due to the steer’s small size and intestinal distention. Transabdominal ultrasonographic examination was performed (3.5 MHz curvilinear transducer). The ultrasonographic examination of the area on the right side between the tuber coxae and the 8th intercostal space, and from the transverse processes of the vertebrae to the linea alba, on the right side, revealed numerous fluid-dilated loops of small intestine.
A tentative diagnosis of complete small intestinal strangulation and obstruction was made and the steer was prepared for a right-flank exploratory laparotomy.
Surgery was performed with the patient standing. The right paralumbar fossa was anesthetized by using 2% lidocaine hydrochloride in an inverted L block pattern. A 30-cm vertical incision was made in the right paralumbar fossa, beginning 10 cm ventral to the transverse processes of the lumbar vertebrae. The muscular layers and peritoneum were incised, and the peritoneal cavity was opened. Exploration of the peritoneal cavity revealed marked distention of the small intestine. The abomasum and cecum were in their correct anatomical positions and they were normal in size. A systematic exploration of the peritoneal cavity revealed that the small intestine was incarcerated within 2 tight fibrous bands, which extended from the caudal abdominal wall toward the pelvic inlet. The bands were palpable but could not be visualized. The incarcerated small intestine was estimated to be 125 cm long, grey, and edematous and was considered nonviable. Due to economic constraints, resection was not performed. The abdomen was closed in routine fashion and the animal was euthanized.
Necropsy revealed strangulation of the ileum at 2 points by 2 identical tubular bands. Each band measured approximately 0.5 cm in diameter and 53 cm in length and extended from the internal inguinal ring to the urethra. The more distal strangulation (Figure 1) was located approximately 15 cm from the ileocecal junction, while the other strangulation was approximately 40 cm proximal to the other strangulation. There were marked constrictions of the ileum at the areas of strangulation. The direction of incarceration (right to left or from left to right) was not established. A loose adhesion was present between the tubular bands and the ileal serosal surface. The segment of small intestine between the strangulated areas was dilated and had focal infarcts. Segments of small intestine proximal to the strangulation were distended with gas and digesta, while the cecum, colon, and rectum were empty.
Figure 1.
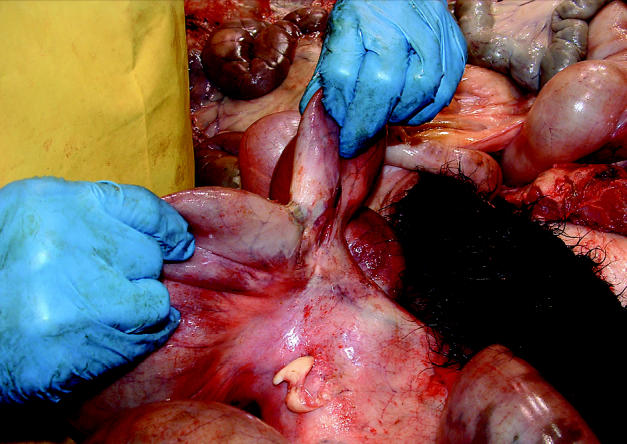
Photograph of the more distal strangulation located 15 cm from the ileocecal junction. There was marked constriction of the ileal wall with marked narrowing of the intestinal lumen and fibrin tags adherent to the serosal ileal surface.
The 2 tubular bands, which were traced to their openings at the urethra, were consistent with remnants of the ductus deferentes (Figure 2). Two bilateral rents in the mesoductus deferens allowed the involved small intestine to pass caudal to both ductus deferentes.
Figure 2.
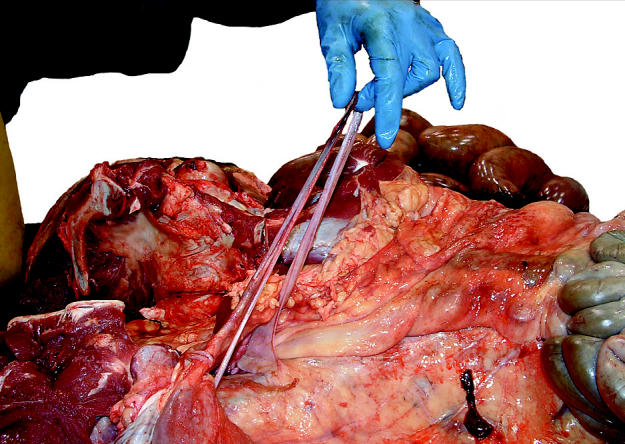
Photograph of the pathologist holding both edematous ductus deferens. Each ductus deferent was approximately 0.5 cm in diameter and 53 cm long.
Discussion
There are many causes of obstruction of the small intestine in cattle. Examples of small intestine obstruction in cattle are intussusception (7,8), volvulus (7,8), herniation through the right lateral ligament of the bladder (9), and strangulation by a persistent urachal remnant (10). Intestinal incarceration of the small intestine by remnants of the ductus deferens has also been described (1–4). It is predominantly only one spermatic cord, the right, which is involved in this condition (1). The case described in this report was considered unusual because the strangulation was bilateral.
Clinical signs of small intestinal obstruction in cattle include anorexia, depression, dehydration, tachycardia, and abdominal pain (7). The presence of right-sided abdominal tympanitic resonance (ping) is a consistent clinical finding in cattle with right displacement of the abomasum (11,12). Other less common causes of rightsided pings include abomasal volvulus, distension of the proximal colon, caecal distension or volvulus, pneumorectum, pneumoperitoneum, physometra, ileus, and distension of the small intestine (7,12–14). Other signs frequently observed in small intestinal obstruction include a marked decrease in fecal output and bilateral abdominal distention. Multiple loops of distended small intestine are usually palpable per rectum (7). In this steer, there was no suggestion of an internal hernia in the inguinal region on rectal examination. The steer’s small size and the intestinal distention made transrectal examination of the abdomen difficult. During early stages of small intestine entrapment, transrectal palpation may have revealed the presence of fibrous bands or entrapment of small intestine in the inguinal region. If rectal examination is not considered appropriate because of the steer’s small size or intestinal distension, transabdominal ultrasonography may be a useful alternative diagnostic tool. In cases of intestinal obstruction or ileus, dilated loops of small intestine may be detected ultrasonographically. If the obstruction is at the level of the jejunum or ileum, at least 5 dilated loops of intestine are likely to be found when the right flank is examined ultrasonographically (15).
Gut-tie has been recognized in cattle practice for many years. The condition has been associated with open castration of cattle by traction of the spermatic cord, which may result in either retraction of the spermatic cord into the abdomen with adhesion formation and obstruction or incarceration of intestine or, as in this steer, traction of the spermatic cord may tear the peritoneal fold of the ductus deferens which attaches the ductus to the abdominal wall, permitting loop(s) of intestine to pass through this hiatus and resulting in incarceration (3). Overt signs of abdominal pain in steers after open castration and traction of the spermatic cord, may indicate gut-tie. This condition of intestinal entrapment by the ductus deferens can be corrected by right flank laparotomy and transection of the fibrous band. In addition, manual rupture of this fibrous band transrectum has been advocated (1); however, there is a risk of rupturing the rectum by this method. Alternate means of castration that prevent disruption of the abdominal mesoductus may prevent development of this condition (4).
Acknowledgments
The authors thank Drs. P. Rose and M. Wichtel for their constructive comments. CVJ
References
- 1.Anreiter J. Uber die strangulation ductospermatica. Wien Tieraerztl Monatsschr. 1951;38:359–366. [Google Scholar]
- 2.O’Connor JP. A case of pelvic hernia or “gut-tie” in a bullock. Irish Vet J. 1972;25:251–252. [Google Scholar]
- 3.Scott PR, Kinder AE, Blake NA, Hawe C. ‘Gut-tie’ in a recently castrated steer. Vet Rec. 1997;140:559–560. doi: 10.1136/vr.140.21.559. [DOI] [PubMed] [Google Scholar]
- 4.Wolfe DF, Mysinger PW, Carson RL, Powers RD, Rice DN. Incarceration of a section of small intestine by remnants of the ductus deferens in steers. J Am Vet Med Assoc. 1987;191:1597–1598. [PubMed] [Google Scholar]
- 5.Hoffsis GF, McGuirk SM. Diseases of the abomasum and the intestinal tract. In: Howard JL, ed. Current Veterinary Therapy: Food Animal Practice 2. Philadelphia: WB Saunders, 1986:724–737.
- 6.Guard C. Obstructive intestinal diseases. In: Smith BP, ed. Large Animal Internal Medicine. 2nd ed. Philadelphia: Mosby, 1996:880–885.
- 7.Pearson H, Pinsent PJ. Intestinal obstruction in cattle. Vet Rec. 1977;101:162–166. doi: 10.1136/vr.101.9.162. [DOI] [PubMed] [Google Scholar]
- 8.Horney FD, Wallace CE. Surgery of the bovine digestive tract. In: Jennings PB, ed. Practice of Large Animal Surgery, Vol 1. Philadelphia: WB Saunders, 1984:493–554.
- 9.Trent AM, Bailey JV. Herniation of small intestine through the right lateral ligament of the bladder in a bull. Can Vet J. 1985;26:16–19. [PMC free article] [PubMed] [Google Scholar]
- 10.Baxter GM, Darien BJ, Wallace CE. Persistent urachal remnant causing intestinal strangulation in a cow. J Am Vet Med Assoc. 1987;191:555–558. [PubMed] [Google Scholar]
- 11.Robertson JM. Diagnosis of left displacement of the bovine abomasum. J Am Vet Med Assoc. 1965;146:820–827. [PubMed] [Google Scholar]
- 12.Smith DF, Erb HN, Kalaher KM, Rebhun WC. The identification of structures and conditions responsible for right side tympanitic resonance (ping) in adult cattle. Cornell Vet. 1982;72:180–199. [PubMed] [Google Scholar]
- 13.Rebhun WC. Right abdominal tympanitic resonance in dairy cattle: identifying the causes. Vet Med. 1991;86:1135–1142. [Google Scholar]
- 14.Hull BL. Differential diagnosis of the right sided ‘ping’. Bovine Practit. 1982;17:72–74. [Google Scholar]
- 15.Braun U, Marmier O, Pusterla N. Ultrasonographic examination of the small intestine of cows with ileus of the duodenum, jejunum or ileum. Vet Rec. 1995;137:209–215. doi: 10.1136/vr.137.9.209. [DOI] [PubMed] [Google Scholar]