

Abstract
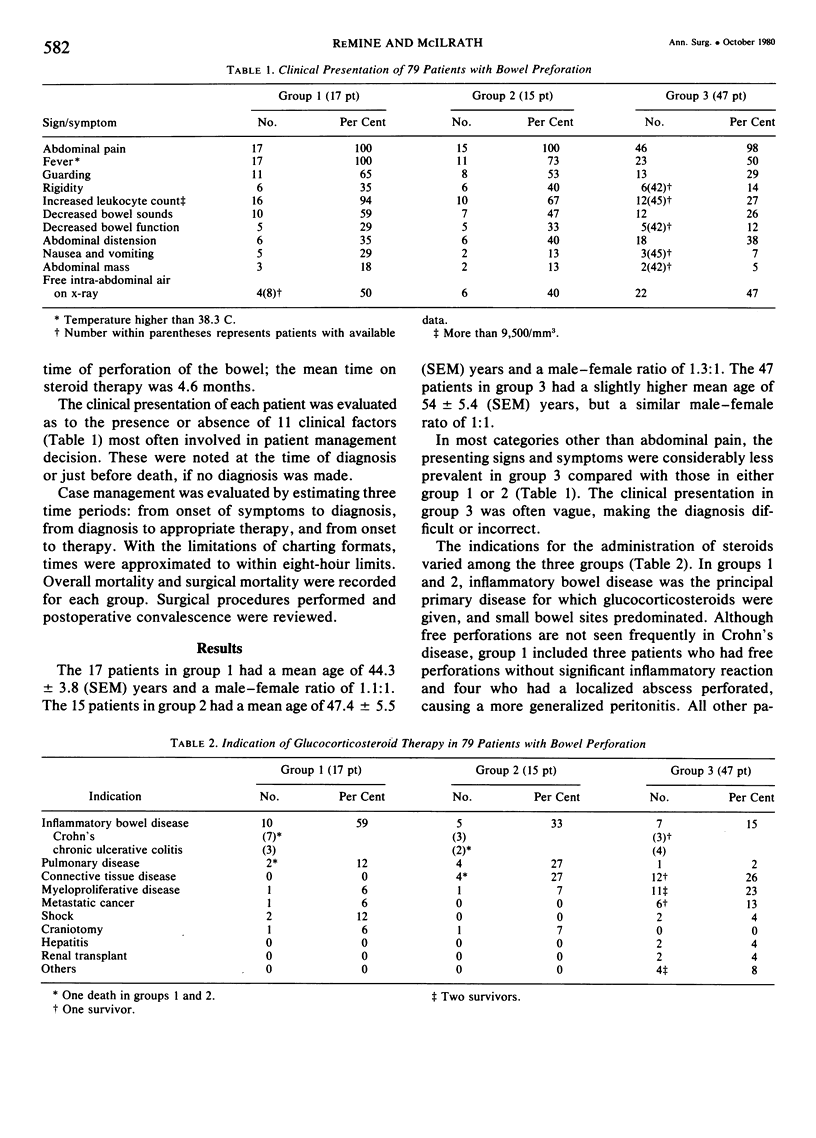
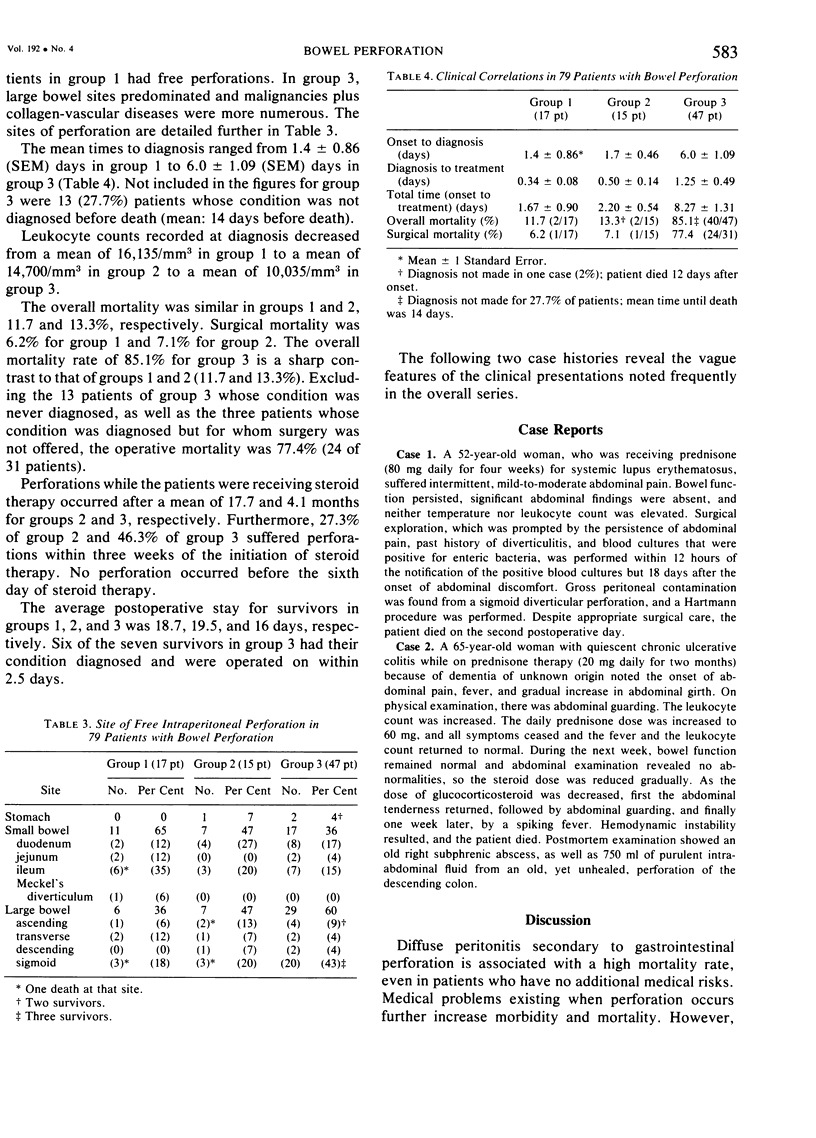
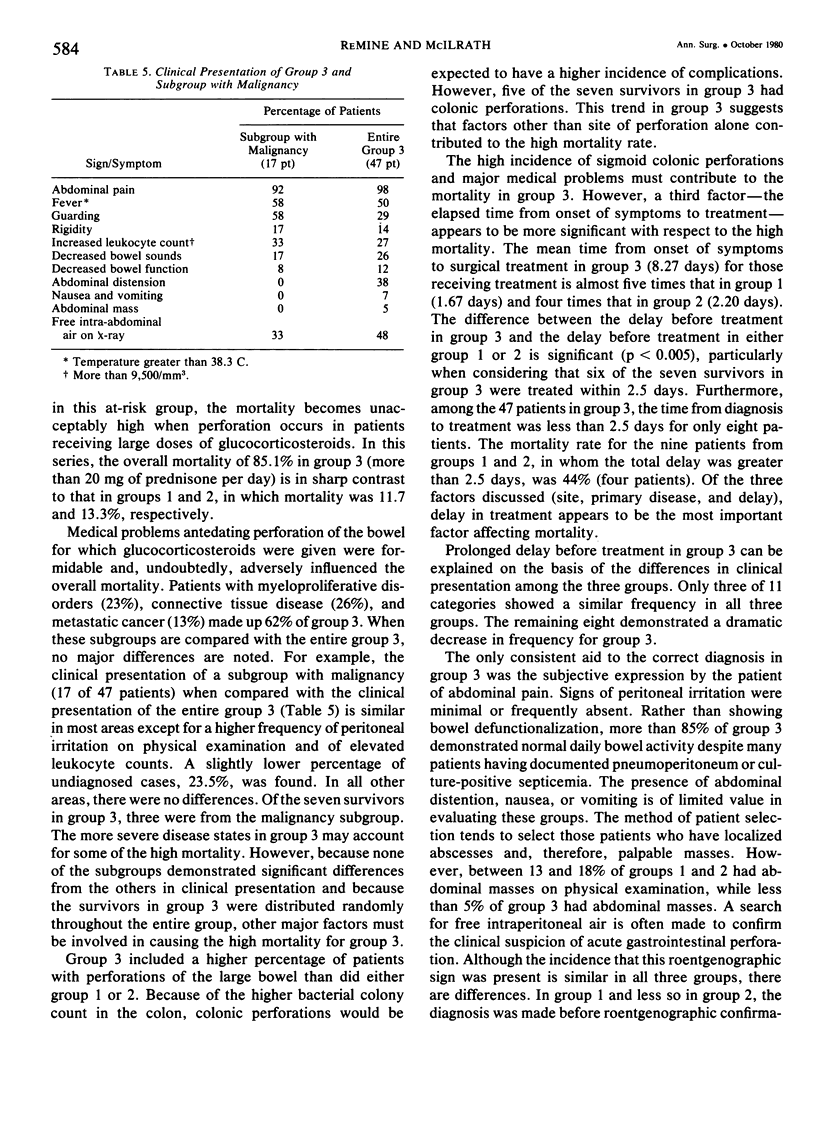
Gastrointestinal perforation in patients receiving glucocorticosteroid (GCS) therapy has been reported to have mortality rates as high as 100%. From 79 patients seen during a nine-year period, three groups were formed according to GCS dosage: group 1 (steroid perioperative coverage), group 2 (low-dose steroids, prednisone < 20 mg daily), and group 3 (high-dose steroids, prednisone greater than or equal to 20 mg daily). Of 11 clinical presentation factors, only abdominal tenderness was consistently present in group 3. The mean delay from onset of symptoms to treatment for group 3 was 8.3 days and was in marked contrast to that for group 1 or 2, 1.7 and 2.2 days, respectively (p < 0.005). Mortality increased from 11.8% in group 1 to 13.3% in group 2 to 85% in group 3. High-dose GCS therapy decreased the clinical expression of peritonitis to the point that recognition and, therefore, treatment of gastrointestinal perforation were markedly delayed. In a patient receiving high-dose GCS, a high degree of clinical suspicion must accompany any new abdominal discomfort, and aggressive diagnostic efforts should be made to establish the cause. If abdominal pain persists, surgical exploration should be considered.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BECK J. C., BROWNE J. S. L., JOHNSON L. G., KENNEDY B. J., MacKENZIE D. W. Occurrence of peritonitis during ACTH administration. Can Med Assoc J. 1950 May;62(5):423–426. [PMC free article] [PubMed] [Google Scholar]
- Balow J. E., Hurley D. L., Fauci A. S. Immunosuppressive effects of glucocorticosteroids: differential effects of acute vs chronic administration on cell-mediated immunity. J Immunol. 1975 Mar;114(3):1072–1076. [PubMed] [Google Scholar]
- Claman H. N. Corticosteroids and lymphoid cells. N Engl J Med. 1972 Aug 24;287(8):388–397. doi: 10.1056/NEJM197208242870806. [DOI] [PubMed] [Google Scholar]
- DOWNS J. W., COOPER W. G., Jr Surgical complications resulting from ACTH and cortisone medication. Am Surg. 1955 Feb;21(2):141–146. [PubMed] [Google Scholar]
- FEIN B. T. Perforation and inflammation of diverticula of the colon secondary to long-term adrenocorticosteroid therapy for bronchial asthma and pulmonary emphysema. South Med J. 1961 Apr;54:355–359. doi: 10.1097/00007611-196104000-00003. [DOI] [PubMed] [Google Scholar]
- Fauci A. S., Dale D. C., Balow J. E. Glucocorticosteroid therapy: mechanisms of action and clinical considerations. Ann Intern Med. 1976 Mar;84(3):304–315. doi: 10.7326/0003-4819-84-3-304. [DOI] [PubMed] [Google Scholar]
- Gill W., Wilson S., Long W. B., 3rd Steroid hypothermia. Surg Gynecol Obstet. 1978 Jun;146(6):944–946. [PubMed] [Google Scholar]
- Glenn F., Grafe W. R., Jr Surgical complications of adrenal steroid therapy. Ann Surg. 1967 Jun;165(6):1023–1034. doi: 10.1097/00000658-196706000-00017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MARKOWITZ A. M. The less common perforations of the small bowel. Ann Surg. 1960 Aug;152:240–257. doi: 10.1097/00000658-196008000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Menguy R. Surgical management of free perforation of the small intestine complicating regional enteritis. Ann Surg. 1972 Feb;175(2):178–189. doi: 10.1097/00000658-197202000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PALMER T. H., Jr, MASON P. J., ADAMS A. C. Diverticulitis of the colon with perforation during cortisone and ACTH therapy. J Maine Med Assoc. 1955 Dec;46(12):349–351. [PubMed] [Google Scholar]
- SAUER W. G., DEARING W. H., WOLLAEGER E. E. Serious untoward gastrointestinal manifestations possibly related to administration of cortisone and corticotropin. Proc Staff Meet Mayo Clin. 1953 Nov 18;28(23):641–649. [PubMed] [Google Scholar]
- SAUTTER R. D., ZIFFREN S. E. Adrenocortical steroid therapy resulting in unusual gastrointestinal complications. AMA Arch Surg. 1959 Aug;79(2):346–356. doi: 10.1001/archsurg.1959.04320080182021. [DOI] [PubMed] [Google Scholar]
- SLOAN S., BRIGGS J. D., HALSTED J. A. ACTH therapy for ulcerative colitis complicated by perforation of coexisting peptic ulcer. Gastroenterology. 1951 Jul;18(3):438–442. [PubMed] [Google Scholar]
- Sterioff S., Orringer M. B., Cameron J. L. Colon perforations associated with steroid therapy. Surgery. 1974 Jan;75(1):56–58. [PubMed] [Google Scholar]
- TULIN M., KERN F., Jr, ALMY T. P. Perforation of bowel during treatment of ulcerative colitis with corticotropin; report of three cases. J Am Med Assoc. 1952 Oct 11;150(6):559–562. doi: 10.1001/jama.1952.03680060031010. [DOI] [PubMed] [Google Scholar]
- Warshaw A. L., Welch J. P., Ottinger L. W. Acute perforation of the colon associated with chronic corticosteroid therapy. Am J Surg. 1976 Apr;131(4):442–446. doi: 10.1016/0002-9610(76)90154-9. [DOI] [PubMed] [Google Scholar]
- Zurier R. B., Weissman G. Anti-immunologic and anti-inflammatory effects of steroid therapy. Med Clin North Am. 1973 Sep;57(5):1295–1307. doi: 10.1016/s0025-7125(16)32230-1. [DOI] [PubMed] [Google Scholar]