

Abstract
We investigated cosmetic outcomes of the midline sternotomy incision. A randomized clinical trial was conducted in 60 patients who underwent surgery through a midline sternotomy incision. Patients were divided into groups A (n=30) and B (n=30). In addition, the incision line was also divided into 2 regions (upper and lower halves) in each group. In group A, the upper half of the skin was closed with absorbable 4-0 braided polyglycolic acid sutures (Sentesor®, Boz; Ankara, Turkey), and the lower half was closed with 4-0 nonabsorbable monofilamentous polypropylene suture (Monoplen®, Boz), and vice versa in group B. Scar width and height were measured and photographed at the 6th postoperative month.
In both groups, the lower part of the incision showed inferior cosmetic results, regardless of the suture material (P < 0.05). On the other hand, the upper part of the incision in group A (the area of absorbable polyglycolic acid sutures) was significantly more hypertrophic.
We conclude that monofilament nylon sutures diminish the risk of hypertrophic scarring, in comparison with absorbable sutures. In the lower half of the sternotomy scar, increased tension and relative mobility of the skin over the xiphoid process lead to inferior cosmetic results, regardless of the suture material used.
Key words: Cardiac surgical procedures; cicatrix, hypertrophic/etiology/pathology; keloid/etiology; skin/injuries; sternum/surgery; surgical procedures, operative/methods; sutures
Hypertrophic scar and keloid formation due to surgery is a well discussed topic. It is also related to suture material, and many studies have been performed to find the most suitable material. Some investigators have found no difference between absorbable and nonabsorbable materials, whereas others have obtained better results with nonabsorbable monofilament nylon sutures.1–3
Personal susceptibility to scar formation is another important factor and usually is not related to suture material.2 As this might be a factor in the conflicting results published in the literature, we tried to eliminate personal variations by applying both of the suture materials in the same patients.
Another, less studied topic is the cause of differences in scar size. For example, scar size varies in various parts of midline sternotomy and laparotomy incisions.3,4 In our experience, a few patients have manifested a prominent hypertrophic scar, especially in the lower zone of the incision (Fig. 1). We have wondered why the scar size was not the same throughout the whole incision line. In this study, we investigated the appearance of the scar in different parts of the sternotomy incision, and we also compared the outcome of different suture materials.
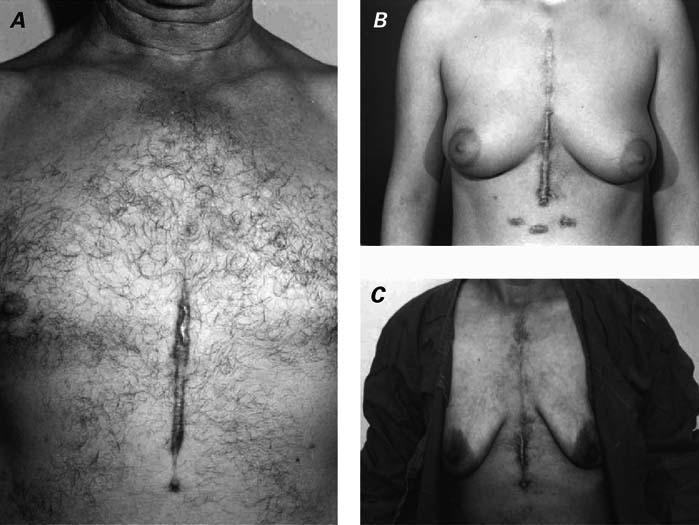
Fig. 1 Median sternotomy scars in a man (A) and in 2 women (B, C) show stretching of the lower half of the scar.
Patients and Methods
Sixty-six consecutive patients undergoing median sternotomy for cardiac surgery were studied from February 2003 through January 2004. They had no accompanying diseases such as diabetes mellitus or renal insufficiency. All those studied were patients in the department of cardiovascular surgery of our hospital. Patients were informed, and the ethical committee of the medical faculty approved the study. Patients were randomly assigned to the groups. We excluded 2 patients who required revision, 2 who died, and 2 who had wound-healing problems. The effective study population was therefore 60 patients: 30 in group A and 30 in group B. Forty-four (73%) were men and 16 (27%) were woman. The mean age was 56.5 years (range, 23–70 years).
Deep sternal closure was always the same: the sternum was approximated with 5 interrupted 5-gauge monofilament steel wires. The presternal fascia and the rectus sheet were closed with 1-0 monofilament polydiaxone, and subcutaneous tissue was closed with continuous 3-0 polyglycolic acid suture. In group A (Fig. 2A), the upper and lower parts of the skin were sutured in subcuticular continuous fashion with absorbable 4-0 braided polyglycolic acid sutures (Sentesorb®, Boz; Ankara, Turkey) and 4-0 nonabsorbable monofilamentous polypropylene suture (Monoplene®, Boz), respectively. The knots were tied outside the skin at the beginning of the incision, at the transition zone between polypropylene and polyglycolic acid suture, and at the end of the incision. In group B, the same materials were used for skin closure, but in reverse manner (Fig. 2B).
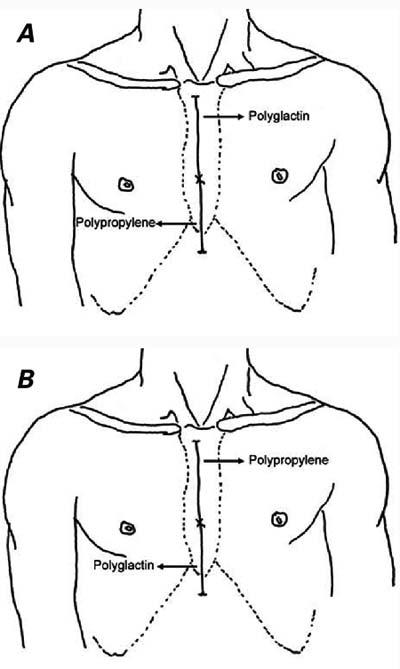
Fig. 2 Study design of A) group A, and B) group B.
Postoperatively, wound care was performed daily. Monoplene sutures were removed 8 to 10 days after surgery, and the wounds were inspected for serous or purulent discharge. The patients were then seen 6 months after surgery. The scar was measured for width and height, and a color photograph was taken of each wound.
Statistical analysis was performed in collaboration with the department of bio-statistics. The SPSS statistical package (version 9.05) (SPSS Inc.; Chicago, Ill) was used for assessing the data. In evaluating the data, we calculated the difference of 2 means and 2 related samples, and we performed χ2 tests and correlation analysis.
Results
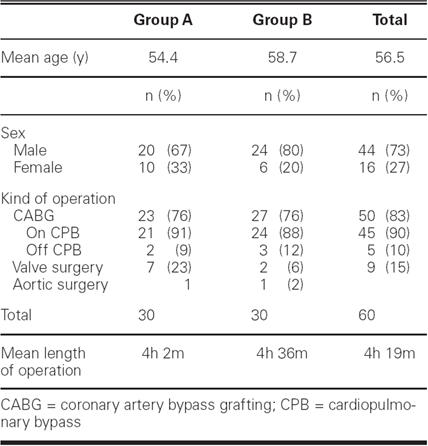
Patient and surgical characteristics are shown in Table I. Most of the patients (n=50, 83%) underwent surgery for coronary artery disease, 9 (15%) for valvular heart disease, and 1 (2%) for aortic surgery. The female-to-male ratio in groups A and B were 1:3 and 1:4, respectively. There was no statistical difference between groups regarding age, sex, length of operation, and type of surgery (Table I).
TABLE I. Distribution and Characteristics of the Patients
The mean values of scar measurements are shown in Table II. The widest scar was 10 mm in width and the narrowest was 1 mm. The highest scar rose 3 mm above the surface of the surrounding skin, and the lowest rose 0.5 mm. In both groups, both the scar width and the scar height were nearly 2-fold greater in the lower half than in the upper half (Fig. 3), and the differences were statistically significant (P < 0.05). The scar height in the upper sternum was almost 2-fold greater in group A (the Sentesorb site) (Fig. 4) than in group B (the Monoplene® site) (0.63 mm versus 0.31 mm). This was a significant finding (P < 0.05).
TABLE II. Scar Measurements of the 2 Groups
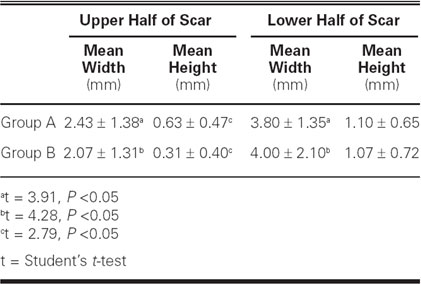

Fig. 3 Photograph illustrates a hypertrophic lower scar (polyglactin area) in a patient in group B.

Fig. 4 Photograph illustrates a hypertrophic upper scar (polyglactin area) in a patient in group A.
Discussion
A scar is usually judged as excellent, good, acceptable, or poor in the literature.1 Rather than apply these subjective categories, we chose to use metric measurements to increase objectivity. We found that the lower half of the sternotomy incision has a greater tendency towards hypertrophic scar formation, regardless of the suture materials. Elliot and colleagues,3 in one of the most important published studies on scar formation in presternal incisions, found that scar stretching occurs most frequently in the lower third of the scar overlying the xiphoid process and extending onto the abdomen. In their study, the incision line was divided into upper, middle, and lower thirds for evaluation. They found, in women, that the middle third of the incision scar showed a significantly greater incidence of marked hypertrophy than did the upper third. They attributed this to the lateral forces exerted by female breasts. In our study, we divided the incision line into 2 regions, as we investigated the effects of different suture materials. We did not observe any regional difference between male and female patients; however, this topic should be investigated in well-designed clinical studies.
It is known that hypertrophic scar and keloid formation are closely related to skin tension. Increased tension contributes to inferior cosmetic results.5,6 The lower half of the presternal area, including the xiphoid process through the upper abdomen, contains more tissue elements (such as subcutaneous fat, the rectus sheet, and muscle). The skin tension is less in the lower sternum; therefore, it is expected that better cosmetic results should be achieved in the lower zone. Our finding is contrary to that hypothesis. Meyer and McGrouther6 systematically studied presternal scars by obtaining punch-biopsy specimens from cadavers. They determined 8 measurement points from the “angle of Louis” to the xiphoid process and from there to the umbilicus; these points were equidistant. At every point, they calculated the ratio of transverse to vertical diameter of the scar. They found a significant difference between the sternum and the upper abdomen: “According to our interpretation, the lines of tension over the sternum act in all directions, whereas over the upper abdomen the overwhelming tension is acting predominantly in the horizontal plane.”6 They explained the difference with “tension directions;” we also speculate that, due to the comparative mobility of the lower half of the presternal area, more suture material is used to approximate those tissues, which can lead to increased scar formation.
There has been controversy on the scar-forming effects of polyglycolic acid.7,8 We encountered greater scar size in the Sentesorb site of group A (Fig. 4). Therefore, we suggest using monofilament nylon sutures for sternotomy skin closure.
This study showed us that obtaining inferior cosmetic results in the lower half of the sternotomy incision is unavoidable. Nonetheless, we believe that better overall cosmetic results can be achieved with use of nonabsorbable monofilament nylon sutures in skin.
Footnotes
Address for reprints: Melih Kaptanoglu, MD, PK: 702, Sivas 58141, Turkey
E-mail: mkaptan@cumhuriyet.edu.tr
References
- 1.Lista FR, Thomson HG. The fate of sternotomy scars in children. Plast Reconstr Surg 1988;81:35–9. [DOI] [PubMed]
- 2.Niessen FB, Spauwen PH, Kon M. The role of suture material in hypertrophic scar formation: Monocryl vs. Vicryl-rapide. Ann Plast Surg 1997;39:254–60. [DOI] [PubMed]
- 3.Elliot D, Cory-Pearce R, Rees GM. The behaviour of presternal scars in a fair-skinned population. Ann R Coll Surg Engl 1985;67:238–40. [PMC free article] [PubMed]
- 4.Trimbos JB, Smeets M, Verdel M, Hermans J. Cosmetic result of lower midline laparotomy wounds: polybutester and nylon skin suture in a randomized clinical trial. Obstet Gynecol 1993;82:390–3. [PubMed]
- 5.Berman B, Flores F. The treatment of hypertrophic scars and keloids. Eur J Dermatol 1998;8:591–5. [PubMed]
- 6.Meyer M, McGrouther DA. A study relating wound tension to scar morphology in the pre-sternal scar using Langer's technique. Br J Plast Surg 1991;44:291–4. [DOI] [PubMed]
- 7.Gabel EA, Jimenez GP, Eaglstein WH, Kerdel FA, Falanga V. Performance comparison of nylon and an absorbable suture material (Polyglactin 910) in the closure of punch biopsy sites. Dermatol Surg 2000;26:750–3. [DOI] [PubMed]
- 8.Parell GJ, Becker GD. Comparison of absorbable with nonabsorbable sutures in closure of facial skin wounds. Arch Facial Plast Surg 2003;5:488–90. [DOI] [PubMed]