

Abstract
Dissection of the interventricular septum due to an aneurysm of the left sinus of Valsalva is a very rare cardiac condition. We report a case in which we used a modified Bentall procedure for aortic root replacement in reoperating on a sinus of Valsalva aneurysm that had dissected into the interventricular septum.
Key words: Aneurysm, dissecting/surgery, aortic aneurysm/complications, aortic valve insufficiency, heart block/etiology, heart septum/pathology/surgery, heart valve prosthesis, sinus of Valsalva/surgery
An unruptured, acquired aneurysm of the left sinus of Valsalva that causes dissection of the interventricular septum is extremely rare. Several techniques, including resection of the aneurysm or simple closure of the aneurysm's mouth, have been reported for surgical correction.1–4 In the presence of aortic valve disease, total aortic root replacement is an another surgical method for the treatment of this rare clinical condition in order to prevent the necessity of reoperation. We report the case of a patient in whom closure of the aneurysm with a patch in the presence of an aortic valve prosthesis resulted in paravalvular leak and patch detachment 1 year later.
Case Report
Due to rheumatic aortic valve insufficiency, a 39-year-old man had undergone aortic valve replacement 6 years before his current presentation. For the last 2 years, the patient had worn a permanent pacemaker because of complete atrioventricular block. One year before the current presentation, he had undergone reoperation, for a left sinus of Valsalva aneurysm that had dissected into the interventricular septum.5 During that reoperation, the 25-mm aortic valve prosthesis (Sulzer Carbomedics; Austin, Tex) had been found to function normally and to be in its correct position, with no annular disease. The sac of the unruptured left sinus of Valsalva aneurysm that extended toward the interventricular septum had been obliterated, and the orifice of the aneurysm had been closed with a Dacron patch. The patient had been discharged from the hospital without complication. His postoperative course had been uneventful for 10 months, but for the last 2 months he had experienced effort dyspnea and fatigue. The patient's functional capacity had deteriorated to New York Heart Association (NYHA) functional class III, and transthoracic echocardiography revealed severe systolic dysfunction of the left ventricle, moderate aortic paravalvular leak, and an enlarged dissecting aneurysm of the interventricular septum due to patch detachment (Fig. 1).
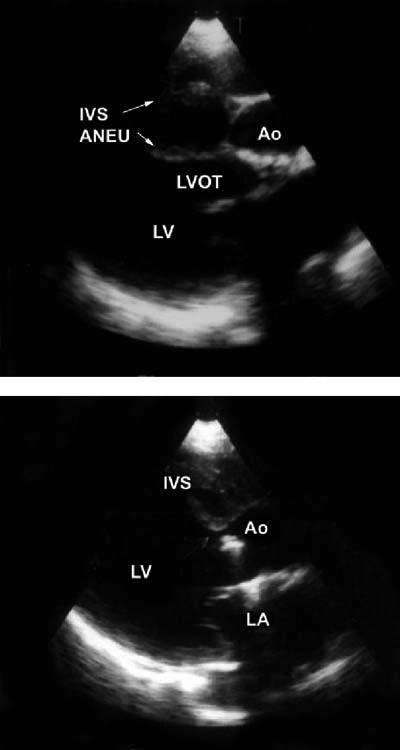
Fig. 1 Echocardiography reveals a 4- × 2- × 4-cm dissecting aneurysm of the interventricular septum and an aortic paravalvular leak.
ANEU = aneurysm; Ao = aorta; IVS = interventricular septum; LA = left atrium; LV = left ventricle; LVOT = left ventricular outflow tract
In April 2004, the patient was taken for a 2nd reoperation, under elective conditions, to completely correct the aortic root disease. The operation was performed via median sternotomy, with mild hypothermic cardiopulmonary bypass. The ascending aorta was opened, and an aortic annular leak was detected between the rim of the previously placed prosthetic valve and the patch. Detachment of the patch from the orifice of the aneurysm of the left sinus of Valsalva was also seen (Fig. 2). The root of the ascending aorta, including the annulus and the sinuses of Valsalva, was fragile; therefore, the previously placed patch, aortic valve prosthesis, and suture remnants were removed, and total replacement of the aortic root was performed with a flanged composite graft that we prepared intraoperatively: this consisted of a 28-mm Dacron woven graft (Terumo, Vascutek Ltd.; Renfrewshire, Scotland) and a 23-mm bileaflet mechanical prosthesis (St. Jude Medical, Inc.; St. Paul, Minn). We trimmed the flanged part of the graft to 1.5 cm in length in order to correct the aortic annular condition.6 The orifice of the aneurysm of the left sinus of Valsalva was obliterated by means of separate Teflon-pledgeted 3-0 Prolene sutures. In addition, Teflon-pledgeted 3-0 Prolene horizontal mattress sutures were placed deeply from the aortic annulus to the flange of the conduit for proximal anastomosis of the composite graft. Both coronary buttons were implanted into the graft, and then the distal end of the graft was anastomosed to the ascending aorta. The patient was weaned from cardiopulmonary bypass with the inotropic support of dobutamine, and he was discharged from the hospital without any complications on the 10th postoperative day. At his 1-year follow-up, the patient was doing well and remained in NYHA functional class I–II.
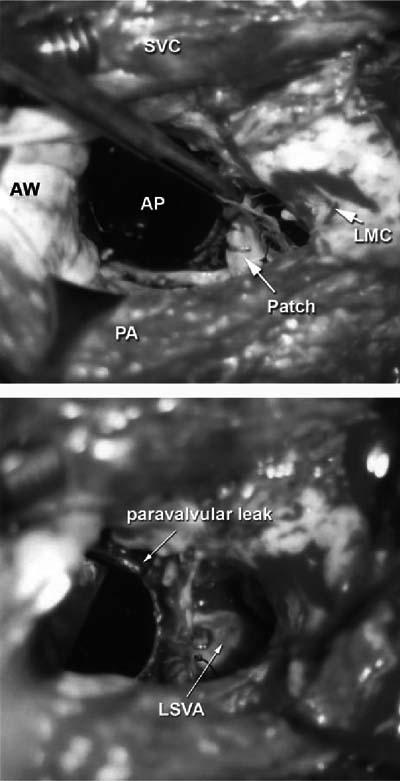
Fig. 2 The intraoperative photograph at top shows the detachment of the Dacron patch that had been placed over the mouth of the aneurysm of the left sinus of Valsalva. In addition, the cavity of the aneurysm that extends into the interventricular septum is seen in the photograph at bottom.
AP = aortic prosthesis; AW = aortic wall; LMC = orifice of left main coronary artery; LSVA = left sinus of Valsalva aneurysm; PA = pulmonary artery; SVC = superior vena cava
Discussion
The mechanism of the aneurysmal dilatation of the sinus of Valsalva is not completely understood. Acquired aneurysms of the sinus of Valsalva are usually caused by a weakness of the aortic media that is generally associated with trauma and endocarditis.7 Postoperative development of sinus of Valsalva aneurysm that dissects into the interventricular septum is extremely rare. It has a progressive course and a poor prognosis. This condition is usually associated with aortic valve insufficiency and annular dilatation. Its clinical manifestations are arrhythmia, AV block, obstruction of ventricular outflow tract, and heart failure, as we observed in our patient. Surgical management strategies involve plication, patch repair, and aortic root replacement, especially in the presence of aortic valve disease.
In the 1st operation associated with this present case (valve replacement), the left sinus of Valsalva aneurysm either was absent or was missed due to its small size. Four years later, the sudden development of complete atrioventricular block should have been interpreted as a 1st symptom of the dissection of the interventricular septum. In our 1st surgical correction of this unexpected aortic root abnormality,5 the aneurysmal cavity was not resected, nor was there an extra procedure for correction of the left ventricular outflow tract. We were therefore content with simple closure of the unruptured aneurysmal sac, as had been reported by others.1,4 Unfortunately, degenerative changes and the fragility of the tissues resulted, over time, in paravalvular leak and patch detachment. The onset and progression of the patient's symptoms were associated with structural deformity of the aortic root, which led to left ventricular dysfunction.
Preparation of a flanged composite graft has been described in detail.6 This modified Bentall procedure for aortic root replacement preserves the flexibility and elasticity of the aortic annulus, with no technical limitation.6 This method is an alternative to previously described Bentall procedures, especially when defects at the annular and subannular levels require repair.
We believe that—in the presence of aortic annulus deformity—resection of the aneurysmal sac and total aortic root replacement with this alternative technique is the appropriate procedure for surgical treatment of this extremely rare combination of pathologic conditions.
Footnotes
Address for reprints: Veysel Kutay, MD, YYU Arastirma Hastanesi, KVC Klinik, 65200 – Van, Turkey
E-mail: vkutay@yahoo.com
References
- 1.Bapat VN, Tendolkar AG, Khandeparkar J, Dalvi B, Agrawal N, Kulkarni H, Magotra R. Aneurysms of sinus of Valsalva eroding into the interventricular septum: etiopathology and surgical considerations. Eur J Cardiothorac Surg 1997;12:759–65. [DOI] [PubMed]
- 2.Wu Q, Xu J, Shen X, Wang D, Wang S. Surgical treatment of dissecting aneurysm of the interventricular septum. Eur J Cardiothorac Surg 2002;22:517–20. [DOI] [PubMed]
- 3.Takahara Y, Sudo Y, Sunazawa T, Nakajima N. Aneurysm of the left sinus of Valsalva producing aortic valve regurgitation and myocardial ischemia. Ann Thorac Surg 1998;65:535–7. [DOI] [PubMed]
- 4.Choudhary SK, Bhan A, Reddy SC, Sharma R, Murari V, Airan B, et al. Aneurysm of sinus of Valsalva dissecting into interventricular septum. Ann Thorac Surg 1998;65:735–40. [DOI] [PubMed]
- 5.Kutay V, Ekim H, Yakut C. Surgical repair of postoperative left sinus of Valsalva aneurysm dissecting into the interventricular septum. Ann Thorac Surg 2005;79:341–3. [DOI] [PubMed]
- 6.Yakut C. A new modified Bentall procedure: the flanged technique. Ann Thorac Surg 2001;71:2050–2. [DOI] [PubMed]
- 7.Goldberg N, Krasnow N. Sinus of Valsalva aneurysms. Clin Cardiol 1990;13:831–6. [DOI] [PubMed]