

Abstract
A 25-year-old, with type I Diabetes Mellitus with a previous diagnosis of Protamine Allergy but not to human Insulin, started to notice anaphylactic reactions inmmediatly after bolus with Insulin. Skin prick and intradermal test were positive to all insulins. Skin tests to other potential allergens resulted negative. Examination after bolus of Human Insulin revealed urticaria. Daily insulin requirement were around 2-2,4 U/Kg/day. Slow desensitisation with Aspart insulin, the insulin with lowest size of skin test, was performed using subcutaneous insulin pump. Six months after the end of desensitisation his daily insulin requirement decreased to 0.8 U/Kg/day and oral corticosteroids are being reduced with no symptoms.
Introduction
Drug hypersensitivity reactions by IgE-mediated mechanisms during therapies have been reported elsewhere. Diagnosis is based in a meticulous clinical history, but many times needs to be supported by skin and/or serological tests and, even sometimes, drug provocation tests since drug preparations may contain multiple potential allergens that can trigger reactions, including drug itself, carrier proteins [1] or additives [2]. Among drugs triggering allergy reactions, insulin allergy might be one of the hot and controversial topics, since it is usually the only known treatment in the case of patients suffering type I diabetes. Although the prevalence of suspected insulin allergy have been reported as high as 2.5% [3], diagnosis should be more accurate since less than one third of patients are finally diagnosed of true insulin allergy [4].
Case report
The patient is a 25-year-old builder with diabetes mellitus who was diagnosed at 23 years of age. Treatment with three daily injections of semi-synthetic human insulin was initially tolerated (Neutral protamine Hagedorn -NPH, Eli Lilly, Indianapolis, IN-: in the morning and in the evening and Lispro -Eli Lilly, Indianapolis, IN- in lunch-time). Glycosilated hemoglobin (HbA1c) controls were around 10%. He gradually started to develop wheals and flare local reactions following his injections of insulin. He was referred to Allergy Service of University Hospital NS Candelaria in April 2003. An initial exam at the Outpatient Clinic revealed strong sensitisation to Nickel Sulphate by patch test after 24, 48 and 96 hours. Separately, skin prick test (SPT) and intradermal test (ID) revealed sensitisation to Protamine (ID at 1:1000 dilution) but not to human insulin. Switch to Insulin without Protamine (Lispro -Eli Lilly, Indianapolis, IN) and subcutaneous insulin pump were both recommended. He did not observed any reaction for a 3-month period using Human regular insulin. Next, he started to notice local symptoms that progressively became worst. The symptoms included immediate episodes of wheals and flare reactions far from insertion site of the catheter, with intensive pruritus on palms and soles, and eventually dyspnea. Then, he developed similar symptoms 2–3 hours after bolus and occasionally some subcutaneos nodules.
Late 2004, he was hospitalised because ketoacidosis. Metil-prednisolone (15 mg/day) and hydroxicine were incorporated. Daily insulin requirement increased up to 2,4 U/Kg/day. He was reassessed at the Outpatient Clinic. SPT were positive to all insulins except Aspart (Novo Nordisk, Denmark). Serial ID showed positive test with Aspart at 1/100 dilution, Glargina (Aventis Pharma, Germany) at 1/100, zinc-crystalline insulin at 1/100, Lispro at 1/1,000 and Human regular insulin at 1/100.000. Skin tests to other potential allergens resulted negative. Specific IgE to protamine (0,43 kU/L), and bovine (2,5 kU/L), pork (3,9 kU/L) and human insulin (2,8 kU/L) were identified (negative: <0.35 kU/L; UniCAP, Pharmacia Diagnostics, Uppsala, Sweden). Controlled reexposure with a bolus of Regular Insulin revealed non-tender swelling with flares (5–6 cm of diameter) far from insertion of catheter without other symptoms. A biopsy specimen of the skin revealed subcutaneous edema with infiltrated cells, including eosinophils.
One month later, he was hospitalised because another cetoacydosis episode. As patient had the lowest grade of sensitisation to Aspart Insulin according to skin tests, and rapid insulin was needed, a desensitisation with Aspart insulin was proposed to him. Metil-prednidsolone 30 mg/day, but not hydroxicine, was maintained. Since his high requirement of insulin and risk of ketoacidosis, treatment with endovenous regular insulin was continued up to achieve enough dose of Aspart insulin to sustain him. After written and oral inform consent, desensitisation using subcutaneous insulin pump [5] was performed in 16 sessions (6–7 doses per day). It was started with 0.001 U and increased 2-fold with intervals of 15–30 min, repeating dose in the case of reaction (Table I). During first consecutive 7 sessions patient suffered flare reactions that were cleared up in few minutes without treatment (figure 1, 2 and 3). During all process ketonemia did not show significant changes and serum tryptase levels were normal, although serum histamine did increase 2-fold. Finally enough basal rate was maintained and "square bolus" up to 20 U could be applied without reactions. Six months after the end of desensitisation his daily insulin requirement decreased to 0.8 U/Kg/day and oral corticosteroids are being reduced (metilprednisolone 2 mg/48 h).
Table 1.
Schedule of desensitization protocol by subcutaneous insulin pump with Aspart Insulin
| DAY | DOSE | Reaction/n° PULSES | TIME BETWEEN DOSES (min) |
| 1 | 0,001 | NO/1 | 15 |
| 1 | 0,005 | NO/1 | 15 |
| 1/2 | 0,01 | YES/4 | 15 |
| 1/2 | 0,02 | YES/2 | 15 |
| 2/3 | 0,05 | YES/2 | 15 |
| 2/3/4 | 0,1 | YES/5 | 15 |
| 3/4/5 | 0,2 | YES/6 | 15 |
| 3/4/5/6 | 0,4 | YES/5 | 15 |
| 6/7 | 0,6 | YES/4 | 15 |
| 6/7/8 | 0,8 | YES/4 | 15 |
| 7/8/9 | 1 | YES/3 | 30 |
| 8/9 | 1,4 | YES/4 | 30 |
| 9/10 | 1,8 | NO/4 | 30 |
| 9/10 | 2,5 | NO/4 | 30 |
| 10/11 | 3 | NO/4 | 30 |
| 11/12 | 3,5 | NO/4 | 30 |
| 12/13 | 4 | NO/4 | 30 |
| 13/14 | 7 | NO/4 | 30 |
| 14/15 | 10 | NO/4 | 30 |
| 15/16 | 15 | NO/4 | 30 |
| 16 | 20 | NO/4 | 30 |
Figure 1.

Skin Reaction patient in day #1.
Figure 2.

Skin Reaction patient in day #2.
Figure 3.

Skin Reaction patient in day #3.
Discussion
Multiples cases of allergy to insulin components have been described and reported [6] since it is the treatment for type I diabetic patients. Currently, the prevalence of reactions during insulin treatment seems to be around 2% [3], but less than one third of reported events have been considered related to insulin therapy [4]. Other multiples causes include protamine [7-9], latex[10], cresol, zinc, etc. IgE-mediated reactions have been reported with animal [11] and human insulin [12-15] including semisynthetic and biosynthetic insulins [5,16-21].
Many algorithms of insulin allergy diagnosis have been published although diagnosis is merely based in compatible clinical history and skin test [4] since many diabetic patients can have positive skin test and serum antibodies without clinical symptoms. Switch to insulin analogs has markedly decreased the number of allergic episodes [22-27], since allergenicity of insulin have been proposed by chemical changes in the terminal of B chain [18], where insulin analogs have the modified structure. For instance, Lispro is insulin with lysine and proline in positions 28 and 29, respectively, of beta chain, instead of proline and lysine as in human insulin. Aspart has aspartate in position 28 of beta chain instead of proline (figure 4). Glargine is insulin with arginine and proline in positions 28 and 29 respectively. However, these analogs have also ability to induce allergic episodes[5,16-21,28] and reduced immunogenicity has been more associated to its faster absorption than any changes in the immunogenic epitopes[25].
Figure 4.
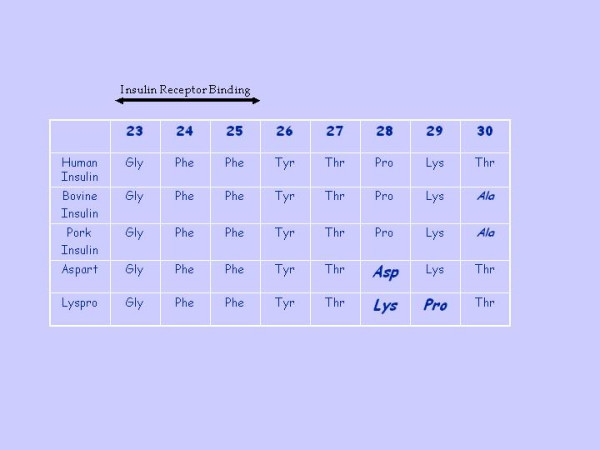
Terminal side of β chain (from aminoacid 23 to 30), including Insulin Receptor Binding (from aminoacid 23 to 25) of different insulins.
In this case, insulin pump [5,29] and slow desensitization protocol[30] have demonstrated usefulness to tolerate insulinen and has also helped to reduce insulin requirement as other authors have seen [31]. Although using insulin pump alone have been associated to decrease in insulin dosage [5], our patient was previously using insulin pump with high doses of required insulin. Thus, we could speculate that desensitisation have created a decrease of insulin requirement.
In the near future, anti-immunoglobulin E treatment with omalizumab will probably give another alternative to these patients before transplantation [32]
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
VM designed Allergy study, was responsible for desensitisation protocol and drafted the manuscript, EP & JC-G performed all skin tests and made the final diagnosis of Insulin allergy, MH has been responsible for patient follow up from the beginning and remitted him to our Allergy Unit, ED & IS performed desensitisation, RD & AG controlled patient's diabetes during hospital stay, LF made skin biopsy, AC controlled patient in Intensive Care Unit every day after desensitisation session and was responsible for coordination trough Medical Transport Ambulance Service between hospitals, FT made first diagnosis of niquel and protamine allergy.
Contributor Information
Victor Matheu, Email: victor.matheu@med.lu.se.
Eva Perez, Email: evaprod@hotmail.com.
Marta Hernández, Email: mhgarcia@huc.es.
Elisa Díaz, Email: evaprod@hotmail.com.
Ricardo Darias, Email: evaprod@hotmail.com.
Abel González, Email: zerupean@hotmail.com.
Jose C García, Email: jgarcia@seaic.es.
Inmaculada Sánchez, Email: zerupean@vodafone.es.
Laura Feliciano, Email: evaprod@hotmail.com.
Agueda Caballero, Email: mhgarcia@huc.es.
Fernando de la Torre, Email: ftormor@gobiernodecanarias.org.
References
- Matheu V, Caloto M, de Barrio M, Baeza ML, Rubio M. Life-threatening anaphylaxis after artificial insemination. Lancet. 2002;359:1779. doi: 10.1016/S0140-6736(02)08627-0. [DOI] [PubMed] [Google Scholar]
- Matheu V, Zapatero L, Alcazar M, Martinez-Molero MI, Baeza ML. IgE-mediated reaction to a banana-flavored drug additive. J Allergy Clin Immunol. 2000;106:1202–1203. doi: 10.1067/mai.2000.111239. [DOI] [PubMed] [Google Scholar]
- Fineberg SE, Huang J, Brunelle R, Gulliya KS, Anderson JHJ. Effect of long-term exposure to insulin lispro on the induction of antibody response in patients with type 1 or type 2 diabetes. Diabetes Care. 2003;26:89–96. doi: 10.2337/diacare.26.1.89. [DOI] [PubMed] [Google Scholar]
- Bodtger U, Wittrup M. A rational clinical approach to suspected insulin allergy: status after five years and 22 cases. Diabet Med. 2005;22:102–106. doi: 10.1111/j.1464-5491.2004.01352.x. [DOI] [PubMed] [Google Scholar]
- Eapen SS, Connor EL, Gern JE. Insulin desensitization with insulin lispro and an insulin pump in a 5-year-old child. Ann Allergy Asthma Immunol. 2000;85:395–397. doi: 10.1016/S1081-1206(10)62554-9. [DOI] [PubMed] [Google Scholar]
- Aiken JB. Allergy to Insulin. Can Med Assoc J. 1964;90:660–662. [PMC free article] [PubMed] [Google Scholar]
- Blanco C, Castillo R, Quiralte J, Delgado J, Garcia I, de Pablos P, Carrillo T. Anaphylaxis to subcutaneous neutral protamine Hagedorn insulin with simultaneous sensitization to protamine and insulin. Allergy. 1996;51:421–424. [PubMed] [Google Scholar]
- Kim R. Anaphylaxis to protamine masquerading as an insulin allergy. Del Med J. 1993;65:17–23. [PubMed] [Google Scholar]
- Bollinger ME, Hamilton RG, Wood RA. Protamine allergy as a complication of insulin hypersensitivity: A case report. J Allergy Clin Immunol. 1999;104:462–465. doi: 10.1016/S0091-6749(99)70394-5. [DOI] [PubMed] [Google Scholar]
- Roest MA, Shaw S, Orton DI. Insulin-injection-site reactions associated with type I latex allergy. N Engl J Med. 2003;348:265–266. doi: 10.1056/NEJM200301163480320. [DOI] [PubMed] [Google Scholar]
- Schernthaner G. Immunogenicity and allergenic potential of animal and human insulins. Diabetes Care. 1993;16 Suppl 3:155–165. doi: 10.2337/diacare.16.3.155. [DOI] [PubMed] [Google Scholar]
- Garcia-Ortega MP. [Allergy to insulin] Med Clin (Barc) 1985;84:535–537. [PubMed] [Google Scholar]
- Rau NR, Prakash PS, Sudha V, Nagaraj MV. Insulin allergy. J Assoc Physicians India. 1991;39:721–722. [PubMed] [Google Scholar]
- Zubeldia JM, Arrieta FJ, Saavedra MP, de las Heras M, Sastre A, Herrera Pombo JL. [Allergy to human insulin, clinical and immunologic aspects and therapeutic approach: apropos of a case] Rev Clin Esp. 1988;183:193–196. [PubMed] [Google Scholar]
- Goldfine AB, Kahn CR. Insulin allergy and insulin resistance. Curr Ther Endocrinol Metab. 1994;5:461–464. [PubMed] [Google Scholar]
- Gonzalo MA, De Argila D, Revenga F, Garcia JM, Diaz J, Morales F. Cutaneous allergy to human (recombinant DNA) insulin. Allergy. 1998;53:106–107. doi: 10.1111/j.1398-9995.1998.tb03786.x. [DOI] [PubMed] [Google Scholar]
- Rosas Vargas MA, Alvarez Amador M, Alvarez Amador LM, del Rio Navarro BE, Avila Castanon L, Sienra Monge JJ. [Desensitization to human recombinant DNA insulin in an adolescent with insulin-dependent diabetes mellitus] Rev Alerg Mex. 2001;48:129–132. [PubMed] [Google Scholar]
- Yokoyama H, Fukumoto S, Koyama H, Emoto M, Kitagawa Y, Nishizawa Y. Insulin allergy; desensitization with crystalline zinc-insulin and steroid tapering. Diabetes Res Clin Pract. 2003;61:161–166. doi: 10.1016/S0168-8227(03)00114-1. [DOI] [PubMed] [Google Scholar]
- Barranco R, Herrero T, Tornero P, Barrio M, Frutos C, Rodriguez A, Malvetti V, Luisa Baeza M. Systemic allergic reaction by a human insulin analog. Allergy. 2003;58:536–537. doi: 10.1034/j.1398-9995.2003.00143.x. [DOI] [PubMed] [Google Scholar]
- Durand-Gonzalez KN, Guillausseau N, Pecquet C, Gayno JP. Glargine insulin is not an alternative in insulin allergy. Diabetes Care. 2003;26:2216. doi: 10.2337/diacare.26.7.2216. [DOI] [PubMed] [Google Scholar]
- Fernandez L, Duque S, Montalban C, Bartolome B. Allergy to human insulin. Allergy. 2003;58:1317. doi: 10.1046/j.1398-9995.2003.00324.x. [DOI] [PubMed] [Google Scholar]
- Abraham MR, al-Sharafi BA, Saavedra GA, Khardori R. Lispro in the treatment of insulin allergy. Diabetes Care. 1999;22:1916–1917. doi: 10.2337/diacare.22.11.1916. [DOI] [PubMed] [Google Scholar]
- Kumar D. Lispro analog for treatment of generalized allergy to human insulin. Diabetes Care. 1997;20:1357–1359. doi: 10.2337/diacare.20.9.1357. [DOI] [PubMed] [Google Scholar]
- Lluch-Bernal M, Fernandez M, Herrera-Pombo JL, Sastre J. Insulin lispro, an alternative in insulin hypersensitivity. Allergy. 1999;54:186–187. doi: 10.1034/j.1398-9995.1999.00988.x. [DOI] [PubMed] [Google Scholar]
- Panczel P, Hosszufalusi N, Horvath MM, Horvath A. Advantage of insulin lispro in suspected insulin allergy. Allergy. 2000;55:409–410. doi: 10.1034/j.1398-9995.2000.00565.x. [DOI] [PubMed] [Google Scholar]
- Yasuda H, Nagata M, Moriyama H, Fujihira K, Kotani R, Yamada K, Ueda H, Yokono K. Human insulin analog insulin aspart does not cause insulin allergy. Diabetes Care. 2001;24:2008–2009. doi: 10.2337/diacare.24.11.2008. [DOI] [PubMed] [Google Scholar]
- Kara C, Kutlu AO, Evliyaoglu O, Bilgili H, Yildirim N. Successful treatment of insulin allergy in a 1-year-old infant with neonatal diabetes by lispro and glargine insulin. Diabetes Care. 2005;28:983–984. doi: 10.2337/diacare.28.4.983. [DOI] [PubMed] [Google Scholar]
- JiXiong X, Jianying L, Yulan C, Huixian C. The human insulin analog aspart can induce insulin allergy. Diabetes Care. 2004;27:2084–2085. doi: 10.2337/diacare.27.8.2084-a. [DOI] [PubMed] [Google Scholar]
- Naf S, Esmatjes E, Recasens M, Valero A, Halperin I, Levy I, Gomis R. Continuous subcutaneous insulin infusion to resolve an allergy to human insulin. Diabetes Care. 2002;25:634–635. doi: 10.2337/diacare.25.3.634-a. [DOI] [PubMed] [Google Scholar]
- Thompson DM, Ronco JJ. Prolonged desensitization required for treatment of generalized allergy to human insulin. Diabetes Care. 1993;16:957–958. doi: 10.2337/diacare.16.6.957. [DOI] [PubMed] [Google Scholar]
- Lahtela JT, Knip M, Paul R, Antonen J, Salmi J. Severe antibody-mediated human insulin resistance: successful treatment with the insulin analog lispro. Diabetes Care. 1997;20:71–73. doi: 10.2337/diacare.20.1.71. [DOI] [PubMed] [Google Scholar]
- Oh HK, Provenzano R, Hendrix J, el-Nachef MW. Insulin allergy resolution following pancreas transplantation alone. Clin Transplant. 1998;12:593–595. [PubMed] [Google Scholar]