

Abstract
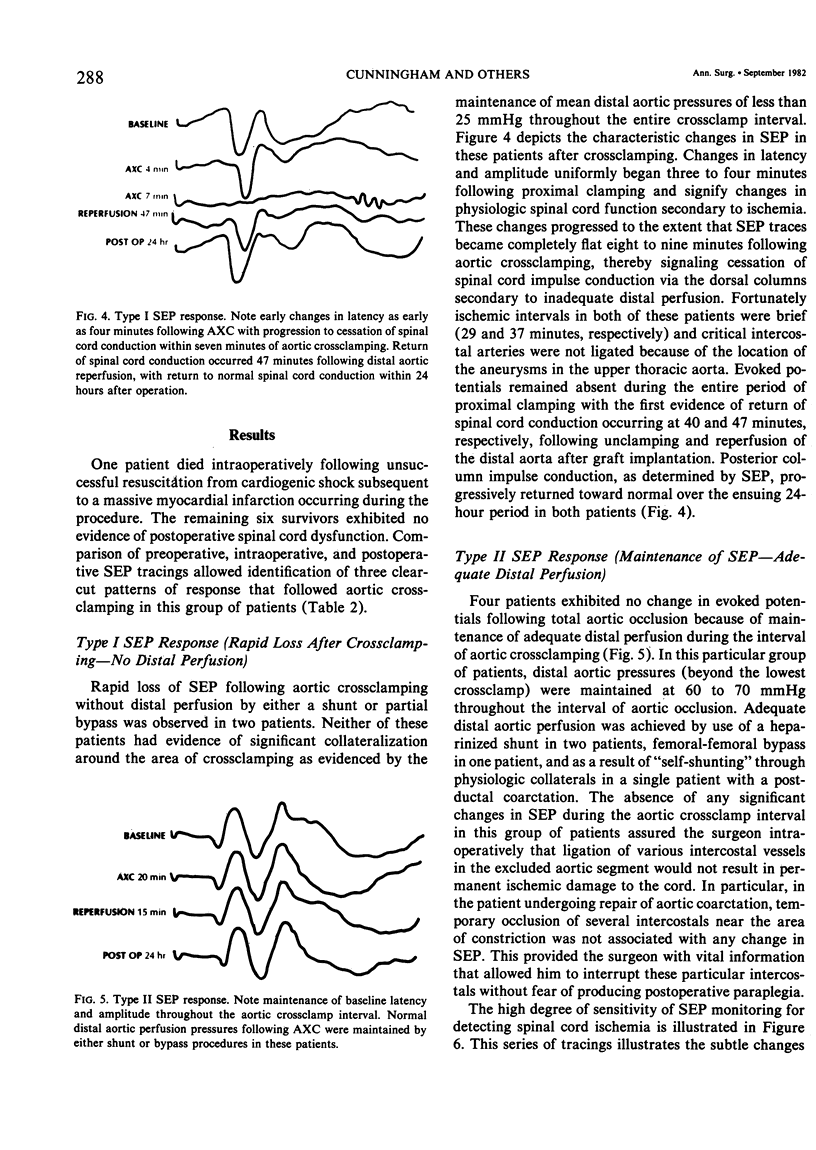
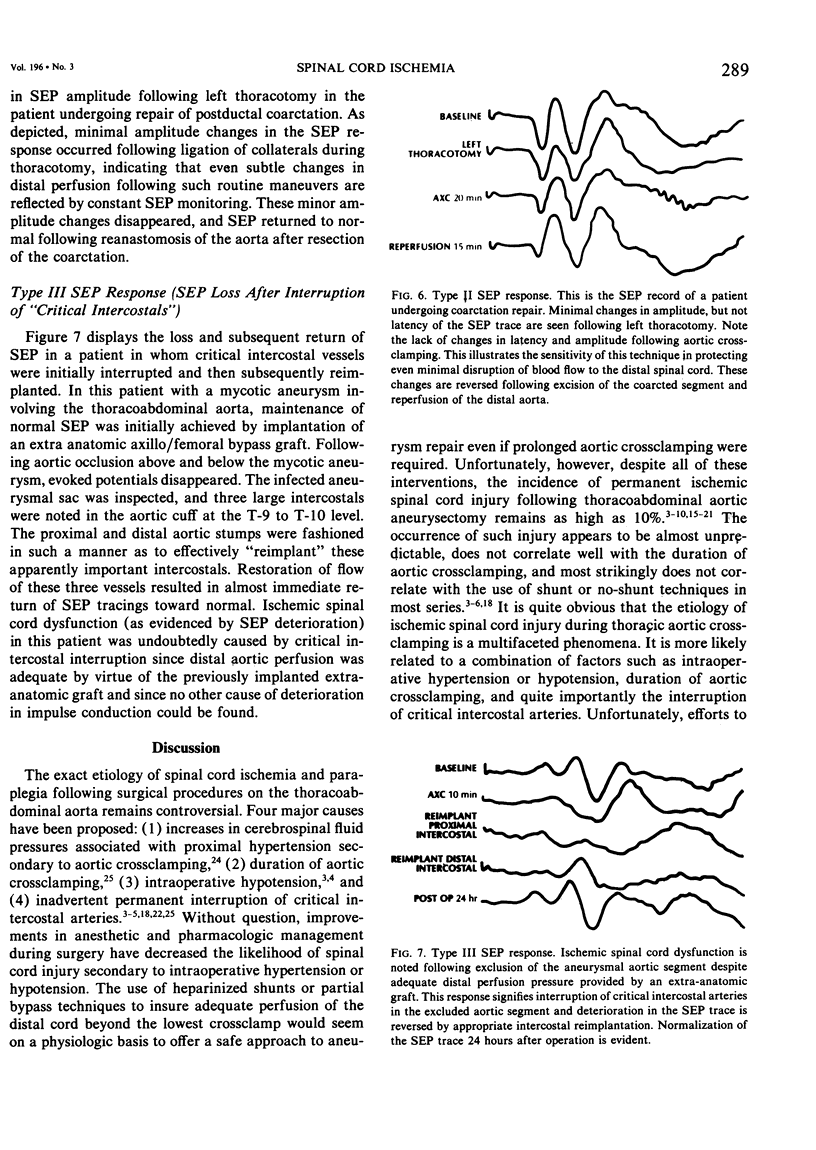
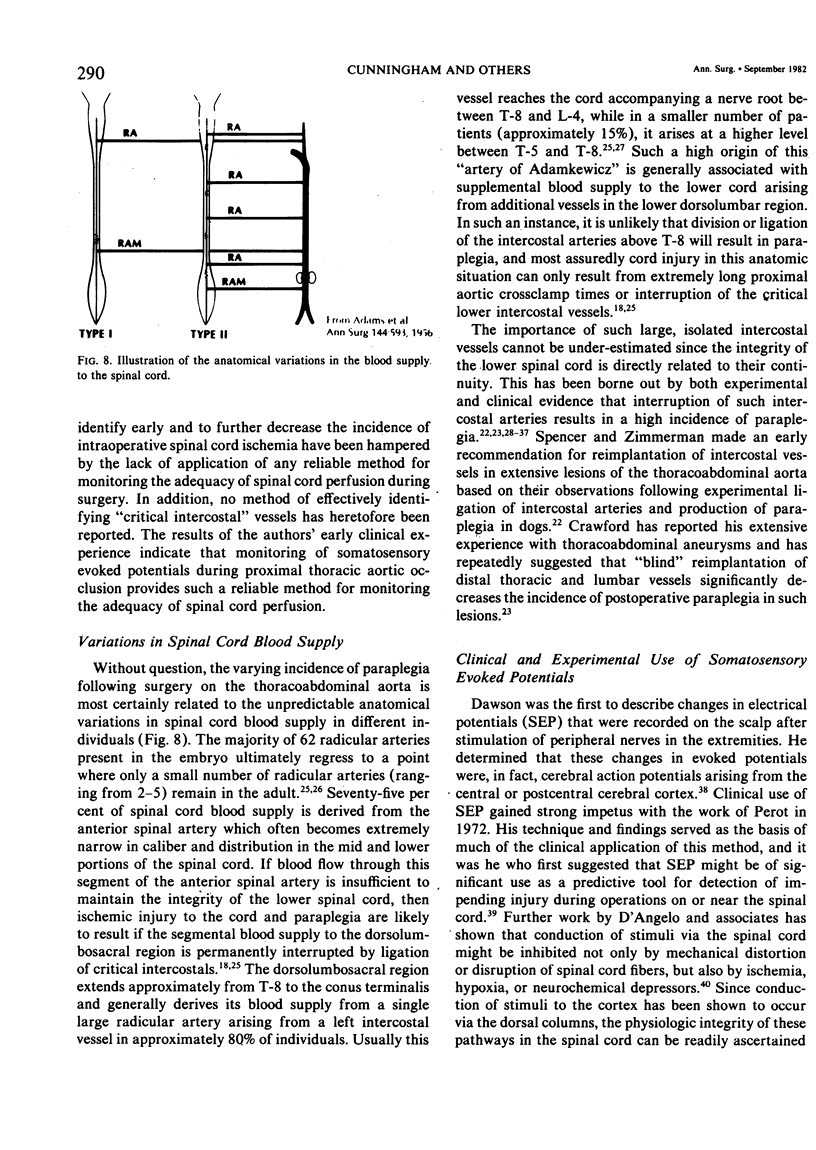
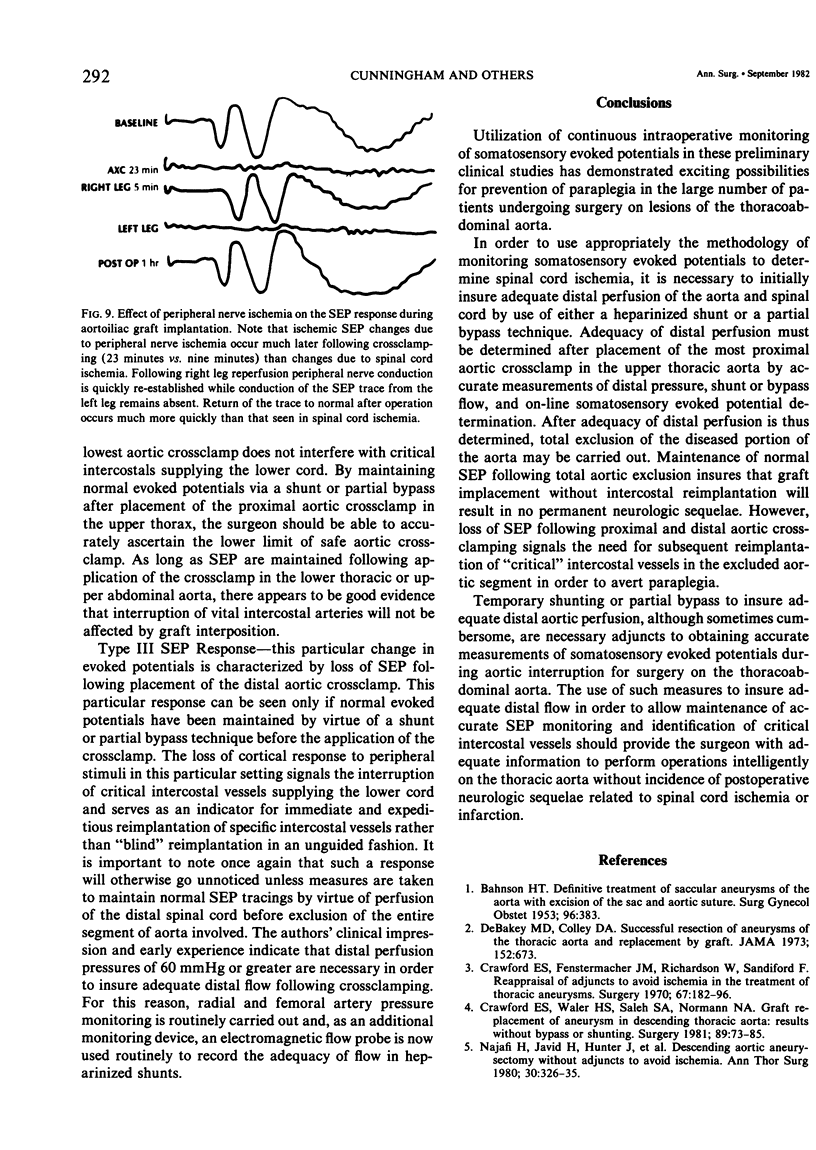
Paraplegia has been an unpredictable, devasting complication following operations upon the thoracoabdominal aorta for over 30 years. The frequency ranges from 0.5% with operations for coarctation to as high as 15% following surgery for thoracoabdominal aneurysms. Both uncertainty and controversy exist about the value of different protective methods during aortic crossclamping (AXC): heparinized shunts, partial bypass, and reimplantation of intercostal arteries. This report describes the authors' initial clinical experience with a highly sensitive indicator of spinal cord ischemia, somatosensory evoked potentials (SEP) in an attempt to prevent paraplegia associated with surgical procedures on the thoracoabdominal aorta. Seven consecutive patients (one coarctation, five thoracic aneurysms, one thoracoabdominal aneurysm) underwent continuous operative monitoring of SEP. Cortical response to simultaneous electrical stimulation (20 mAmps, 0.6 mSec., 2.3 cps) of both the right and left posterior tibial nerves was recorded before, during, and after AXC, and following operation. When ischemic changes were detected by SEP, increasing distal circulation by different maneuvers (heparinized shunt, femoral-femoral bypass, reimplantation of intercostal arteries) reversed these changes. In two patients with thoracic aneurysms, ischemic changes appeared within three minutes after AXC and all potentials disappeared in nine minutes. Rapid insertion of a graft (AXC 28 and 37 minutes) resulted in SEP return 40 minutes following restoration of flow. These changes were prevented by a heparinized shunt in two patients, femoral/femoral bypass in one, and T8-T9 intercostal reimplantation in one. No SEP changes occurred in the patient with coarctation. No postoperative neurologic complications occurred. Continuous operative monitoring of SEP has exciting possibilities for preventing paraplegia. It is simple, highly sensitive, and seems to provide a precise measurement of adequacy of circulation to the spinal cord.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
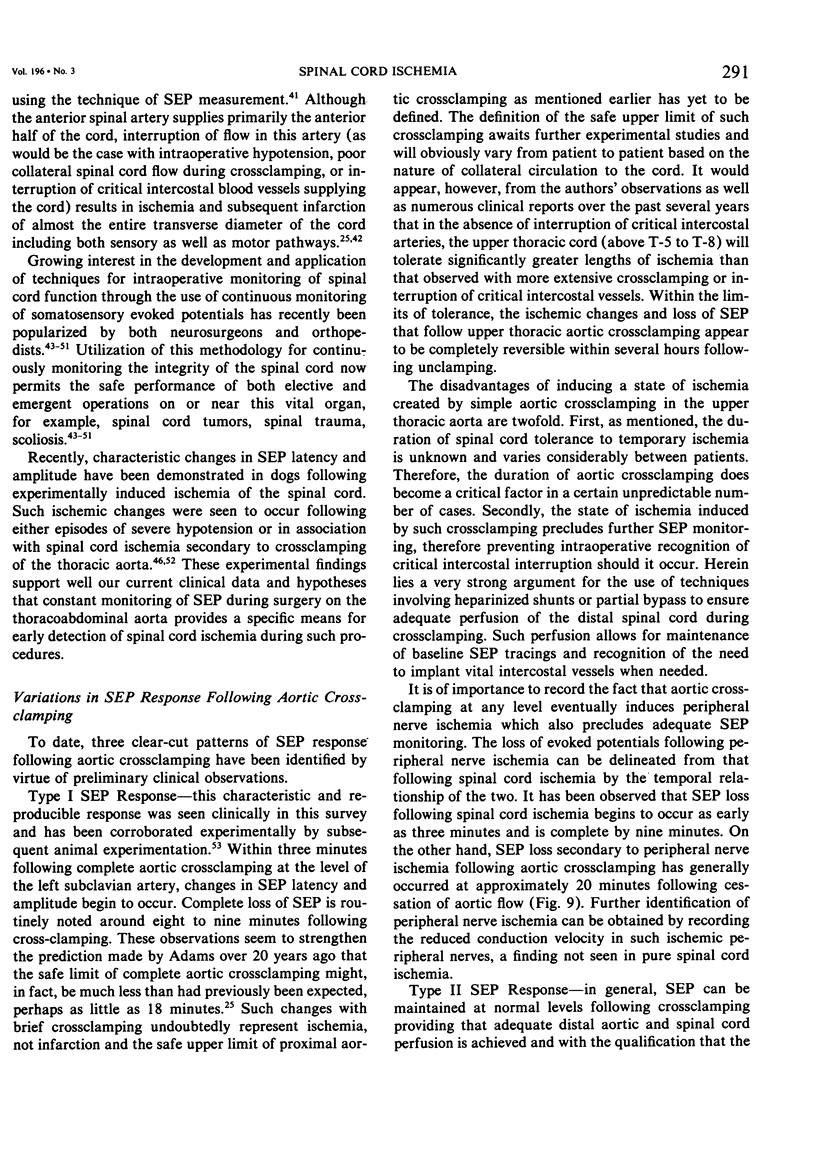
- ADAMS H. D., VAN GEERTRUYDEN H. H. Neurologic complications of aortic surgery. Ann Surg. 1956 Oct;144(4):574–610. doi: 10.1097/00000658-195610000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BAHNSON H. T. Definitive treatment of saccular aneurysms of the aorta with excision of sac and aortic suture. Surg Gynecol Obstet. 1953 Apr;96(4):383–402. [PubMed] [Google Scholar]
- BLAISDELL F. W., COOLEY D. A. The mechanism of paraplegia after temporary thoracic aortic occlusion and its relationship to spinal fluid pressure. Surgery. 1962 Mar;51:351–355. [PubMed] [Google Scholar]
- Cohen A. R., Young W., Ransohoff J. Intraspinal localization of the somatosensory evoked potential. Neurosurgery. 1981 Aug;9(2):157–162. doi: 10.1227/00006123-198108000-00008. [DOI] [PubMed] [Google Scholar]
- Connolly J. E., Wakabayashi A., German J. C., Stemmer E. A., Serres E. J. Clinical experience with pulsatile left heart bypass without anticoagulation for thoracic aneurysms. J Thorac Cardiovasc Surg. 1971 Oct;62(4):568–576. [PubMed] [Google Scholar]
- Connors J. P., Ferguson T. B., Roper C. L., Weldon C. S. The use of the TDMAC-heparin shunt in replacement of the descending thoracic aorta. Ann Surg. 1975 May;181(5):735–741. doi: 10.1097/00000658-197505000-00031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crawford E. S., Fenstermacher J. M., Richardson W., Sandiford F. Reappraisal of adjuncts to avoid ischemia in the treatment of thoracic aortic aneurysms. Surgery. 1970 Jan;67(1):182–196. [PubMed] [Google Scholar]
- Crawford E. S., Snyder D. M., Cho G. C., Roehm J. O., Jr Progress in treatment of thoracoabdominal and abdominal aortic aneurysms involving celiac, superior mesenteric, and renal arteries. Ann Surg. 1978 Sep;188(3):404–422. doi: 10.1097/00000658-197809000-00016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crawford E. S., Walker H. S., 3rd, Saleh S. A., Normann N. A. Graft replacement of aneurysm in descending thoracic aorta: results without bypass or shunting. Surgery. 1981 Jan;89(1):73–85. [PubMed] [Google Scholar]
- Croft T. J., Brodkey J. S., Nulsen F. E. Reversible spinal cord trauma: a model for electrical monitoring of spinal cord function. J Neurosurg. 1972 Apr;36(4):402–406. doi: 10.3171/jns.1972.36.4.0402. [DOI] [PubMed] [Google Scholar]
- Cukingnan R. A., Fee H. J., Carey J. S. Repair of lesions of the descending thoracic aorta with the TDMAC-heparin shunt. J Thorac Cardiovasc Surg. 1978 Feb;75(2):227–231. [PubMed] [Google Scholar]
- D'Angelo C. M., Van Gilder J. C., Taub A. Evoked cortical potentials in experimental spinal cord trauma. J Neurosurg. 1973 Mar;38(3):332–336. doi: 10.3171/jns.1973.38.3.0332. [DOI] [PubMed] [Google Scholar]
- DeMeester T. R., Cameron J. L., Gott V. L. Repair of a through-and-through gunshot wound of the aortic arch using a heparinized shunt. Ann Thorac Surg. 1973 Aug;16(2):193–198. doi: 10.1016/s0003-4975(10)65836-5. [DOI] [PubMed] [Google Scholar]
- Donahoo J. S., Brawley R. K., Gott V. L. The heparin-coated vascular shunt for thoracic aortic and great vessel procedures: a ten-year experience. Ann Thorac Surg. 1977 Jun;23(6):507–513. doi: 10.1016/s0003-4975(10)63692-2. [DOI] [PubMed] [Google Scholar]
- Engler G. L., Spielholz N. J., Bernhard W. N., Danziger F., Merkin H., Wolff T. Somatosensory evoked potentials during Harrington instrumentation for scoliosis. J Bone Joint Surg Am. 1978 Jun;60(4):528–532. [PubMed] [Google Scholar]
- Frantz P. T., Murray G. F., Shallal J. A., Lucas C. L. Clinical and experimental evaluation of left ventriculoiliac shunt bypass during repair of lesions of the descending thoracic aorta. Ann Thorac Surg. 1981 Jun;31(6):551–557. doi: 10.1016/s0003-4975(10)61348-3. [DOI] [PubMed] [Google Scholar]
- Fried L. C., Aparicio O. Experimental ischemia of the spinal cord. Histologic studies after anterior spinal artery occlusion. Neurology. 1973 Mar;23(3):289–293. doi: 10.1212/wnl.23.3.289. [DOI] [PubMed] [Google Scholar]
- Fried L. C., Di Chiro G., Doppman J. L. Ligation of major thoraco-lumbar spinal cord arteries in monkeys. J Neurosurg. 1969 Dec;31(6):608–614. doi: 10.3171/jns.1969.31.6.0608. [DOI] [PubMed] [Google Scholar]
- HILL C. S., Jr, VASQUEZ J. M. Massive infarction of spinal cord and vertebral boides as a complication of dissecting aneurysm of the aorta. Circulation. 1962 Jun;25:997–1000. doi: 10.1161/01.cir.25.6.997. [DOI] [PubMed] [Google Scholar]
- Hilgenberg A. D., Rainer W. G., Sadler T. R., Jr Aneurysm of the descending thoracic aorta: replacement with the use of a shunt or bypass. J Thorac Cardiovasc Surg. 1981 Jun;81(6):818–824. [PubMed] [Google Scholar]
- Kouchoukos N. T., Lell W. A., Karp R. B., Samuelson P. N. Hemodynamic effects of aortic clamping and decompression with a temporary shunt for resection of the descending thoracic aorta. Surgery. 1979 Jan;85(1):25–30. [PubMed] [Google Scholar]
- Lawrence G. H., Hessel E. A., Sauvage L. R., Krause A. H. Results of the use of the TDMAC-heparin shung in the surgery of aneurysms of the descending thoracic aorta. J Thorac Cardiovasc Surg. 1977 Mar;73(3):393–398. [PubMed] [Google Scholar]
- MOERSCH F. P., SAYRE G. P. Neurologic manifestations associated with dissecting aneurysm of the aorta. J Am Med Assoc. 1950 Dec 2;144(14):1141–1148. doi: 10.1001/jama.1950.02920140001001. [DOI] [PubMed] [Google Scholar]
- May I. A., Ecker R. R., Iverson L. I. Heparinless femoral venoarterial bypass without an oxygenator for surgery on the descending thoracic aorta. J Thorac Cardiovasc Surg. 1977 Mar;73(3):387–392. [PubMed] [Google Scholar]
- Najafi H., Javid H., Hunter J., Serry C., Monson D. Descending aortic aneurysmectomy without adjuncts to avoid ischemia. Ann Thorac Surg. 1980 Oct;30(4):326–335. doi: 10.1016/s0003-4975(10)61269-6. [DOI] [PubMed] [Google Scholar]
- Nash C. L., Jr, Lorig R. A., Schatzinger L. A., Brown R. H. Spinal cord monitoring during operative treatment of the spine. Clin Orthop Relat Res. 1977 Jul-Aug;(126):100–105. [PubMed] [Google Scholar]
- Perot P. L., Jr Chapter 28. The clinical use of somatosensory evoked potentials in spinal cord injury. Clin Neurosurg. 1973;20:367–381. doi: 10.1093/neurosurgery/20.cn_suppl_1.367. [DOI] [PubMed] [Google Scholar]
- Reul G. J., Cooley D. A., Hallman G. L., Reddy S. B., Kyger E. R., 3rd, Wukasch D. C. Dissecting aneurysm of the descending aorta. Improved surgical results in 91 patients. Arch Surg. 1975 May;110(5):632–640. doi: 10.1001/archsurg.1975.01360110178030. [DOI] [PubMed] [Google Scholar]
- SCHWARZ G. A., SHOREY W. K., ANDERSON N. S. Myelomalacia secondary to dissecting aneurysm of the aorta. Arch Neurol Psychiatry. 1950 Sep;64(3):401–416. doi: 10.1001/archneurpsyc.1950.02310270090005. [DOI] [PubMed] [Google Scholar]
- SCOTT R. W., SANCETTA S. M. Dissecting aneurysm of aorta with hemorrhagic infarction of the spinal cord and complete paraplegia. Am Heart J. 1949 Nov;38(5):747-57, illust. doi: 10.1016/0002-8703(49)90531-1. [DOI] [PubMed] [Google Scholar]
- SPENCER F. C., ZIMMERMAN J. M. The influence of ligation of intercostal arteries on paraplegia in dogs. Surg Forum. 1958;9:340–342. [PubMed] [Google Scholar]
- Spielholz N. I., Benjamin M. V., Engler G. L., Ransohoff J. Somatosensory evoked potentials during decompression and stabilization of the spine. Methods and findings. Spine (Phila Pa 1976) 1979 Nov-Dec;4(6):500–505. doi: 10.1097/00007632-197911000-00008. [DOI] [PubMed] [Google Scholar]
- THOMPSON G. B. Dissecting aortic aneurysm with infarction of the spinal cord. Brain. 1956 Mar;79(1):111–118. doi: 10.1093/brain/79.1.111. [DOI] [PubMed] [Google Scholar]
- Wakabayashi A., Connolly J. E. Prevention of paraplegia associated with resection of extensive thoracic aneurysms. Arch Surg. 1976 Nov;111(11):1186–1189. doi: 10.1001/archsurg.1976.01360290020003. [DOI] [PubMed] [Google Scholar]
- Wakabayashi A., Connolly J. E., Stemmer E. A., Nakamura Y., Kubo T., Ino T. Heparinless left heart bypass for resection of thoracic aortic aneurysms. Am J Surg. 1975 Aug;130(2):212–218. doi: 10.1016/0002-9610(75)90373-6. [DOI] [PubMed] [Google Scholar]
- de Bakey M. E., McCollum C. H., Graham J. M. Surgical treatment of aneurysms of the descending thoracic aorta: long-term results in 500 patients. J Cardiovasc Surg (Torino) 1978 Nov-Dec;19(6):571–576. [PubMed] [Google Scholar]