

Abstract
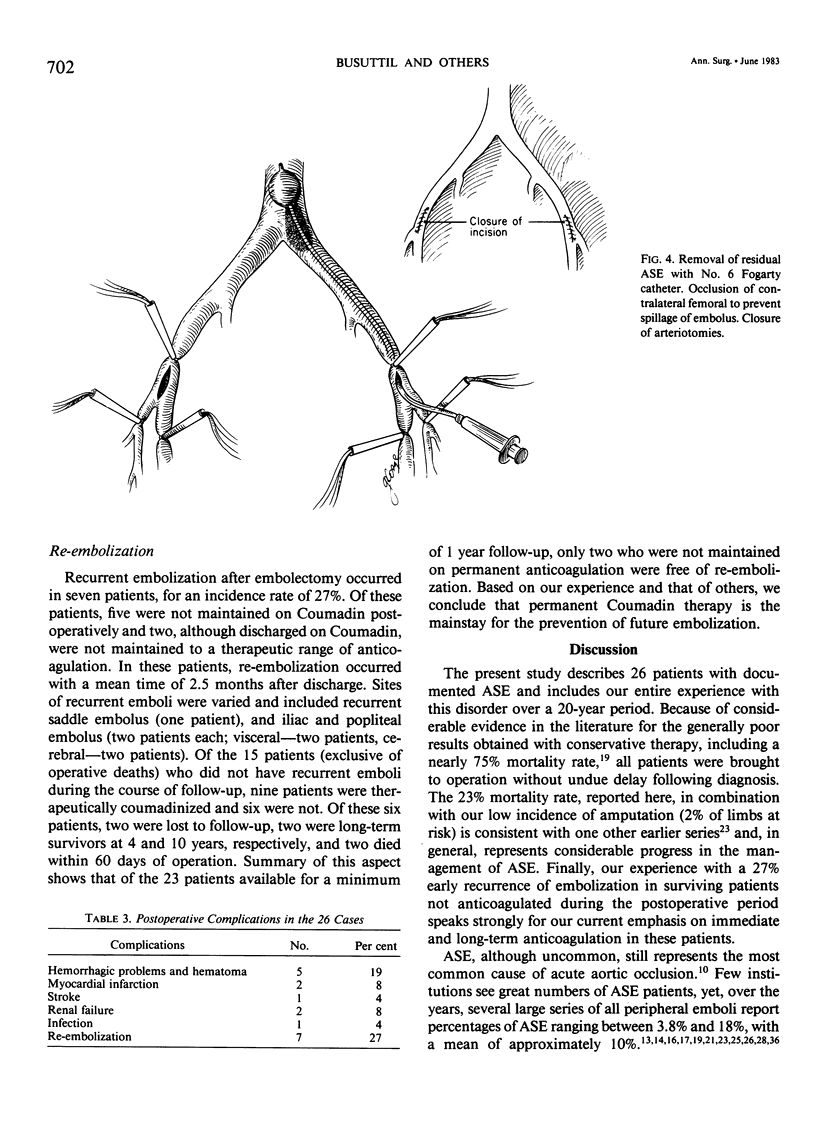
Clinical experience with aortic saddle embolus (ASE) is not extensive due to the relative infrequent lodging of emboli at the aortic bifurcation. During the period 1962-1982, 26 patients (mean age, 56 years) were treated at the UCLA Medical Center for ASE and followed from 2 to 158 months (mean, 45 months). These cases were reviewed in order to identify features of diagnosis, anticoagulation, and operation which impact on results. All 26 patients presented with bilateral lower extremity ischemia with or without extension of clot to the iliac bifurcation. Ninety-six per cent of emboli were of cardiac origin and one-third occurred in patients who had previous symptoms of chronic lower extremity ischemia. Rest pain and motor/sensory deficits were main complaints in 92% of the patients, but did not become manifest until more than 6 hours, unlike more distal emboli which have an earlier presentation. Preoperative angiography, even in the patient with a history of claudication, has a small role in planning the surgical approach to patients with ASE and, although performed in 11 patients, it influenced operation in only two. Operation within the "golden period" of 6 hours after embolization did not significantly influence outcome after ASE, since 20 patients were operated on more than 6 hours after embolization, with results similar to six patients who were operated on less than 6 hours after embolization. Early high-dose heparinization, used in all patients and maintained for a mean of 12 days, may have contributed to this effect. In 22 patients (85%) Forgarty catheter extraction via bilateral groin approaches was used with a mortality of 14%; only one death was directly attributed to the catheter embolectomy. In 15% of patients, a direct approach on the aorta was selected with a zero mortality rate. Postoperative functional result was excellent with an amputation rate of only 2% (one limb). Re-embolization occurred in seven patients (27%) after discharge, five of whom had not been maintained on Coumadin and two who were not anticoagulated adequately. The authors conclude that the keys to successful treatment of ASE include high dose heparin which is maintained through the perioperative period, embolectomy without preoperative angiography, and maintenance of long-term oral anticoagulation.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ALBRIGHT H. L., LEONARD F. C. Embolectomy from the abdominal aorta. N Engl J Med. 1950 Feb 23;242(8):271–277. doi: 10.1056/NEJM195002232420801. [DOI] [PubMed] [Google Scholar]
- Barker C. F., Rosato F. E., Roberts B. Peripheral arterial embolism. Surg Gynecol Obstet. 1966 Jul;123(1):22–26. [PubMed] [Google Scholar]
- Blaisdell F. W., Steele M., Allen R. E. Management of acute lower extremity arterial ischemia due to embolism and thrombosis. Surgery. 1978 Dec;84(6):822–834. [PubMed] [Google Scholar]
- CRANLEY J. J., KRAUSE R. J., STRASSER E. S., HAFNER C. D., FOGARTY T. J. PERIPHERAL ARTERIAL EMBOLISM: CHANGING CONCEPTS. Surgery. 1964 Jan;55:57–63. [PubMed] [Google Scholar]
- DETERLING R. A., Jr, VARGAS L. L., McALLISTER F. F. Follow up studies of patients with embolic occlusion of the aortic bifurcation. Ann Surg. 1962 Mar;155:383–391. doi: 10.1097/00000658-196203000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Darling R. C., Austen W. G., Linton R. R. Arterial embolism. Surg Gynecol Obstet. 1967 Jan;124(1):106–114. [PubMed] [Google Scholar]
- Edwards E. A., Tilney N., Lindquist R. R. Causes of peripheral embolism and their significance. JAMA. 1966 Apr 11;196(2):133–138. [PubMed] [Google Scholar]
- Elliott J. P., Jr, Hageman J. H., Szilagyi E., Ramakrishnan V., Bravo J. J., Smith R. F. Arterial embolization: problems of source, multiplicity, recurrence, and delayed treatment. Surgery. 1980 Dec;88(6):833–845. [PubMed] [Google Scholar]
- Flanc C. Saddle embolism of the aorta. Aust N Z J Surg. 1968 May;37(4):384–390. [PubMed] [Google Scholar]
- Fogarty T. J. Catheter technic for arterial embolectomy. J Cardiovasc Surg (Torino) 1967 Jan-Feb;8(1):22–28. [PubMed] [Google Scholar]
- Fogarty T. J., Daily P. O., Shumway N. E., Krippaehne W. Experience with balloon catheter technic for arterial embolectomy. Am J Surg. 1971 Aug;122(2):231–237. doi: 10.1016/0002-9610(71)90323-0. [DOI] [PubMed] [Google Scholar]
- Foster J. H., Carter J. W., Edwards W. H., Graham C. P., Jr Arterial injuries secondary to the use of the Fogarty catheter. Ann Surg. 1970 Jun;171(6):971–978. doi: 10.1097/00000658-197006010-00019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freund U., Romanoff H., Floman Y. Mortality rate following lower limb arterial embolectomy: causative factors. Surgery. 1975 Feb;77(2):201–207. [PubMed] [Google Scholar]
- Gould L., Migliorelli F. Aortic saddle embolus in acute myocardial infarction. Successful removal by a fogarty catheter technic. Am J Cardiol. 1967 Feb;19(2):231–233. doi: 10.1016/0002-9149(67)90538-3. [DOI] [PubMed] [Google Scholar]
- Green R. M., DeWeese J. A., Rob C. G. Arterial embolectomy before and after the Fogarty catheter. Surgery. 1975 Jan;77(1):24–33. [PubMed] [Google Scholar]
- Haimovici H., Moss C. M., Veith F. J. Editorials: Arterial embolectomy revisited. Surgery. 1975 Oct;78(4):409–410. [PubMed] [Google Scholar]
- Hight D. W., Tilney N., Couch N. P. Changing clinical trends in patients with peripheral arterial emboli. Surgery. 1976 Feb;79(02):172–176. [PubMed] [Google Scholar]
- Holm J., Scherstén T. Anticoagulant treatment during and after embolectomy. Acta Chir Scand. 1972;138(7):683–687. [PubMed] [Google Scholar]
- Jarrett F., Dacumos G. C., Crummy A. B., Detmer D. E., Belzer F. O. Late appearance of arterial emboli: diagnosis and management. Surgery. 1979 Dec;86(6):898–905. [PubMed] [Google Scholar]
- Kannel W. B., Abbott R. D., Savage D. D., McNamara P. M. Epidemiologic features of chronic atrial fibrillation: the Framingham study. N Engl J Med. 1982 Apr 29;306(17):1018–1022. doi: 10.1056/NEJM198204293061703. [DOI] [PubMed] [Google Scholar]
- Levin B. H., Giordano J. M. Delayed arterial embolectomy. Surg Gynecol Obstet. 1982 Oct;155(4):549–551. [PubMed] [Google Scholar]
- Levy J. F., Butcher H. R., Jr Arterial emboli: an analysis of 125 patients. Surgery. 1970 Dec;68(6):968–973. [PubMed] [Google Scholar]
- Porter J. M., Acinapura A. J., Silver D. Aortic saddle embolectomy. Arch Surg. 1966 Aug;93(2):360–364. doi: 10.1001/archsurg.1966.01330020152026. [DOI] [PubMed] [Google Scholar]
- READ A. E., BALL K. P., ROB C. G. Embolic occlusion of the aorta in patients with mitral stenosis. Q J Med. 1960 Jul;29:459–471. [PubMed] [Google Scholar]
- Ravdin I. S., Wood F. C. THE SUCCESSFUL REMOVAL OF A SADDLE EMBOLUS OF THE AORTA, 11 DAYS AFTER ACUTE CORONARY OCCLUSION. Ann Surg. 1941 Nov;114(5):834–839. doi: 10.1097/00000658-194111000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SPENCER F. C., EISEMAN B. DELAYED ARTERIAL EMBOLECTOMY--A NEW CONCEPT. Surgery. 1964 Jan;55:64–72. [PubMed] [Google Scholar]
- Sachatello C. R., Killen D. A. Recurrent saddle and iliac emboli following anterior myocardial infarction. South Med J. 1969 Apr;62(4):477–479. doi: 10.1097/00007611-196904000-00025. [DOI] [PubMed] [Google Scholar]
- Satiani B., Gross W. S., Evans W. E. Improved limb salvage after arterial embolectomy. Ann Surg. 1978 Aug;188(2):153–157. doi: 10.1097/00000658-197808000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silvers L. W., Royster T. S., Mulcare R. J. Peripheral arterial emboli and factors in their recurrence rate. Ann Surg. 1980 Aug;192(2):232–236. doi: 10.1097/00000658-198008000-00018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- TAYLOR F. W. Saddle embolus of the aorta. AMA Arch Surg. 1951 Jan;62(1):38–49. doi: 10.1001/archsurg.1951.01250030041005. [DOI] [PubMed] [Google Scholar]
- Thomas T. V. Arterial embolectomy: role of anticoagulants and arteriography. J Cardiovasc Surg (Torino) 1972 Nov-Dec;13(6):584–593. [PubMed] [Google Scholar]
- Thompson J. E., Sigler L., Raut P. S., Austin D. J., Patman R. D. Arterial embolectomy: a 20 year experience with 163 cases. Surgery. 1970 Jan;67(1):212–220. [PubMed] [Google Scholar]
- Thompson J. E., Weston A. S., Sigler L., Raut P. S., Austin D. J., Patman R. D. Arterial embolectomy after acute myocardial infarction. A study of 31 patients. Ann Surg. 1970 Jun;171(6):979–986. doi: 10.1097/00000658-197006010-00020. [DOI] [PMC free article] [PubMed] [Google Scholar]