

Abstract
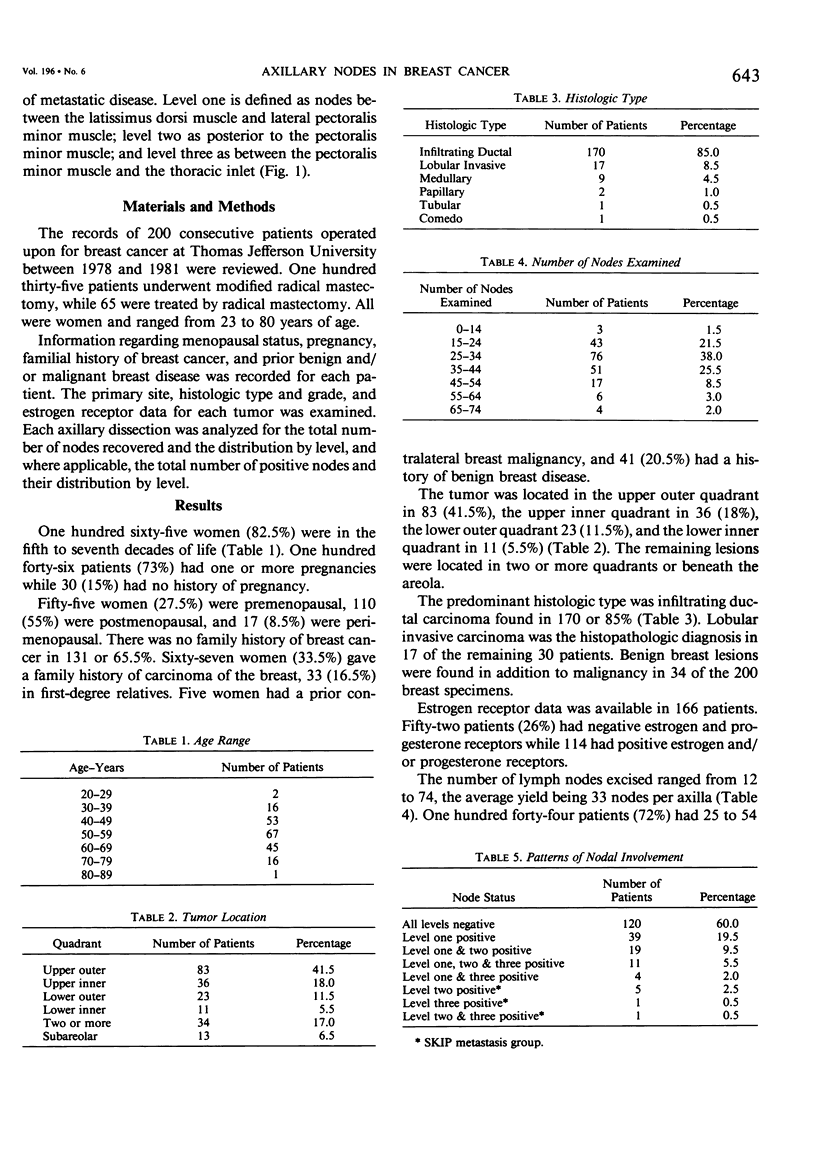
Two hundred consecutive mastectomies with total axillary dissection were analyzed for patterns of involvement at levels one, two and three. The purpose was to determine the accuracy of level one axillary dissection in predicting the status of the entire lymph node chain in carcinoma of the breast. Level one was defined as latissimus dorsi to lateral pectoralis minor; level two behind the pectoralis minor and level three medial pectoralis minor to thoracic inlet. The average number of nodes analyzed per patient was 22. The average number of nodes recovered per level was 14 at level one, 11.5 at level two and eight at level three. One hundred twenty patients (60%) had no nodal involvement, while 80 patients had metastases to axillary lymph nodes. There were seven patients (3.5% of the entire 200) who had positive nodes at levels two and/or three without metastasis to level one. This represents the incidence of "skip" metastases. The group exhibiting "skip" metastases comprise 5.5% of patients (seven of 127) with negative axillary nodes at level one and 8.7% of patients (seven of 80) with axillary metastases secondary to carcinoma of the breast. In the authors' experience, level one lymph node dissection is an accurate predictor of the status of the entire lymph node chain. Negative nodes at level one would indicate lack of involvement at levels two and three with nearly 95% accuracy.
Full text
PDF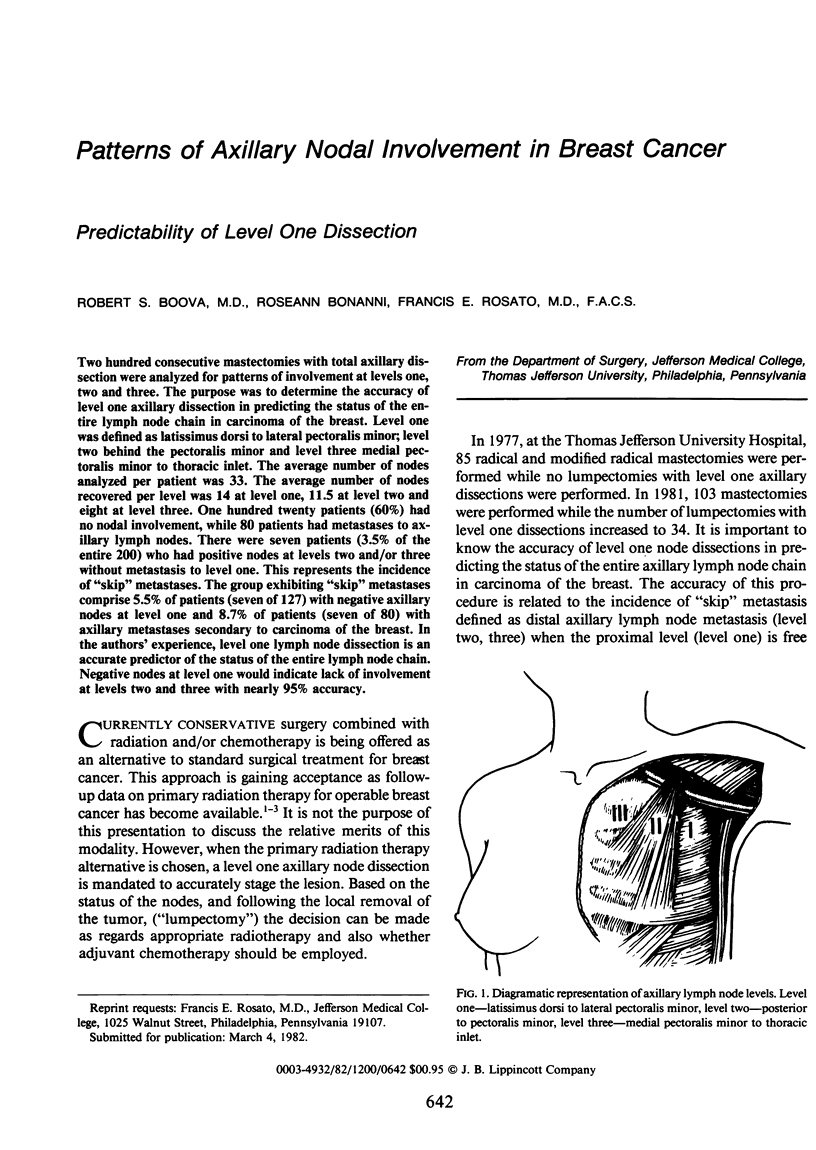
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- AUCHINCLOSS H. SIGNIFICANCE OF LOCATION AND NUMBER OF AXILLARY METASTASES IN CARCINOMA OF THE BREAST. Ann Surg. 1963 Jul;158:37–46. doi: 10.1097/00000658-196307000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BERG J. W. The significance of axillary node levels in the study of breast carcinoma. Cancer. 1955 Jul-Aug;8(4):776–778. doi: 10.1002/1097-0142(1955)8:4<776::aid-cncr2820080421>3.0.co;2-b. [DOI] [PubMed] [Google Scholar]
- Montague E. D., Gutierrez A. E., Barker J. L., Tapley N. D., Fletcher G. H. Conservation surgery and irradiation for the treatment of favorable breast cancer. Cancer. 1979 Mar;43(3):1058–1061. doi: 10.1002/1097-0142(197903)43:3<1058::aid-cncr2820430341>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- Prosnitz L. R., Goldenberg I. S. Radiation therapy as primary treatment for early stage carcinoma of the breast. Cancer. 1975 Jun;35(6):1587–1596. doi: 10.1002/1097-0142(197506)35:6<1587::aid-cncr2820350617>3.0.co;2-w. [DOI] [PubMed] [Google Scholar]
- Smith J. A., 3rd, Gamez-Araujo J. J., Gallager H. S., White E. C., McBride C. M. Carcinoma of the breast: analysis of total lymph node involvement versus level of metastasis. Cancer. 1977 Feb;39(2):527–532. doi: 10.1002/1097-0142(197702)39:2<527::aid-cncr2820390221>3.0.co;2-n. [DOI] [PubMed] [Google Scholar]
- Veronesi U. Value of limited surgery for breast cancer. Semin Oncol. 1978 Dec;5(4):395–402. [PubMed] [Google Scholar]
- Wastell C. Axillary lymph nodes in breast cancer. Surg Annu. 1978;10:123–133. [PubMed] [Google Scholar]