

Abstract
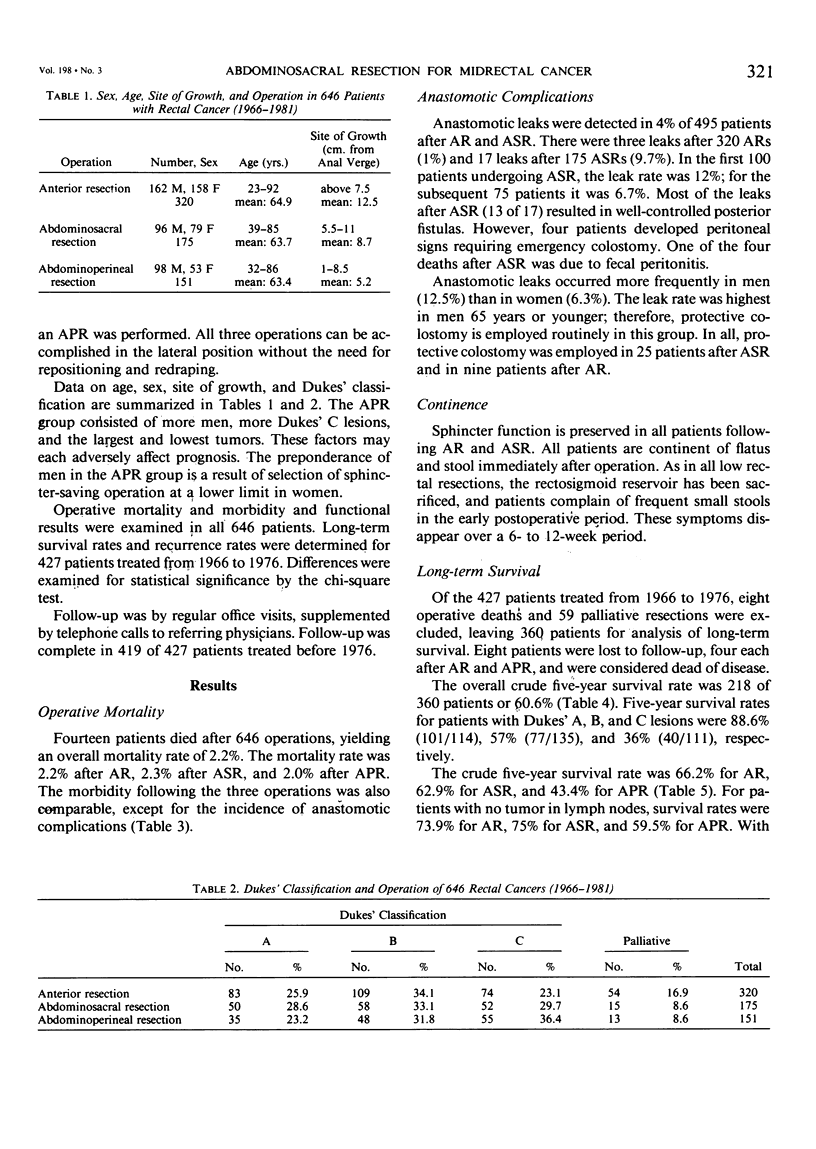
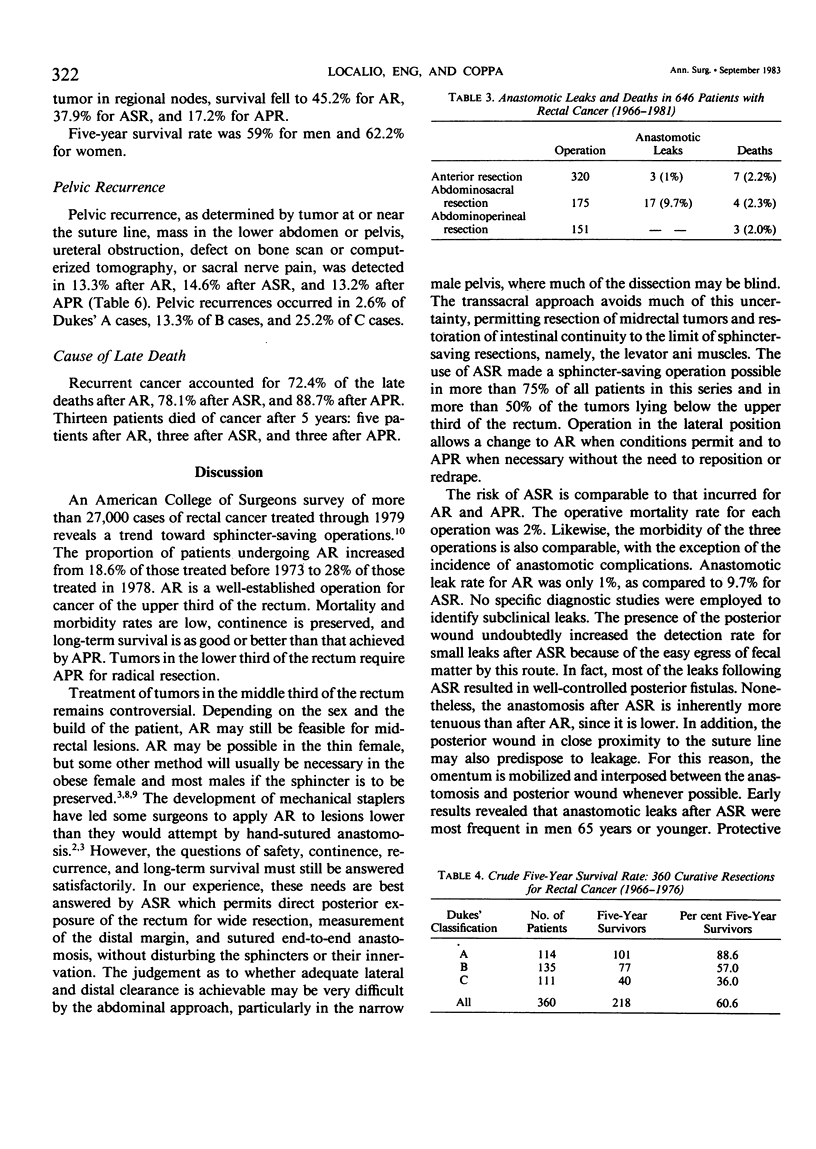
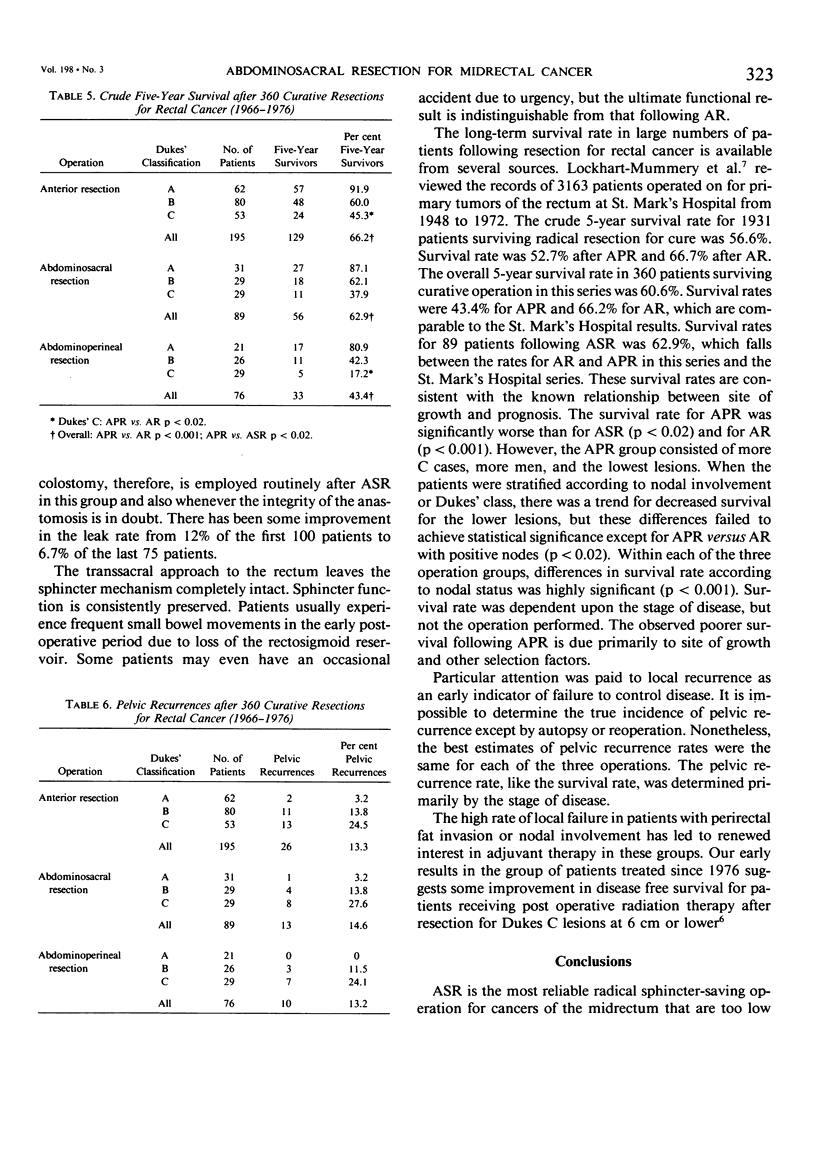
From 1966 to 1981, 646 patients underwent resection for primary adenocarcinoma of the rectum by one surgeon (S.A.L.) in one hospital. The operation, selected by preoperative sigmoidoscopic measurement, was anterior resection (ASR) in 320 patients, abdominosacral resection (ASR) in 175 patients, and abdominoperineal resection (APR) in 151 patients. The operative mortality rate was 2% following each of the operations. Anastomotic complications occurred in less than 2% after AR and in 9.7% after ASR. All patients were completely continent of stool and flatus after AR and ASR. Follow-up is complete in 419 of 427 patients treated from 1966 to 1976. Five-year survival for curative resection (no distant metastases) was 66.2% after AR (129/195), 62.9% after ASR (56/89), and 43.4% after APR (33/76). For patients with no tumor in lymph nodes, survival rates were 73.9% in AR, 75% for ASR, and 59.5% for APR. With involvement of regional lymph nodes, survival fell to 45.2% in AR, 37.9% for ASR, and 17.7% for APR. Pelvic recurrence was detected in 13.3% after AR, 14.6% after ASR, and 13.2% after APR. The authors believe that for midrectal cancer, ASR is the most reliable sphincter-saving procedure. It affords maximum exposure for wide resection of the tumor and safe anastomosis without disrupting the anal sphincters and their innervation. Sphincter preservation can be consistently preserved with no apparent increase in the risk of local recurrence or death from cancer.
Full text
PDF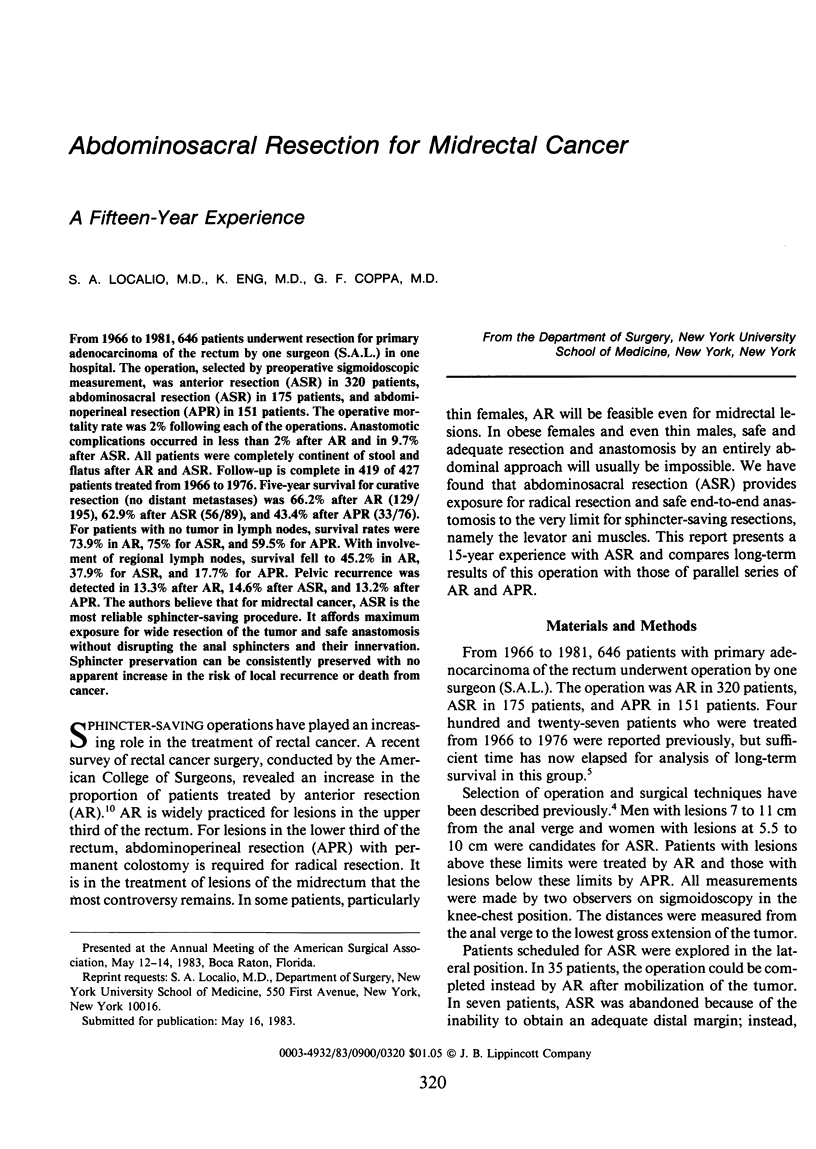

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Beart R. W., Jr, Kelly K. A. Randomized prospective evaluation of the EEA stapler for colorectal anastomoses. Am J Surg. 1981 Jan;141(1):143–147. doi: 10.1016/0002-9610(81)90027-1. [DOI] [PubMed] [Google Scholar]
- Goligher J. C. Use of circular stapling gun with peranal insertion of anorectal purse-string suture for construction of very low colorectal or colo-anal anastomoses. Br J Surg. 1979 Jul;66(7):501–504. doi: 10.1002/bjs.1800660714. [DOI] [PubMed] [Google Scholar]
- Localio S. A., Eng K., Gouge T. H., Ranson J. H. Abdominosacral resection for carcinoma of the midrectum: ten years experience. Ann Surg. 1978 Oct;188(4):475–480. doi: 10.1097/00000658-197810000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Localio S. A., Nealon W., Newall J., Valensi Q. Adjuvant postoperative radiation therapy for Dukes C adenocarcinoma of the rectum. Ann Surg. 1983 Jul;198(1):18–24. doi: 10.1097/00000658-198307000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lockhart-Mummery H. E., Ritchie J. K., Hawley P. R. The results of surgical treatment for carcinoma of the rectum of St Mark's Hospital from 1948 to 1972. Br J Surg. 1976 Sep;63(9):673–677. doi: 10.1002/bjs.1800630902. [DOI] [PubMed] [Google Scholar]
- Mason A. Y. Transsphincteric approach to rectal lesions. Surg Annu. 1977;9:171–194. [PubMed] [Google Scholar]
- Parks A. G. Transanal technique in low rectal anastomosis. Proc R Soc Med. 1972 Nov;65(11):975–976. [PMC free article] [PubMed] [Google Scholar]