

Abstract
Objectives:
We sought to test the safety and efficacy of fluoroscopically guided, video-assisted, thoracoscopic resection after computed tomography (CT)-guided localization using platinum microcoils.
Summary Background Data:
Video-assisted thoracoscopic (VATS) resection of small pulmonary nodules >5 mm deep to the visceral pleura fails to locate the nodule and requires conversion to open thoracotomy in two thirds of cases. Therefore, we developed a new technique for intraoperative localization of these nodules using CT-guided placement of platinum microcoils. This study tests the safety and efficacy of this technique in a Phase I human study.
Methods:
Twelve patients with undiagnosed growing pulmonary nodules <20 mm were marked preoperatively using percutaneously placed CT-guided platinum microcoils. The coil was deployed adjacent to the nodule with the distal end of the coil placed deep to the nodule and the superficial end coiled on the pleural surface. The nodule and coil were excised using endostaplers guided by VATS and fluoroscopy. Histopathologic diagnosis was performed immediately after resection.
Results:
CT-guided microcoil localization was successful in all patients. A small hemothorax and a pneumothorax requiring a chest tube occurred in 2 patients. Mean distance from visceral pleura to the deep edge of the nodule was 30.9 ± 15.4 mm. VATS resection of the nodules (size = 11.8 ± 3.2mm) was successful in all patients. Mean microcoil localization, fluoroscopy, and operative times were 42 ± 14, 3.1 ± 2.0, and 67 ± 27 minutes. A diagnosis of primary nonsmall cell bronchogenic carcinoma was made in 6 patients who then received a completion lobectomy. Six patients (hamartoma: 2, reactive lymph node: 1, bronchoalveolar cell carcinoma: 2, metastatic sarcoma: 1) did not receive further resections.
Conclusions:
Preoperative localization of pulmonary nodules using percutaneous CT-guided platinum microcoil insertion combined with operative fluoroscopic visualization is a safe, effective technique that increases the success rate of VATS excision.
Preoperative localization of small pulmonary nodules using CT-guided, percutaneously deployed, platinum microcoils combined with fluoroscopic guided thoracoscopic resection is a safe and effective technique. Simultaneous marking of the intraparenchymal nodule and the overlying visceral pleural surface increases the success rate of VATS excision.
Lung cancer is the most common cause of cancer death for both men and women in the industrialized world.1 Prognosis for lung cancer is affected by many factors, but one of the most important is the stage of the disease at presentation. Individuals with peripheral lesions less than 3 cm in diameter (T1) are ideal candidates for surgical resection and have the best outcomes, with 5-year survival rates as high as 60% to 80%.2,3 The initial results from screening high-risk lung cancer populations using computed tomography (CT) have conclusively shown CT is more sensitive than chest radiographs for detecting small lung cancers.4–6 Given the worldwide interest in screening for lung cancer, it is likely that a large number of small growing nodules will be detected that will require further investigation.7
The detection of a small growing lung nodule on chest CT raises the suspicion of lung cancer, but proof of malignancy must be established by either needle biopsy or nodule resection. Many centers excise these small growing nodules using video-assisted thoracoscopic surgery (VATS) to minimize postoperative morbidity and to remove as small a volume of lung tissue as possible. However, Suzuki,8 reported that failure to visualize or palpate the nodule resulted in 54% of patients requiring conversion from VATS to thoracotomy for successful resection. This conversion occurred in 63% of patients if the nodule was less than or equal to 10 mm in diameter and greater than 5 mm from the pleural surface.
A number of small nodule localization techniques have been developed in an attempt to improve the accuracy of thoracoscopic resection, but these techniques have many limitations and have not been put into general practice. Recently, we have developed a novel technique whereby a commercially available vascular embolization microcoil (80 mm long, 0.018-inch diameter fiber-coated, platinum wire) was placed in the lung parenchyma of a pig using CT guidance.9 These coils were delivered percutaneously via a 22-gauge needle with one end embedded in lung parenchyma and the other end coiled in the pleural space. Using the animal model, we showed that these coils can be deployed safely and easily, and subsequently localized and resected using fluoroscopically guided, thoracoscopic, wedge resection.
The purpose of this human phase I study was to determine if this microcoil technique could be safely used in humans with small peripheral lung nodules. We hypothesized that this preoperative procedure would increase the VATS resection of small pulmonary nodules and decrease the rate of conversion to thoracotomy.
MATERIALS AND METHODS
The study protocol and patient consent forms were approved by the Institutional Review Board of the Vancouver Hospital and Health Sciences Centre and the University of British Columbia.
Patient Selection
Patients referred to our institution for surgery with growing pulmonary nodules less than 20 mm in maximum long axis diameter in peripheral lung, between April 1, 2003, and November 15, 2003, were evaluated and, if eligibility criteria were met, approached to participate in the study. Thirteen patients agreed to participate after being informed of the risks and benefits of the procedure as well as all the alternatives for treatment.
Preoperative CT Review
The preoperative CT scan was jointly reviewed by the surgeon (R.F., K.E., J.Y.) and the radiologist (T.P., J.M.) to determine whether the nodule could be excised using thoracoscopic staple wedge techniques. Nodule lobar location, size, depth from the nearest overlying pleural surface, and mean density were assessed and recorded using electronic calipers on the scanner workstation. Preoperative variables, including smoking history, FEV1, and the presence of emphysema on CT scan were recorded.
Radiologic Localization Procedure
The CT-guided percutaneous microcoil nodule localization procedure was performed using conscious sedation and local anesthesia. A CT scan was performed using a Siemens Sensation 16 multidetector-row CT scanner (Siemens Medical Systems, Erlangen, Germany) to localize the nodule. The scan protocol used was identical to the lung cancer screening follow-up protocol used in our institution (16-slice helical acquisition mode, 0.75-mm detector aperture, table speed 3.6 cm per second, beam pitch 1.5, 320 mA, 0.5-second rotation time and 120 kVp). One-mm thick images were reconstructed at 1-mm intervals using a 180 linear-interpolation algorithm and both low (B45) and high (B60) spatial frequency reconstruction algorithms. The images were archived in the DICOM 3.0 format. The CT scan was used to plan the needle access route and measure the depth of the nodule from the external surface of the chest wall.
An 80-mm long, fiber-coated 0.018-inch diameter platinum microcoil (Vortx-18, Diamond Shape, Boston Scientific, Cork, Ireland) was completely loaded into a 100- or 150-mm long Chiba needle with 10-mm graduations on the needle shaft (Cook (Canada) Inc., Stouffville, Ontario, Canada). A 40-cm, 0.018-inch diameter, guide wire from a micropuncture catheter introducer set (Mini-Stick Kit, Boston Scientific, Waterton, MA) was marked at 2 points; the length necessary to eject 30 mm of the fiber coated coil and the length necessary to eject the entire coil from the Chiba needle.
Using CT guidance, the tip of the loaded Chiba needle was percutaneously placed approximately 5 mm deep to the lung nodule. The guide wire was introduced up to the first mark, advancing 30 mm of the 80-mm long fiber-coated microcoil out of the Chiba needle and into the lung parenchyma where it assumed a tightly coiled helical configuration adjacent to the nodule (Figs. 1a and 2). A second localized CT scan was performed to confirm that the first 30 mm of coil was successfully deployed and to measure the distance from the tip of the Chiba needle to the pleural surface of the lung. Using the graduation on the needle, the Chiba needle tip was retracted from its location adjacent to the nodule to the pleural surface while holding the stiff end of the guide wire in place. This maneuver deployed a straight segment of microcoil along the needle tract, from the nodule to the pleural surface of the lung. Then the needle was held stationary and the guide wire advanced to the second mark, ejecting the remaining microcoil from the needle (Fig. 1b). Once pushed out of the Chiba needle, the end of the fiber-coated microcoil formed a compact helical configuration on the visceral pleural surface. The empty Chiba needle was then removed from the chest wall (Figs. 1c and 3).

FIGURE 1. A, 3 to 5 cm of the microcoil were initially deployed within 10 mm of the lung nodule within the lung. B, The needle was then retracted to the pleural edge and the remainder of the microcoil deployed onto the pleural surface. C, The nodule and coil were completely excised using endostaplers under fluoroscopic and thoracoscopic guidance.

FIGURE 2. Chiba needle loaded with a microcoil has been introduced into the lung using CT guidance. The needle touches the posterior edge of a 10-mm diameter growing nodule in this 54-year-old female who had previously attended a CT lung cancer-screening program.

FIGURE 3. Microcoil ejected from the 22-gauge Chiba needle, sitting with the deep end coiled adjacent to the 8-mm nodule and the superficial end coiled on the visceral pleural surface. A small associated pneumothorax is noted.
A CT scan was obtained to assess the position of the microcoil relative to the lesion and the pleural space and to assess for the presence of hemorrhage and pneumothorax. The CT images were also reconstructed as a 3-dimensional image using a Leonardo medical workstation (Siemens Medical Systems, Erlangen, Germany) to measure the distance from the microcoil to the nodule. The patient was then transferred to the operating theater.
Surgical Procedure
In the operating room, the patient was placed in the lateral position under general anesthesia. A double lumen endotracheal tube was inserted and the involved lung deflated. A 5-mm thoracoscopic port was inserted into the pleural space and the microcoil located on the visceral pleural surface. Based on the position of the microcoil, 2 other ports were placed to insert a grasping instrument and a linear stapling device (Endo GIA II –United States Surgical, Norwalk, CT). The pleural end of the microcoil and adjacent lung surface were grasped together and elevated. Fluoroscopy was used to visualize the deep end of the coil and to guide the placement of the endoscopic staplers (Fig. 4). The resected lung was placed in an endoscopic retrieval bag and withdrawn through the chest wall. Excision of the complete microcoil and nodule was confirmed fluoroscopically and the specimen sent for frozen section.
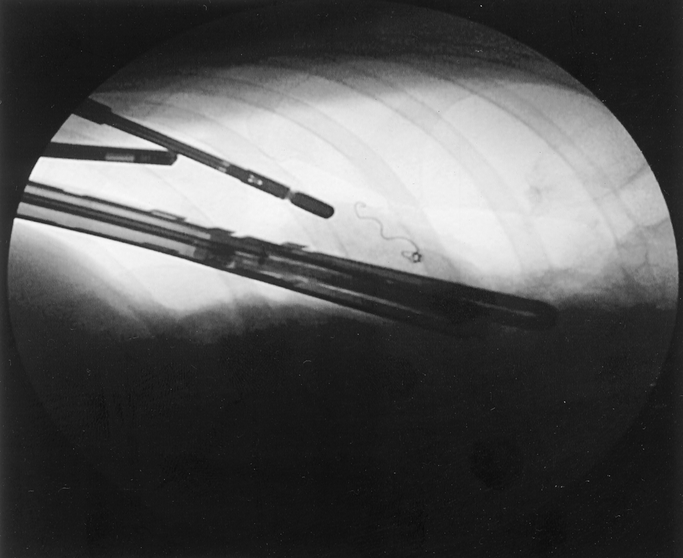
FIGURE 4. Intraoperative fluoroscopy image showing the microcoil within peripheral lung that is being excised using a GIA stapler. A grasper has been applied to the lung adjacent to the coiled end of the microcoil on the visceral pleura.
An experienced pulmonary pathologist examined the wedge resection according to accepted clinical practice at our institution. A frozen section block was removed from the nodule for histologic diagnosis. If the lesion was found to be a nonsmall cell lung cancer the patient received intraoperative staging to determine resectability. If the patient had adequate cardiopulmonary reserve and the lesion was resectable, a formal lobectomy was performed. If the lesion was determined to be benign or completely resected, metastatic or well differentiated bronchoalveolar cancer, the thoracic cavity was irrigated with saline and a small chest tube was put in place and attached to underwater drainage. The lung was re-expanded, the incisions closed, and the patient transported to the postanesthetic recovery room.
Perioperative variables, including CT-guided microcoil placement time, length of general anesthesia, surgical operating time, number and types of operating ports, and number and types of disposable endoscopic staple cartridges, were recorded. Pathologic variables including size, shape and histology of the lesion, and minimum and maximum resection margins from the edge of the tumor were assessed. Postoperative recovery room time, length of hospital stay (LOS), duration of air leak from chest tubes, total blood loss from chest tubes, postoperative complications and analgesic use were recorded.
RESULTS
Thirteen patients were enrolled in the trial. One patient, during the preoperative CT review was excluded because the nodule was located too close to the inferior pulmonary vein to allow safe wedge excision. All 12 remaining patients underwent successful fluoroscopically guided video-assisted thoracoscopic resection of small peripheral lung nodules after CT-guided microcoil localization. The mean patient age was 61 ± 10 years (range, 43–70). Six patients were male (50%). The mean weight was 81 ± 16 kg (range, 62–118 kg). The mean height was 171 ± 13 cm. The preoperative FEV1 was 2.97 ± 0.81 L (range 1.76–4.07 L). Five patients had emphysema visible on the preprocedure CT scan.
The mean nodule size was 11.8 ± 3.2 mm. (range, 6–18 mm) with a mean CT attenuation of 34 ± 69 HU (range, 9–155 HU).There was 1 nodule located in the right upper, 2 in right middle, 2 in the right lower, 4 in the left upper, and 3 in the left lower lobe. The distance from the most superficial edge of the nodule to the visceral pleura was 19 ± 14 mm (range, 2–45 mm) and the distance to the deepest edge was 31 ± 15 mm (range, 10–54 mm).
The time for CT guided insertion of the microcoil was 42 ±16 min (range, 21–79 min). The distal end of the coil was located within 10 mm of the lesion in all but 1 case. The mean distance from the distal end of the coil to the visceral pleural surface was 29 ± 13 mm (range, 14–46). The proximal end of the microcoil was deployed on the pleural surface in 9 patients, within 1 mm of the lung visceral pleural surface in 1 patient and tethered within the chest wall under the parietal pleura in 2 patients. In the 2 cases where the coil was tethered within the chest wall, 1 coil was successfully extracted from the chest wall at the time of thoracoscopy without displacement of the intrapulmonary portion of the coil. The nodule and coil were successfully excised. In the other case, the coil pulled out of the lung during deflation of the lung. Fortunately, the entry site of the microcoil was visible on the visceral pleural surface at thoracoscopy and was permanently marked using cautery. This nodule was also successfully excised using the VATS technique by measuring the depth of the nodule on the CT scan. After deployment of the coil, one patient with emphysema required a chest tube for decompression of a symptomatic pneumothorax in the CT suite. One other patient had approximately 30 mL of blood found at thoracoscopy.
Complete nodule excision using endostaplers guided by VATS and fluoroscopy was successful in all of the patients. Mean fluoroscopy and operative times for resection of the nodule were 3.1 ± 2 (range, 1–7) and 67 ± 27 (range, 20–98) minutes. The mean number of staple lines placed was 5 ± 2 (range, 3–9) cartridges.
Frozen section histopathology provided adequate information for correct intraoperative patient management in all cases. Permanent section analysis confirmed the frozen section diagnosis in all cases. The soft metal of the microcoil did not affect the sectioning for pathologic analysis. Three patients had benign disease (hamartoma: 2, reactive lymph node: 1) and underwent no further resections (Table 1). Three patients had complete wedge resections of either well-differentiated bronchoalveolar carcinomas (n = 2) or metastatic spindle cell sarcoma (n =1) and also received no further resections. The length of stay (LOS) for these VATS resected patients was 2.7 ± 0.6 days, and there were no postoperative complications.
TABLE 1. Patient Nodule Characteristics With Clinical and Histopathological Correlation

The remaining 6 patients, 5 with adenocarcinoma and 1 with squamous cell carcinoma, received a completion lobectomy via transaxillary thoracotomy. Tumor staging for these cancers was: T1N0 = 4, T1N1 = 1, and T1N2 = 1. The LOS for this group was 12.2 ± 15 days (range, 3–40 days). Postoperative complications in the completion lobectomy group included atrial fibrillation (n = 2), prolonged air leak (n = 2) and aspiration pneumonia.
The preoperative treatment plan of 5 patients was changed after nodule resection. Three patients with either a negative percutaneous needle biopsy or negative positron emission tomography (PET) scans were found to harbor malignant nodules. Two patients with positive PET scans were shown to have benign nodules after resection (Table 1).
The mean postoperative follow-up has been 2.5 ± 1.7 months, and there have been no deaths in the study group. The mean changes in total lung capacity (TLC) and forced expiratory volume in 1 second (FEV1) in the patients receiving wedge resections were 0.39 ± 0.21 L (5.2% decrease from preoperative value of 7.37 L) and 0.25 ± 0.11 L (7% reduction from preoperative value of 3.57 L). The patient with a spindle cell sarcoma metastasis developed further metastases 4 months following wedge excision. No other patients have developed recurrent disease.
DISCUSSION
This study shows that small peripheral lung nodules can be safely marked using CT-guided placement of fiber-coated platinum microcoils. The localization procedure is technically similar to that used for standard CT-guided fine-needle aspiration lung biopsy. This procedure allows the accurate intraoperative fluoroscopic localization of the marker with successful excision of these nodules using VATS techniques. Using this localization procedure, open thoracotomy was avoided in the 50% of our patients who were found to have lesions not requiring therapeutic lobectomy.
The current management of growing small lung nodules or those with suspicious CT findings (spiculated margins, lobulation, mixed ground glass and solid morphology) is CT directed percutaneous needle biopsy or surgical excision. CT-guided fine-needle biopsy of subcentimeter nodules can be difficult, and the tissue obtained is often nondiagnostic.10–12 Perioperative complications and length of stay are reduced compared with thoracotomy when these small nodules are excised using an endoscopic stapling device directed by a video assisted thoracoscope. Small nodules are often visible with the thoracoscope if they lie within 5 mm of the visceral pleural surface, but if they are located deeper in the lung, they need to be palpated to locate them for excision. Suzuki et al8 found that 54% of 92 patients undergoing video assisted thoracoscopic surgery required conversion to thoracotomy. The most common reason for conversion to full thoracotomy was failure to locate the nodule. Univariate and multivariate analysis of eleven nodule variables showed that if the distance from the pleural surface to the nodule edge was greater than 5 mm, the failure rate for nodule detection was 63%. Forty percent of these nodules were found to be malignant. Because of the localization problem at surgery and the increasing clinical load of small lung nodules found using CT lung cancer screening, there has been extensive investigation into localization techniques to assist in resecting small nodules at video assisted thoracoscopy.
Pulmonary localizing techniques have been classified into 3 types.13 The first uses intraoperative imaging, either intraoperative ultrasonography14–16 or intraoperative CT.17,18 Localization with intraoperative ultrasound is difficult as the lung must be completely collapsed to visualize small nodules. This lengthens the surgery as the complete collapse of the lung can take between 30 to150 minutes and is often impossible in patients with extensive emphysema. Experience with real-time CT guidance of thoracoscopic resection is limited but artifact from instruments and staples degrades the CT image and the limited space within the scanner gantry makes surgery difficult.19
The second class of targeting techniques includes percutaneous injection of dyes,20,21 contrast media,22,23 radionuclides,24 or colored adhesive agents.25 Diffusion away from the nodule is a limitation of these techniques and imposes restrictions on the allowable time between the CT localization procedure and thoracoscopic resection. This can cause difficulties in operating room scheduling. Also, dyes such as methylene blue carry a possible risk of anaphylactic reactions following injection20 and are often difficult to visualize on the visceral pleural surface in patients with extensive anthracotic pigmentation of the lungs. Radiographic contrast media (Lipiodol, barium)22,23 can also rapidly diffuse away from the nodule and into the pulmonary lymphatics. Because these materials are not water-soluble they carry potential risk of stroke if they gain access to the pulmonary veins.
The third class of targeting techniques uses percutaneous hook wire26–31 or wire coil placement.28,32,33 Percutaneous localization using a mammographic needle and hook wire is one of the most common methods used.26 However, a high incidence of preoperative wire dislodgement with associated pneumothorax, intrapulmonary hemorrhage and pleural pain have been reported with this technique.28,30,34 All hook wires cause visible tearing and damage if dislodged35 and may cause massive air embolism.36 Variations of the technique using both short hook wires13 and short platinum microcoils32 attached to sutures have been reported.
The 0.018-inch microcoils used in this study are soft and pliable and cause little damage to lung tissue, even when dislodged. Gagliano et al35 compared microcoil and hook wires for localization in ex vivo goat lungs. They reported that when a microcoil is displaced, it uncoils causing minimal tissue damage. In addition, the “fuzzy” fiber coating on these microcoils induces coagulation and increases the adhesion of the coil to the lung tissue. The coiled configuration and fiber coating virtually eliminates the risk of embolization.
The data from the current study suggest that CT-guided microcoil localization results in a similar complication profile and rate as has been reported for CT-guided, fine-needle, aspiration biopsy.37–39 The 1 patient requiring insertion of a chest tube had in fact suffered a pneumothorax during a previous attempt at fine-needle aspiration biopsy, secondary to significant, underlying emphysema. The 1 patient with a small hemothorax was asymptomatic and the hemothorax was only visible at thoracoscopy. A review of the CT images and the 3-dimensional reconstruction images indicated that the deepest part of the microcoil was successfully deployed to within 10 mm of the lesion in 11 of 12 patients and the most superficial part of the coil was deployed on the visceral pleura in 9 of 12 patients. VATS resection of the nodules was successful in all patients. There were no intraoperative complications during the wedge resection. We note that care must be taken during initial deflation of the lung, at thoracoscopy, to ensure that the superficial end of the coil is not retained in the chest wall. If chest wall placement occurs, the pleural end of the coil is removed from the chest wall via thoracoscopy to avoid any subsequent dislodgement of the microcoil from lung tissue.
A definitive diagnosis was made in all 12 patients. The management of 5 patients who had undergone routine preoperative investigations was changed after resection of the nodule. Three patients with malignant nodules had previous negative percutaneous CT-guided, fine-needle, aspiration biopsy or negative PET scans. Two patients with benign nodules had positive PET scans preoperatively. The 2 patients with small adenocarcinomas showing histologic features of well differentiated bronchoalveolar cell cancer were treated with wedge resection alone because these tumors have a propensity to develop future multifocal lesions. Neither of these patients has shown recurrent disease on follow-up. Although the gold standard for surgical resection of small nonsmall cell cancer is lobectomy,40 there is evidence that complete nonanatomic resections of well differentiated bronchoalveolar cell cancers have similar survival rates compared with lobectomy.41
In conclusion, this study suggests that this CT-guided percutaneous, needle-deployed microcoil system provides a fast, effective and safe method for localization of small peripheral lung nodules prior to thoracoscopic wedge resection. The technique allows simultaneous marking of the intraparenchymal nodule and the overlying visceral pleural surface. A randomized trial of this technique is planned to confirm these preliminary results. We would also like to thank the British Columbia Lung Association for their support.
ACKNOWLEDGMENTS
We would like to acknowledge the following for their participation, help and support in this study: Steve Kalloger (Radiology); Rhonda Lancaster, Ron Chitsaz, Donna Lopez (CT); Dr. Annette Williamson, Dr. Stephen Lam (Lung Health Study); and Dr. Julia Flint (Pathology).
Discussions
Dr. Alden H. Harken (Oakland, California): I want to compliment Dr. Finley and his group for solving a very real surgical problem. This is a difficult issue for many thoracic surgeons, and, as he points out, it is getting tougher as the imaging strategies get better. In our patients, we are now turning up nodules that are hard to find surgically. And I commend you for borrowing from some of our general surgical colleagues in the breast area and in the tattooing of the colon to try to find these things.
I have 3 questions. First, the contraindications to the procedure—you say that a surgeon and a radiologist convened to look at the films prior to this, and you indicate that in one instance you thought that the lesion was a little close to one of the pulmonary veins. Are there any other contraindications? Can you detect pleurodesis, preoperative bullous disease, or other potential technical problems?
The second is, you indicated that in 2 instances the microcoil pulled out, but in one of those instances you were able to detect where it had violated the visceral pleura and that was sufficient for you to identify the nodule. Does that mean that if you just tattooed the visceral pleura that would be sufficient?
Next is the preoperative evaluation of these patients that present with small undiagnosed lung nodules. As you indicate, this is our problem, you see a little lump and you have got to figure, is there any solution other than taking that lump out? And you point out that the fine needle aspirate was confusing at best in several instances. And many of our hospitals that have purchased PET scanners are desperate to find some reason to use the PET scanner. But the 3 of your patients with cancer had a negative PET scan and 2 of your patients with benign disease exhibited a positive PET scan. Would you now suggest that it is irresponsible to get a PET scan prior to one of these procedures?
Finally, you are now pushing the envelope in the mean size of these nodules was 1.18 centimeters. If you believe, as I do, that a regional lymphadenectomy is diagnostic, not therapeutic, is there any reason to perform a standard anatomic lobectomy for therapy of these patients and would your wedge resection be sufficient?
Thank you again for solving a very real problem.
Dr. Richard J. Finley (Vancouver, British Columbia, Canada): Thank you, Dr. Harkin, for your questions.
With the evolution of thin sliced CT scan, thoracic surgeons are being asked to take out smaller and smaller nodules. The body of knowledge for the thoracoscopic excision of these nodules is also evolving. The major goal is to carry out the procedure safely and effectively. One patient was excluded from our study since the pulmonary nodule was too close to one of the main branches of the pulmonary vein to safely excise the lesion with a stapler. The radiologists and thoracic surgeons at the Vancouver General Hospital are presently mapping out the areas of the lung where these nodules can be safely excised. The deepest nodule that we have excised was 54 mm from the visceral pleural surface. Fortunately, the fissures were developed in this patient allowing resection. We are also looking at pre-operative methods using the CT scanner to determine whether the fissures are fused. At the present time, thoracoscopy is the only accurate way to determine if a fissure is complete or incomplete.
Two patients in our study had the proximal end of the microcoil deployed in the chest wall. These deployments were carried out early in our study period. We have learned to place the proximal end of the microcoil deeper into the lung in order to avoid dislodgement of the microcoil with deflation of the lung. One of the proximal ends of the microcoil was visualized at the time thoracoscopy and carefully removed from the chest wall avoiding dislodgement from the lung. The other patient had the distal end of the microcoil dislodge from the lung. Fortunately, we were able to see the puncture site in the lung during thoracoscopy and to safely remove the nodule using a combination of thoracoscopy and fluoroscopy.
Non-invasive diagnosis of pulmonary nodules has been improved with the introduction of CT PET scans. I believe that we need to keep an open mind about the accuracy of the PET scan in determining pathology of these undiagnosed lesions. At the present times, nodules below 15 mm are difficult to diagnose with PET scan. I believe, we will be using the CT PET for diagnosis and staging of these nodules similar to the sentinel node mapping technique used in the staging of breast cancer.
At the present time, the Lung Cancer Study Group paper by Ginsberg and his colleagues showed that lobectomy is the gold standard for treatment of T1 non-small cell lung cancers. As we continue to identify smaller lung cancers (less than 15 mm) a new study needs to be done to exam the efficacy of segmental or non-anatomical resection versus lobectomy. The study is supported by evidence from the Japanese literature that shows equivalent survival with wedge resection versus lobectomy for bronchoalveolar cell cancers.
Thank you.
Footnotes
Supported by British Columbia Lung Association.
Reprints: Richard J. Finley, MD, FRCSC, Department of Surgery, Vancouver hospital and Health Sciences Centre, 910 West 10th Avenue, Vancouver, BC, Canada V7V3A2. E-mail: rjfinley@interchange.ubc.ca.
REFERENCES
- 1.Jemal A, Murray T, Samuels A, et al. Cancer statistics, 2003. CA Cancer J Clin. 2003;53:5–26. [DOI] [PubMed] [Google Scholar]
- 2.Miller DL, Rowland CM, Deschamps C, et al. Surgical treatment of non-small cell lung cancer 1 cm or less in diameter. Ann Thorac Surg. 2002;73:1545–1550; discussion 1550–1551. [DOI] [PubMed]
- 3.Martini N, Bains MS, Burt ME, et al. Incidence of local recurrence and second primary tumors in resected stage I lung cancer. J Thorac Cardiovasc Surg. 1995;109:120–129. [DOI] [PubMed] [Google Scholar]
- 4.Henschke CI, Naidich DP, Yankelevitz DF, et al. Early lung cancer action project: initial findings on repeat screenings. Cancer. 2001;92:153–159. [DOI] [PubMed] [Google Scholar]
- 5.Kaneko M, Eguchi K, Ohmatsu H, et al. Peripheral lung cancer: screening and detection with low-dose spiral CT versus radiography. Radiology. 1996;201:798–802. [DOI] [PubMed] [Google Scholar]
- 6.Sone S, Takashima S, Li F, et al. Mass screening for lung cancer with mobile spiral computed tomography scanner. Lancet. 1998;351:1242–1245. [DOI] [PubMed] [Google Scholar]
- 7.Leef JL 3rd, Klein JS. The solitary pulmonary nodule. Radiol Clin North Am 2002;40:123–143, ix. [DOI] [PubMed] [Google Scholar]
- 8.Suzuki K, Nagai K, Yoshida J, et al. Video-assisted thoracoscopic surgery for small indeterminate pulmonary nodules: indications for preoperative marking. Chest. 1999;115:563–568. [DOI] [PubMed] [Google Scholar]
- 9.Powell T, Jangra D, Kalloger S, et al. Peripheral lung nodules: CT-guided insertion of platinum microcoil markers to aid thoracoscopic resection. Lung Cancer 2003;41(2 Suppl):s9. [Google Scholar]
- 10.Li H, Boiselle PM, Shepard JO, et al. Diagnostic accuracy and safety of CT-guided percutaneous needle aspiration biopsy of the lung: comparison of small and large pulmonary nodules. AJR Am J Roentgenol. 1996;167:105–109. [DOI] [PubMed] [Google Scholar]
- 11.vanSonnenberg E, Casola G, Ho M, et al. Difficult thoracic lesions: CT-guided biopsy experience in 150 cases. Radiology. 1988;167:457–461. [DOI] [PubMed] [Google Scholar]
- 12.Tsukada H, Satou T, Iwashima A, et al. Diagnostic accuracy of CT-guided automated needle biopsy of lung nodules. AJR Am J Roentgenol. 2000;175:239–243. [DOI] [PubMed] [Google Scholar]
- 13.Dendo S, Kanazawa S, Ando A, et al. Preoperative localization of small pulmonary lesions with a short hook wire and suture system: experience with 168 procedures. Radiology. 2002;225:511–518. [DOI] [PubMed] [Google Scholar]
- 14.Greenfield AL, Steiner RM, Liu JB, et al. Sonographic guidance for the localization of peripheral pulmonary nodules during thoracoscopy. AJR Am J Roentgenol. 1997;168:1057–1060. [DOI] [PubMed] [Google Scholar]
- 15.Santambrogio R, Montorsi M, Bianchi P, et al. Intraoperative ultrasound during thoracoscopic procedures for solitary pulmonary nodules. Ann Thorac Surg. 1999;68:218–222. [DOI] [PubMed] [Google Scholar]
- 16.Sortini A, Carrella G, Sortini D, et al. Single pulmonary nodules: localization with intrathoracoscopic ultrasound–a prospective study. Eur J Cardiothorac Surg. 2002;22:440–442. [DOI] [PubMed] [Google Scholar]
- 17.Akamatsu H, Sunamori M, Katsuo K. Thoracoscopic lung resection for extremely small nodular lesions using simultaneous intraoperative real-time computed tomography. Thorac Cardiovasc Surg. 2000;48:34–35. [DOI] [PubMed] [Google Scholar]
- 18.Coxson HO MJ, Kalloger SE, Lara-Guerra H, et al. Computed tomography guided resection of simulated small peripheral lung nodules using thoracoscopic surgical techniques. Radiology 2002;225:293. [Google Scholar]
- 19.Jangra D, Finley R, Lara-Guerra H, et al. The effect of surgical instrumentation and endoscopic staplers on real-time CT images of subcentimeter thoracic nodules. Canadian Association of Thoracic Surgeons Annual Scientific Meeting. London, Ontario, 2002. [Google Scholar]
- 20.Lenglinger FX, Schwarz CD, Artmann W. Localization of pulmonary nodules before thoracoscopic surgery: value of percutaneous staining with methylene blue. AJR Am J Roentgenol. 1994;163:297–300. [DOI] [PubMed] [Google Scholar]
- 21.Vandoni RE, Cuttat JF, Wicky S, Suter M. CT-guided methylene-blue labelling before thoracoscopic resection of pulmonary nodules. Eur J Cardiothorac Surg. 1998;14:265–270. [DOI] [PubMed] [Google Scholar]
- 22.Moon SW, Wang YP, Jo KH, et al. Fluoroscopy-aided thoracoscopic resection of pulmonary nodule localized with contrast media. Ann Thorac Surg. 1999;68:1815–1820. [DOI] [PubMed] [Google Scholar]
- 23.Choi BG, Kim HH, Kim BS, et al. Pulmonary nodules: CT-guided contrast material localization for thoracoscopic resection. Radiology. 1998;208:399–401. [DOI] [PubMed] [Google Scholar]
- 24.Chella A, Lucchi M, Ambrogi M, et al. A pilot study of the role of TC-99 radionuclide in localization of pulmonary nodular lesions for thoracoscopic resection. Eur J Cardio-Thoracic Surg. 2000;18:17–21. [DOI] [PubMed] [Google Scholar]
- 25.Yoshida J, Nagai K, Nishimura M, et al. Computed tomography-fluoroscopy guided injection of cyanoacrylate to mark a pulmonary nodule for thoracoscopic resection. Jpn J Thorac Cardiovasc Surg. 1999;47:210–213. [DOI] [PubMed] [Google Scholar]
- 26.Mack MJ, Gordon MJ, Postma TW, et al. Percutaneous localization of pulmonary nodules for thoracoscopic lung resection. Ann Thorac Surg. 1992;53:1123–1124. [DOI] [PubMed] [Google Scholar]
- 27.Mack MJ, Shennib H, Landreneau RJ, et al. Techniques for localization of pulmonary nodules for thoracoscopic resection. J Thorac Cardiovasc Surg. 1993;106:550–553. [PubMed] [Google Scholar]
- 28.Mullan BF, Stanford W, Barnhart W, et al. Lung nodules: improved wire for CT-guided localization. Radiology. 1999;211:561–565. [DOI] [PubMed] [Google Scholar]
- 29.Plunkett MB, Peterson MS, Landreneau RJ, et al. Peripheral pulmonary nodules: preoperative percutaneous needle localization with CT guidance. Radiology. 1992;185:274–276. [DOI] [PubMed] [Google Scholar]
- 30.Shah RM, Spirn PW, Salazar AM, et al. Localization of peripheral pulmonary nodules for thoracoscopic excision: value of CT-guided wire placement. AJR Am J Roentgenol. 1993;161:279–283. [DOI] [PubMed] [Google Scholar]
- 31.Templeton PA, Krasna M. Needle/wire lung nodule localization for thoracoscopic resection. Chest. 1993;104:953–954. [DOI] [PubMed] [Google Scholar]
- 32.Reinschmidt JP, Murray SP, Casha LM, et al. Localization of pulmonary nodules using suture-ligated microcoils. J Comput Assist Tomogr. 2001;25:314–318. [DOI] [PubMed] [Google Scholar]
- 33.Partik BL, Leung AN, Muller MR, et al. Using a dedicated lung-marker system for localization of pulmonary nodules before thoracoscopic surgery. AJR Am J Roentgenol. 2003;180:805–809. [DOI] [PubMed] [Google Scholar]
- 34.Thaete FL, Peterson MS, Plunkett MB, et al. Computed tomography-guided wire localization of pulmonary lesions before thoracoscopic resection: results in 101 cases. J Thorac Imaging. 1999;14:90–98. [DOI] [PubMed] [Google Scholar]
- 35.Gagliano RA, Murray SP, Casha LM, Tracy D, Collins GJ. A novel method of transthoracic lung nodule localization. Curr Surg. 1999;56:410–412. [Google Scholar]
- 36.Horan TA, Pinheiro PM, Araujo LM, et al. Massive gas embolism during pulmonary nodule hook wire localization. Ann Thorac Surg. 2002;73:1647–1649. [DOI] [PubMed] [Google Scholar]
- 37.Cox JE, Chiles C, McManus CM, et al. Transthoracic needle aspiration biopsy: variables that affect risk of pneumothorax. Radiology. 1999;212:165–168. [DOI] [PubMed] [Google Scholar]
- 38.Wallace MJ, Krishnamurthy S, Broemeling LD, et al. CT-guided percutaneous fine-needle aspiration biopsy of small (< or =1-cm) pulmonary lesions. Radiology. 2002;225:823–828. [DOI] [PubMed] [Google Scholar]
- 39.Topal U, Ediz B. Transthoracic needle biopsy: factors effecting risk of pneumothorax. Eur J Radiol. 2003;48:263–267. [DOI] [PubMed] [Google Scholar]
- 40.Ginsberg RJ, Rubinstein LV. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann Thorac Surg 1995;60:615–622; discussion 622–623. [DOI] [PubMed]
- 41.Noguchi M, Morikawa A, Kawasaki M, et al. Small adenocarcinoma of the lung. Histologic characteristics and prognosis. Cancer. 1995;75:2844–2852. [DOI] [PubMed] [Google Scholar]