

Abstract
Objective.
To determine the role of household composition as an independent risk factor for fatal inflicted injuries among young children and describe perpetrator characteristics.
Design, Setting, and Population.
A population-based, case-control study of all children <5 years of age who died in Missouri between January 1, 1992, and December 31, 1999. Missouri Child Fatality Review Program data were analyzed. Cases all involved children with injuries inflicted by a parent or caregiver. Two age-matched controls per case child were selected randomly from children who died of natural causes.
Main Outcome Measure.
Inflicted-injury death. Household composition of case and control children was compared by using multivariate logistic regression. We hypothesized that children residing in households with adults unrelated to them are at higher risk of inflicted-injury death than children residing in households with 2 biological parents.
Results.
We identified 149 inflicted-injury deaths in our population during the 8-year study period. Children residing in households with unrelated adults were nearly 50 times as likely to die of inflicted injuries than children residing with 2 biological parents (adjusted odds ratio: 47.6; 95% confidence interval: 10.4–218). Children in households with a single parent and no other adults in residence had no increased risk of inflicted-injury death (adjusted odds ratio: 0.9; 95% confidence interval: 0.6–1.9). Perpetrators were identified in 132 (88.6%) of the cases. The majority of known perpetrators were male (71.2%), and most were the child’s father (34.9%) or the boyfriend of the child’s mother (24.2%). In households with unrelated adults, most perpetrators (83.9%) were the unrelated adult household member, and only 2 (6.5%) perpetrators were the biological parent of the child.
Conclusions.
Young children who reside in households with unrelated adults are at exceptionally high risk for inflicted-injury death. Most perpetrators are male, and most are residents of the decedent child’s household at the time of injury.
Keywords: inflicted injury, child abuse, fatality, risk factors, case-control study
ABBREVIATIONS: CFRP, Child Fatality Review Program; SIDS, sudden infant death syndrome; OR, odds ratio; aOR, adjusted odds ratio; CI, confidence interval; TBI, traumatic brain injury
Inflicted injuries are the leading cause of injury death among infants1 and account for one third of injury deaths resulting from maltreatment among children under the age of 5 in Missouri.2 Almost all fatal inflicted injuries to young children are caused by adult caregivers and are therefore, by definition, physical child abuse.3
Using vital-records data makes it possible to conduct large, population-based studies to identify risk factors for fatal inflicted injuries. It is well documented, however, that studies based on vital records severely underestimate child maltreatment deaths, with 50% to 85% of child maltreatment deaths misclassified as resulting from other causes.3–7 In addition, vital-records data are typically limited to a small subset of maternal and child variables and provide no information on household composition, the perpetrators, or their relationship to the decedent child. This combination of pronounced misclassification and lack of risk-factor information in vital records severely limits the usefulness of these data for child-maltreatment research.1,8–10
Combining data from multiple sources, now a common practice in many state-based child-fatality-review programs, can greatly reduce the misclassification of maltreatment fatalities as resulting from other causes. In addition, compared with vital records, child-fatality-review programs often document detailed information about the cause and circumstances of death and record information on a wider variety of risk factors.5,7,11 We published a case-control study2 in Pediatrics in 2002 using the first 3 years of Missouri Child Fatality Review Program (CFRP) data (1992–1994). We reported that children residing in households with adults unrelated to them were 8 times as likely to die of maltreatment than children residing with only 2 biological parents and showed no increased risk of maltreatment death to children in households with a single parent and no other adult residents. The findings of this study were important, but the number of cases was too small to analyze household composition by maltreatment type with adequate statistical power or to explore perpetrator relationships. Maltreatment is a term that typically incorporates both child abuse and neglect outcomes. Analyses by specific type of maltreatment are critical to sort out distinct risk factors and possible etiologic differences. For example, several studies have noted different risk factors for physical abuse versus neglect,12–15 and several studies specifically noted differences in household composition by maltreatment type.2,16,17
The purpose of this study was to evaluate household composition as an independent risk factor for fatal inflicted injuries among young children. We analyzed 8 years of the Missouri CFRP data to test 2 hypotheses: (1) that children residing in households with adults unrelated to them are at higher risk of inflicted-injury death than children residing in households with 2 parents and no other adults; and (2) that children living with a single parent were at no greater risk of inflicted-injury death than children living with 2 parents as long as no other adults lived in the home. Secondary objectives included conducting a descriptive analysis of perpetrator characteristics including gender, relationship to decedent child, and whether the perpetrator was a member of the decedent’s household at the time of the child’s death.
METHODS
Study Population and Data Sources
All children less than age 5 who died in Missouri between January 1, 1992, and December 31, 1999, were eligible for the study. The primary source of data for this study was records from the Missouri CFRP. Mandated in 1991 and established January 1, 1992, the CFRP consists of multidisciplinary review teams in each of Missouri’s 114 counties and the city of St Louis. Team composition is mandated and includes the county prosecuting attorney, the county coroner or medical examiner, law enforcement, and representatives from child protective services, the juvenile court, public health, and emergency services. Each death of a child <18 years of age is reported to the county coroner or medical examiner, who then reviews the death with the chair of the county review team. When the cause, manner, or circumstances of the death meet any of ~20 criteria, the death is referred to the full multidisciplinary team for review. Review criteria include all injury deaths; unexpected, unexplained or suspicious deaths; deaths potentially related to malnutrition or delay in seeking medical care; and deaths in households with prior child protective services contacts. Deaths not meeting these criteria may be referred for review at the discretion of the chair. During the review, team members contribute knowledge of the circumstances of the death and information on prior contacts with the child or the child’s family. Unlike some child-fatality-review programs, reviews in Missouri are conducted within days or a few weeks of the child’s death. Standardized data forms are used to record information about the decedent and detailed circumstances surrounding the death. Information on household members and their relationship to the decedent child is collected on all child deaths even if the death does not meet the criteria for review by the full county team. In the case of inflicted injuries, information on perpetrator gender and the relationship of the perpetrator to the decedent child are also recorded. State-level program personnel compile the forms from each county and, by checking against death certificates, routinely monitor completion of the forms. They also conduct annual training sessions throughout the state to ensure accurate and consistent data-collection procedures by the local teams.
For this study, we obtained the completed CFRP data forms and computerized data files, as well as documentation of child abuse and neglect reports on all case and control children, from the Missouri Department of Social Services. Data from birth and death certificates were obtained from the Missouri Department of Health and Senior Services and linked to the CFRP data. The study protocol was exempted from review by the Health Sciences Institutional Review Board at the University of Missouri.
Procedures for Identification and Selection of Cases and Controls
We reviewed the CFRP forms of all children <5 years old who died of an injury or undetermined cause during the 8-year study period. We also reviewed other corroborating documents such as autopsy or police reports when available. Children were included as case children for this analysis when, after reviewing the available information describing the circumstances of death, we were able to determine that the injury resulting in death was inflicted by a parent or other adult caregiver.
Eligible controls were all children who died of natural causes during the same period. We included children whose deaths were a result of prematurity and congenital malformations if they lived >7 days. We excluded children who lived ≤7 days based on our assumption that these children likely never left the hospital and therefore were never members of a household in the same manner as cases. We excluded sudden infant death syndrome (SIDS) deaths because of the potential for misclassification of inflicted-injury cases as SIDS. Although we believe that the Missouri child-fatality-review process results in few such misclassifications, not all SIDS deaths in our data meet the diagnostic criteria of complete autopsy, death-scene investigation, and review of clinical history. We generated a list of all eligible control children. Using a random-number generator, we selected 2 control children per case child, frequency matched by age (month of age for infants, year of age for children aged 1–4). If household information was missing, the selected control was discarded and the next randomly selected eligible control child with complete household information was chosen.
Exposure and Outcome Measures
The main outcome measure was inflicted-injury death at the hands of a parent or other adult caregiver. The primary exposure variable was composition of the decedent child’s household. We classified household composition into 5 mutually exclusive categories based on the relationship of adults in the household to the decedent child. When developing the classification scheme, we attempted to distinguish between biological relationships (eg, biological parent, other relative), nonbiological relationships that included a “parental role” (eg, stepparent or foster parent), and neither biological nor parental relationships. The categories were (1) households with 2 biological parents and no other adult residents, (2) households with 1 biological parent and no other adult residents, (3) households with 1 or 2 biological parents and another adult relative(s), (4) households with stepparents or foster parents, and (5) households with 1 or 2 biological parents and another unrelated adult(s).
Households with a combination of related and unrelated adults in residence were classified based on the following hierarchy. If an unrelated adult resided in the household, the household was classified in the unrelated-adult category regardless of the other household members. Households with a stepparent or foster parent in addition to another relative were classified in the stepparent or foster category.
In our first study using CFRP data,2 we classified households with adoptive parent(s) in the category with stepparents and foster parents; our rationale was that adoptive parents are in a parental role but unrelated to the child, like stepparents or foster parents. However, this categorization generated several passionate discussions during presentations of those study findings by people who felt that the adoptive parent’s motivation for becoming a parent is strong, making them more similar to biological parents than stepparents or foster parents. As a result, for this analysis we classified households with adoptive parents in the same way as biological-parent households.
Statistical Analysis
We assessed the distribution of all variables of interest and potential confounding variables by using univariate and bivariate methods. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated by using logistic regression. The OR provides an estimate of the risk of fatal inflicted injury associated with each household-composition category compared with the reference category, which was households with 2 biological parents and no other adults in residence. For the multivariate-regression analyses we imputed missing values for each variable to the low-risk category. For example, records missing information on maternal education were assigned a code reflecting maternal education as high school graduate. Imputation of missing variables allows use of all data for regression analyses, resulting in less-biased effect estimates.18 Assigning the low-risk category for each variable minimizes overestimation of risk. All statistical analyses were conducted by using SAS (SAS Institute, Inc, Cary, NC).19
We conducted multivariate logistic regression to assess confounding. Potential confounding variables were identified from these data and the literature. Potential confounders included child factors (black race, age), maternal factors (young maternal age, less than high school education, unmarried, late or no prenatal care, and Medicaid eligibility at child’s birth), and household factors (presence of siblings under the age of 5 in the household, prior child protective services report on this child or other household residents). We considered a variable a confounder if its inclusion in a regression model with household composition resulted in a change in the effect estimate of ≥10%.20 Once all confounders were identified, we used multivariate logistic regression to calculate the adjusted OR (aOR) of the relationship between household composition and fatal inflicted injury while controlling for the identified confounding variables.
RESULTS
Of the 901 children <5 years old who died as a result of an injury or undetermined cause during the 8-year study period, we identified 149 deaths caused by inflicted injuries (case children) and randomly selected 298 control children frequency matched on age. The majority of the children were male (56%), white (52%), and infants <1 year old (58%). Seventy-five percent of the children were <2 years old and 90% were <3 years old at the time of death. When compared with controls, children who died as a result of inflicted injuries were more likely to be black; born to young, unmarried, Medicaid-eligible mothers with less than a high school education and late or no prenatal care; reside in households with young siblings; and have a prior report to child protective services (Table 1).
TABLE 1.
Distribution of Select Child, Maternal, and Household Variables for Inflicted Injury: Case and Control Children, 1992–1999
| Variable | Cases (N = 149), n (%) | Controls (N = 298), n (%) | OR (95% CI) |
|---|---|---|---|
| Child variables | |||
| Gender | |||
| Male | 84 (56) | 146 (49) | 1.3 (0.9–2.0) |
| Female | 65 (44) | 152 (51) | Reference |
| Race | |||
| Black/other | 72 (48) | 85 (29) | 2.3 (1.6–3.5) |
| White | 77 (52) | 213 (71) | Reference |
| Maternal variables | |||
| Age at child’s birth | |||
| <25 y | 95 (64) | 122 (41) | 2.8 (1.8–4.4) |
| ≥25 y | 39 (26) | 141 (47) | Reference |
| Missing (50) | 15 (10) | 35 (12) | |
| Education at child’s birth | |||
| <High school | 55 (37) | 64 (21) | 2.1 (1.4–3.3) |
| High school graduate | 79 (53) | 195 (65) | Reference |
| Missing (54) | 15 (10) | 39 (14) | |
| Marital status at child’s birth | |||
| Not married | 94 (63) | 114 (38) | 3.2 (2.1–5.1) |
| Married | 38 (26) | 149 (50) | Reference |
| Missing (52) | 17 (11) | 35 (12) | |
| Month of first prenatal visit | |||
| None, 5th–9th mo | 33 (22) | 34 (11) | 2.2 (1.3–3.8) |
| 1st–4th mo | 98 (66) | 224 (75) | Reference |
| Missing (58) | 18 (12) | 40 (13) | |
| Medicaid eligible at child’s birth | |||
| Eligible | 90 (60) | 124 (41) | 3.0 (1.8–4.8) |
| Not eligible | 32 (22) | 133 (45) | Reference |
| Missing (68) | 27 (18) | 41 (14) | |
| Household variables | |||
| Siblings <5 y old | |||
| Yes | 72 (48) | 60 (20) | 3.5 (2.3–5.4) |
| No | 75 (50) | 219 (74) | Reference |
| Missing (21) | 2 (1) | 19 (6) | |
| Prior report of abuse/neglect on anyone in household | |||
| Yes | 70 (47) | 38 (13) | 4.4 (2.7–7.3) |
| No | 60 (40) | 144 (48) | Reference |
| Missing (135) | 19 (13) | 116 (39) | |
| Prior report of abuse/neglect on decedent | |||
| Yes | 22 (15) | 7 (2) | 7.2 (3.0–17.3) |
| No | 127 (85) | 291 (98) | Reference |
Seventy-three percent of the injuries were inflicted by shaking or striking the child (108 of 149). Of these, 69 children died as a result of abusive head trauma, and 39 suffered abdominal, thoracic, or multiple trauma from their beating. Of the remaining 41 children, 20 (13.4%) were suffocated, 8 (5.4%) were killed with firearms, and 13 (8.7%) were injured in a variety of other ways (burns, poisonings, etc).
Household Composition and Risk of Fatal Inflicted Injuries
Only 37% of case children, compared with 64% of control children, lived in households with 2 biological parents and no other adult residents (Fig 1). Case children were more likely than control children to live in households with adult relatives, stepparents or foster parents, and unrelated adults; in fact, 35% of case children versus 6% of control children lived in these 3 household types. There were only 2 households with adoptive parents in these data (both were control households), so it is not likely that our classification of adoptive parents with biological parents influenced our final results.
Fig 1.
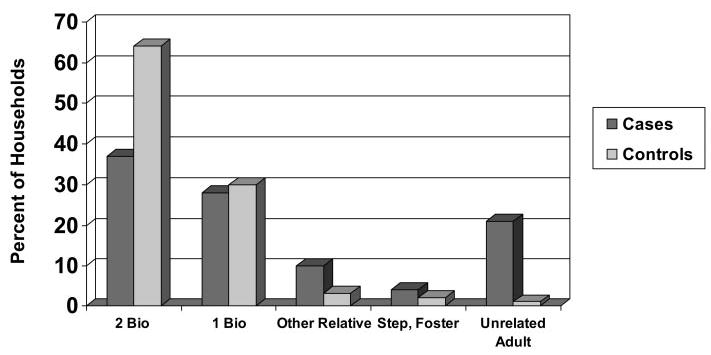
Household composition by case-control status: 1992–1999. Bio, biological parent.
Children living in households with an adult unrelated to them were almost 50 times as likely to die of an inflicted injury than children living in households with 2 biological parents, after controlling for confounding factors (aOR: 47.6; 95% CI: 10.4–218) (Table 2). Eighty-two percent (27 of 33) of those in the unrelated-adult household category consisted of the decedent child’s biological mother and her boyfriend. Three households had the mother and another adult, 1 had the father and his girlfriend, and 2 households in this category had no biological parents in residence.
TABLE 2.
Multivariate Logistic-Regression Results for the Association Between Household Composition and Risk of Inflicted-Injury Death: Missouri, 1992–1999
| Household-Composition Category | Case Households (N = 149), n (%) | Control Households (N = 298), n (%) | aOR (95% CI)* |
|---|---|---|---|
| Two biological parents only | 55 (37) | 192 (64) | Reference |
| One biological parent only | 42 (28) | 89 (30) | 0.9 (0.6–1.9) |
| Other relative present | 15 (10) | 9 (3) | 2.3 (0.8–6.2) |
| Stepparent or foster parent | 6 (4) | 6 (2) | 1.1 (0.3–4.7) |
| Unrelated adult(s) | 31 (21) | 2 (1) | 47.6 (10.4–218) |
Regression analyses were adjusted for child’s race, mother’s age at child’s birth, late or no prenatal care, siblings <5 years old, and prior child abuse or neglect reports on child and household.
There was a twofold increase in risk to children in households with other adult relatives in residence, but this result did not reach statistical significance. No increased risk was found for children in households with stepparents or foster parents, and it is important to note that there was no increased risk of fatal inflicted injury in households with a single parent and no other adults.
Perpetrator Characteristics
Perpetrators were identified in 132 (88.6%) of the cases. The majority of known perpetrators were male (94 of 132 [71.2%]). Forty-six (34.9%) were the child’s father, and 32 (24.2%) were the boyfriend of the child’s mother. The child’s mother was the perpetrator for 26 (19.7%) cases (Table 3). Most known perpetrators lived with the decedent child at the time of injury (96 of 132 [72.7%]). Perpetrators who killed children residing with a single parent only were least likely to be a resident of the household (ie, the perpetrator was not the parent) (Table 4). In contrast, all known perpetrators who killed children residing in stepparent/foster households were members of the household (most commonly the stepparent or foster parent); most perpetrators who killed children from households with unrelated adults (28 of 31 [90.3%]) were members of the household, and 74.2% (23 of 31) were the boyfriends of the decedent’s mother. Most perpetrators killing children in 2-parent households (76.4%) were also residents.
TABLE 3.
Gender of Perpetrator and Relationship to Decedent Child
| Relationship | n (%) |
|---|---|
| Males | 94 (71.2) |
| Biological father | 46 (34.9) |
| Boyfriend of mother | 32 (24.2) |
| Other male relative | 6 (4.5) |
| Male nonrelative | 4 (3.0) |
| Stepfather | 3 (2.3) |
| Male babysitter | 2 (1.5) |
| Foster father | 1 (0.8) |
| Females | 34 (25.8) |
| Biological mother | 26 (19.7) |
| Female babysitter | 4 (3.0) |
| Other female relative | 2 (1.5) |
| Girlfriend of father | 1 (0.8) |
| Female, nonrelative | 1 (0.8) |
| Gender unknown | 4 (3.0) |
| Babysitter | 3 (2.3) |
| Nonrelative | 1 (0.8) |
| Total (known perpetrator) | 132 (100) |
TABLE 4.
Identification of the Perpetrator as a Member of the Decedent Child’s Household According to Household-Composition Category
| Was Perpetrator Member of Decedent’s Household?
|
|||
|---|---|---|---|
| Household-Composition Category | Yes n (%) | No n (%) | Unknown n (%) |
| Two biological parents only | 42 (76.4) | 9 (16.4) | 4 (7.3) |
| One biological parent only | 15 (35.7) | 21 (50.0) | 6 (14.3) |
| Other relative | 6 (40.0) | 4 (26.7) | 5 (33.3) |
| Stepparent or foster parent | 5 (83.3) | 0 (0.0) | 1 (16.7) |
| Unrelated adult residents | 28 (90.3) | 2 (6.5) | 1 (3.2) |
| Total | 96 (64.4) | 36 (24.2) | 17 (11.4) |
A perpetrator was not identified by the CFRP team for 17 cases. In most of these situations, the police investigation was ongoing at the time that the CFRP forms were completed. The most common scenarios resulting in an unidentified perpetrator involved the presence of 2 adults at the time of injury, neither of which was providing information to the police, or there was a delay in seeking treatment and the person responsible for the care of the child when the injury was inflicted had not been identified.
DISCUSSION
In this population-based case-control study using 8 years of child-fatality-review data, we found that children <5 years old who live in households with adults unrelated to them have a risk of inflicted-injury death that is almost 50 times the risk to children residing in households with 2 biological parents. More than 80% of these households with unrelated adults consisted of the child’s mother and her boyfriend, and in 74% of these households (23 of 31) the mother’s boyfriend was the perpetrator of the abuse.
Single-parent families have repeatedly been associated with increased risk of child maltreatment.16,21–27 The findings of this study identify a key distinction in single-parent households: those with a single parent alone and those with a single parent and other adults. We found no increase in risk of inflicted-injury death in households with a single parent and no other adults. We found a twofold increase in households with other adult relatives in residence (not statistically significant) and a nearly 50-fold increase in households with unrelated adults, usually the boyfriend of the decedent child’s mother. To our knowledge, the present study is the first analytic study of inflicted injuries among young children to show that it is the presence of adults (usually male) in the household who are unrelated to the child victim that accounts for the increased risk of fatal maltreatment in single-parent households, not single parenthood per se.
A recently published study of traumatic brain injury (TBI) in young children exemplifies this omission. Keenan et al28 analyzed several household-composition characteristics in their study comparing young children with an inflicted TBI to those with a noninflicted TBI. They reported a twofold increase in risk of inflicted TBI among children living in households with extended family, comparable to our category of household with other relatives present in which we report a similar increase in risk. They reported a protective effect of households in which the child’s biological father was a resident in the home (OR: 0.5; 95% CI: 0.2–0.9). When we examined our current data comparing households with a biological father to those without, we found a similar protective effect of having the biological father residing in the home (OR: 0.4; 95% CI: 0.3–0.06). Our study confirms the findings by Keenan et al. However, their report did not include some of the most important risk factors and relationships associated with fatal inflicted injuries in young children: the presence of unrelated adults in the household, the relationship of the perpetrator to the decedent child, and perpetrator residence in the decedent child’s household.
Early studies of physical child abuse most often identified the child’s mother as the perpetrator of abuse.29,30 In 1986, Bergman et al31 examined trends in severe and fatal inflicted injuries to children in the period 1981–1983 compared with 1971–1973 in Seattle, Washington. They documented a greater proportion of severe and fatal injuries inflicted by known male perpetrators, including a greater proportion of boyfriends of the child’s mother, over the 10-year period. The authors point out that it was not possible to determine if the increase in the proportion of male perpetrators was real or related to social changes that took place during the study period. A greater social acceptance of couples living together without being married, more women entering the workforce, and men spending more time caring for children occurred in this 10-year interval.
More recent studies have confirmed that a greater proportion of men are identified as the perpetrator of inflicted injuries to children.3,32,33 Starling et al33 identified perpetrators of both fatal and nonfatal abusive head trauma over a 12-year period (1982–1994) at the Children’s Hospital of Denver and reported that 68.5% were male. For fatal abusive head trauma only, men were perpetrators in 74.2% of the cases, providing support for the Bergman et al findings that males were responsible for more severe injuries. Starling et al also examined the relationship of the perpetrator to the child for fatal and nonfatal cases combined and reported that 37.0% of perpetrators were the child’s father, 20.5% were the boyfriend of the child’s mother, 3.1% were stepfathers, and 12.6% were the child’s mother. In a study of child abuse homicide cases from 1985 to 1994 among North Carolina residents, Herman-Giddens et al3 reported that 65.5% of perpetrators were male, 29.6% were the child’s father, 18.2% were the mother’s boyfriend, 3.9% were stepfathers, and 30.0% were the child’s mother.
Our findings on perpetrator gender and relationship to the child victim are similar to those reported by Starling et al and Herman-Giddens et al except for the higher proportion of perpetrators identified as the child’s mother by Herman-Giddens et al (30.0%) compared with the present study (19.7%), which may be explained partially by their focus on child homicides. Fatal inflicted injuries by caregivers (physical abuse) are not always identified as homicides.5 Fatal inflicted injuries in the first week of life (neonaticide) are more often perpetrated by mothers and may be more likely to be recorded as homicides than fatal child abuse after the neonatal period.1,34,35
Starling et al33 speculated that male caregivers are more dangerous then female caregivers. Our data offer support for this hypothesis and identify households in which a young child resides with his or her mother and her boyfriend as dramatically higher risk. In these high-risk households, the boyfriend was typically responsible for caring for the child at the time of the fatal-injury event and was the perpetrator of abuse. At the same time, it is important to note that although the relative risk is greater in households with unrelated adults, the most common male perpetrator of fatal inflicted injury was the child’s biological father; nearly equal numbers of children were killed by their biological fathers as by other related and unrelated males, combined. For all household-composition categories, >70% of known perpetrators in our study were male, and >70% of known perpetrators lived with the decedent child.
Our findings have important implications for educational strategies to prevent fatalities caused by inflicted injuries and for child care policy. Educational campaigns designed to prevent “shaken-infant syndrome” (also referred to as abusive head trauma) are most likely to reach mothers of young infants. However, Starling et al33 and Ricci et al32 have shown that few mothers are perpetrators of abusive head trauma, and in the present study, mothers were perpetrators for just 20% of all inflicted injuries. A broader message that includes training on early childhood development as well as methods for identifying safe and appropriate child care should ideally be provided to all likely caregivers of infants and young children. This and other prevention strategies should particularly target biological fathers and other male caregivers, if possible. Furthermore, programs that provide prenatal and early childhood home visitation by nurses can reduce child abuse and neglect on the part of low-income, unmarried mothers. Although these programs were not developed explicitly to address fatal inflicted injuries, they effectively reduce many risk factors for fatal abuse and should be given high priority when considering broad-based child abuse and neglect–prevention programs in high-risk populations (low-income, unmarried mothers).36 Finally, with “welfare-to-work” policies forcing more mothers of young children into the workforce, policies and the financial resources to ensure high-quality day care for low-income mothers could significantly reduce the exposure of young children to male caregivers and therefore inflicted injuries.
The limitations of this study include a lack of information on some of the known risk factors for child physical abuse including parental substance abuse, domestic violence, history of abuse as a child, and depression. We also did not have information on the trigger (if any) of the abuse incident, which is important information when identifying potential prevention strategies. The imprecision of the effect estimate for risk of fatal maltreatment in households with unrelated adults (aOR: 47.6), as evidenced by the wide 95% CI (10–218), is a limitation. The relatively small number of children residing in these households and the number of covariates in the final logistic-regression model, relative to the number of study subjects, may have contributed to the imprecision of this estimate.
We believe the household data on the CFRP forms are quite accurate; however, external validation studies have not been conducted, and the forms may contain inaccuracies. The probability of misclassification resulting from data inaccuracies would likely be the same for both cases and controls and would bias the results toward the null value (underestimate the true effect).
This study has numerous strengths. It is a population-based analytic study comparing children who died as a result of inflicted injuries to natural-cause deaths. The comprehensive and standardized CFRP data provide detailed information on household members and their relationship to the decedent child at the time of death for all child deaths. This enabled us to classify children by household composition, evaluate the association between household composition and fatal inflicted injury, and ultimately tease out the fact that it is primarily the presence of unrelated adult males that leads to the striking increase in risk for fatal inflicted injuries among children in single-parent households. Although the finite classification of household composition is a study strength, there are no comparable statewide data available for all children. The US Census Bureau only classifies household structure for families with children into 2-parent (including stepparent, foster, adoptive) and 1-parent (regardless of other adults in residence) households, so it is not possible to determine the proportion of households in the state with only biological parents versus parents and some combination of other related and unrelated adult residents. Based on census data for Missouri, ~30% of children under the age of 18 live in single-parent households (nationally, this proportion is 28%) and 70% live in 2-parent households. Collapsing our study data into 2 household categories (single parents and 2 parents), we have 59% single-parent and 41% 2-parent households for case children and 34% single-parent and 66% 2-parent households for controls. The control group more closely resembles the statewide distribution. This is noteworthy, because the goal in selecting controls is that they represent the background frequency of exposure in the population free of the outcome of interest (in this study, fatal inflicted injury).
The availability of in-depth information on the circumstances leading to the fatal injury in the CFRP data, including identification of the perpetrator of inflicted injuries, is an additional strength. Use of this detailed information in injury circumstances ensured accurate classification of cases and controls for this study, permitted identification of injury mechanisms, and made it possible for us to avoid the underreporting of child abuse deaths and misclassification of infant and child homicides that has hampered most prior research on fatal child abuse.
Use of a subset of maltreatment-related fatal injuries, those inflicted by a caregiver, is another strength of this study. In our 2002 study of household composition and fatal child maltreatment using the first 3 years of CFPR data, we reported an aOR for fatal maltreatment in households with unrelated adults of 8.8 (95% CI: 3.6–21.5).2 However, the number of cases was too small to analyze the data by maltreatment type (inflicted injuries versus those related to inadequate supervision or failure to protect from known hazards). We conducted this study, using 5 additional years of data, to evaluate household risk factors by maltreatment type. Based on the aOR of 47.6 in this subset, the risk caused by inflicted injuries in households with unrelated adults is likely much higher than risk caused by other maltreatment-related injuries. Although our subset analysis of other maltreatment-related injuries over the 8-year period is not yet published, the preliminary findings are consistent with this conclusion. Furthermore, these results are consistent with other studies that have noted different risk factors and household composition for physical abuse versus neglect.12–17
CONCLUSIONS
We found that young children who reside in households with an unrelated adult are at nearly 50-fold risk of suffering a fatal inflicted injury, compared with children residing with 2 biological parents. The majority of perpetrators were male members of the decedent child’s household. Comprehensive CFRPs with systematic data collection such as the program in Missouri provide unique opportunities for research and offer important insights for injury prevention. Educational programs, policies, and resources directed toward providing young children with safe, protective environments including quality day care for single, working mothers should be considered important strategies for preventing inflicted-injury deaths among young children.
Acknowledgments
This study was funded in part by National Institute for Child Health and Human Development grant 5K08HD01377.
We are grateful to the Missouri Department of Health and Senior Services and Department of Social Services for providing data for this research. We are particularly grateful to Gus Kolilis and his staff at the State Technical Assistance Team for patiently responding to numerous requests for additional information and unfailing support for this research. We also thank Darla Horman, MA, for diligent data management and Drs Daniel Vinson and Mary Overpeck for helpful reviews of an earlier version of this manuscript.
Footnotes
No conflict of interest declared.
References
- 1.Overpeck MD, Brenner RA, Trumble AC, Trifiletti LB, Berendes HW. Risk factors for infant homicide in the United States. N Engl J Med. 1998;339:1211–1216. doi: 10.1056/NEJM199810223391706. [DOI] [PubMed] [Google Scholar]
- 2.Stiffman MN, Schnitzer PG, Adam P, Kruse RL, Ewigman BG. Household composition and risk of fatal child maltreatment. Pediatrics. 2002;109:615–621. doi: 10.1542/peds.109.4.615. [DOI] [PubMed] [Google Scholar]
- 3.Herman-Giddens ME, Brown G, Verbiest S, et al. Underascertainment of child abuse mortality in the United States. JAMA. 1999;282:463–467. doi: 10.1001/jama.282.5.463. [DOI] [PubMed] [Google Scholar]
- 4.Herman-Giddens ME. Underrecoding of child abuse and neglect fatalities in North Carolina. N C Med J. 1991;52:634–639. [PubMed] [Google Scholar]
- 5.Ewigman B, Kivlahan C, Land G. The Missouri child fatality study: underreporting of maltreatment fatalities among children younger than five years of age, 1983 through 1986. Pediatrics. 1993;91:330–337. [PubMed] [Google Scholar]
- 6.McClain PW, Sacks JJ, Froehlke RG, Ewigman BG. Estimates of fatal child abuse and neglect, United States, 1979 through 1988. Pediatrics. 1993;91:338–343. [PubMed] [Google Scholar]
- 7.Crume TL, DiGuiseppi C, Byers T, Sirotnak AP, Garrett CJ. Underascertainment of child maltreatment fatalities by death certificates, 1990–1998. . Pediatrics. 2002;110(2) doi: 10.1542/peds.110.2.e18. Available at: www.pediatrics.org/cgi/content/full/110/2/e18. [DOI] [PubMed] [Google Scholar]
- 8.Overpeck MD, Trumble AC, Berendes HW, Brenner RA. Risk factors for infant homicide. N Engl J Med. 1999;340:895–896. doi: 10.1056/NEJM199810223391706. [DOI] [PubMed] [Google Scholar]
- 9.West S. Risk factors for infant homicide [letter] N Engl J Med. 1999;340:895. [PubMed] [Google Scholar]
- 10.Wissow LS. Infanticide. N Engl J Med. 1998;339:1239–1241. doi: 10.1056/NEJM199810223391710. [DOI] [PubMed] [Google Scholar]
- 11.Schloesser P, Pierpont J, Poertner J. Active surveillance of child abuse fatalities. Child Abuse Negl. 1992;16:3–10. doi: 10.1016/0145-2134(92)90003-a. [DOI] [PubMed] [Google Scholar]
- 12.Martin MJ, Walters J. Familial correlates of selected types of child abuse and neglect. J Marriage Fam. 1982;44:267–276. [Google Scholar]
- 13.Dubowitz H, Hampton RL, Bithoney WG, Newberger EH. Inflicted and noninflicted injuries: differences in child and familial characteristics. Am J Orthopsychiatry. 1987;57:525–535. doi: 10.1111/j.1939-0025.1987.tb03568.x. [DOI] [PubMed] [Google Scholar]
- 14.Zuravin SJ. Unplanned childbearing and family size: their relationship to child neglect and abuse. Fam Plann Perspect. 1991;23:155–161. [PubMed] [Google Scholar]
- 15.Chaffin M, Kelleher K, Hollenberg J. Onset of physical abuse and neglect: psychiatric, substance abuse, and social risk factors from prospective community data. Child Abuse Negl. 1996;20:191–203. doi: 10.1016/s0145-2134(95)00144-1. [DOI] [PubMed] [Google Scholar]
- 16.Wilson M, Daly M, Weghorst SJ. Household composition and the risk of child abuse and neglect. J Biosoc Sci. 1980;12:333–340. doi: 10.1017/s0021932000012876. [DOI] [PubMed] [Google Scholar]
- 17.Creighton SJ. An epidemiological study of abused children and their families in the United Kingdom between 1977 and 1982. Child Abuse Negl. 1985;9:441–448. doi: 10.1016/0145-2134(85)90052-3. [DOI] [PubMed] [Google Scholar]
- 18.Harrell FE, Jr, Lee KL, Mark DB. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med. 1996;15:361–387. doi: 10.1002/(SICI)1097-0258(19960229)15:4<361::AID-SIM168>3.0.CO;2-4. [DOI] [PubMed] [Google Scholar]
- 19.SAS [computer program]. Version 8.0. Cary, NC: SAS Institute, Inc; 1999
- 20.Rothman KJ, Greenland S. Modern Epidemiology Philadelphia, PA: Lippincott-Raven; 1998
- 21.Showers J, Apolo J, Thomas J, Beavers S. Fatal child abuse: a two-decade review. Pediatr Emerg Care. 1985;1:66–70. [PubMed] [Google Scholar]
- 22.Malkin CM, Lamb ME. Child maltreatment: a test of sociobiological theory. J Comp Fam Stud. 1994;25:121–133. [Google Scholar]
- 23.Daly M, Wilson M. Child abuse and other risks of not living with both parents. Ethol Sociobiol. 1985;6:197–210. [Google Scholar]
- 24.Wilson M, Daly M. Risk of maltreatment of children living with step-parents. In: Gelles RJ, Lancaster JB, eds. Child Abuse and Neglect: Biosocial Dimensions New York, NY: Aldine De Gruyter; 1987:215–232
- 25.Baldwin JA, Oliver JE. Epidemiology and family characteristics of severely-abused children. Br J Prev Soc Med. 1975;29:205–221. doi: 10.1136/jech.29.4.205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Smith SM, Hanson R, Noble S. Social aspects of the battered baby syndrome. Br J Psychiatry. 1974;125:568–582. doi: 10.1192/bjp.125.6.568. [DOI] [PubMed] [Google Scholar]
- 27.Ebbin AJ, Gollub MH, Stein AM, Wilson MG. Battered child syndrome at the Los Angeles County General Hospital. Am J Dis Child. 1969;118:660–667. doi: 10.1001/archpedi.1969.02100040662025. [DOI] [PubMed] [Google Scholar]
- 28.Keenan HT, Runyan DK, Marshall SW, Nocera MA, Merten DF, Sinal SH. A population-based study of inflicted traumatic brain injury in young children. JAMA. 2003;290:621–626. doi: 10.1001/jama.290.5.621. [DOI] [PubMed] [Google Scholar]
- 29.Kaplun D, Reich R. The murdered child and his killers. Am J Psychiatry. 1976;133:809–813. doi: 10.1176/ajp.133.7.809. [DOI] [PubMed] [Google Scholar]
- 30.Gil DG. Incidence of child abuse and demographic characteristics of persons involved. In: Helfer RE, Kempe CH, eds. The Battered Child Chicago, IL: University of Chicago Press; 1968:19–40
- 31.Bergman AB, Larsen RM, Mueller BA. Changing spectrum of serious child abuse. Pediatrics. 1986;77:113–116. [PubMed] [Google Scholar]
- 32.Ricci L, Giantris A, Merriam P, Hodge S, Doyle T. Abusive head trauma in Maine infants: medical, child protective, and law enforcement analysis. Child Abuse Negl. 2003;27:271–283. doi: 10.1016/s0145-2134(03)00006-1. [DOI] [PubMed] [Google Scholar]
- 33.Starling SP, Holden JR, Jenny C. Abusive head trauma: the relationship of perpetrators to their victims. Pediatrics. 1995;95:259–262. [PubMed] [Google Scholar]
- 34.Jason J, Gilliland JC, Tyler CW., Jr Homicide as a cause of pediatric mortality in the United States. Pediatrics. 1983;72:191–197. [PubMed] [Google Scholar]
- 35.Herman-Giddens ME, Smith JB, Mittal M, Carlson M, Butts JD. Newborns killed or left to die by a parent: a population-based study. JAMA. 2003;289:1425–1429. doi: 10.1001/jama.289.11.1425. [DOI] [PubMed] [Google Scholar]
- 36.Olds DL, Eckenrode J, Henderson CR, Jr, et al. Long-term effects of home visitation on maternal life course and child abuse and neglect. Fifteen-year follow-up of a randomized trial. JAMA. 1997;278:637–643. [PubMed] [Google Scholar]