

Abstract
Objective
To examine the relative impact of four service quality dimensions on outpatient satisfaction and to test the invariance of the structural relationships between the service quality dimensions and satisfaction across three patient groups of varying numbers of prior visits to the same hospital as outpatients.
Data Sources/Study Setting
Survey of 557 outpatients using a self-administered questionnaire over a 10-day period at a general hospital in Sungnam, South Korea.
Data Collection
Patients answered questions related to two main constructs, patient satisfaction and health care service quality. The health care service quality measures (30 items) were developed based on the results of three focus group interviews and the SERVQUAL scale, while satisfaction (3 items) was measured using a previously validated scale.
Study Design
Confirmatory factor analysis was used to assess the construct validity of the service quality scale by testing convergent and divergent validity. A structural equation model specifying the four service quality dimensions as exogenous variables and patient satisfaction as an endogenous variable was estimated to assess the relative impact of each of the service quality dimensions on satisfaction. This was followed by a multigroup LISREL analysis that tested the invariance of structural coefficients across three groups with different frequencies of outpatient visits to the hospital.
Principal Findings
Findings support the causal relationship between service quality and satisfaction in the context of the South Korean health care environment. The four service quality dimensions showed varying patterns of impact on patient satisfaction across the three different outpatient groups.
Conclusion
The hospital management needs to be aware of the relative importance of each of the service quality dimensions in satisfaction formation of outpatients, which varies across different hospital utilization groups, and use this in strategic considerations.
Keywords: Outpatient satisfaction, service quality, visit frequency pattern, measurement validation
The health care system in the United States has recently experienced tremendous change. For the first time, providers are facing decreased funding, increased competition, and the maturation of the entire industry (Emanuel and Dubler 1995). To survive in this harsh environment, providers must learn how to cost-effectively satisfy the needs and desires of their patients. Consequently, the culture is shifting from emphasizing the efficacy and effectiveness of care outcomes to adapting services in response to patient needs (Donabedian 1996; Williams 1994).
In this new culture, providers and policymakers are increasingly using patient satisfaction measures to assess the performance of health care organizations (Hibbard and Jewett 1996; Zaslavsky et al. 2000). Patient satisfaction is important because it leads to a higher rate of patient retention and customer loyalty (Nelson et al. 1992) and influences the rates of patient compliance with physician advice (Calnan 1988; Roter Hall and Katz 1987). A good deal of research has explored a variety of health care service quality dimensions that may influence patient satisfaction, such as continuity of care, physician expertise, the concern shown by the physician and other medical staff, and physical facilities (Fletcher et al. 1983; Ware Davies-Avery and Stewart 1978; Ware Snyder and Wright 1977). Findings suggest that patients as customers are not homogeneous in what they expect from care providers (Reidenbach and Sandifer-Smallwood 1990), and that different patient subgroups (e.g., old versus young and chronic versus acute) may place different degrees of importance on the various quality dimensions that in turn influence patient satisfaction (Fletcher et al. 1983; Lytle and Mokwa 1992).
Past research on patient satisfaction has also found a linkage between satisfaction and hospital utilization. While the majority of past findings supported a positive relationship (Ware, Davies-Avery, and Stewart 1978), several studies presented evidence for an inverse relationship between satisfaction and the frequency of outpatient visits (Linn, Linn and Stein 1982; Pascoe and Attkinsson 1983; West 1976). Given the prevailing view in the consumer behavior literature that satisfaction positively affects loyalty (Nelson et al. 1992), these conflicting findings in patient behavior warrant further research to better ascertain the linkage between satisfaction and utilization. Many researchers (e.g., Oliver 1977; Pascoe 1983) viewed patient satisfaction as an outcome of the process in which patients assess the actual performance of the health care service against their expectations. This process is dynamic. As patients gain experience, or as their medical condition changes during the treatment process, patients may modify their expectations. It is also likely that their evaluation criteria or the priority placed on the salient service quality dimensions may evolve from the day they first visit the hospital.
As an extension of the past research on the relationship between service quality and patient satisfaction, this study investigated the impact of hospital visit frequency on the relative importance of health care service dimensions in satisfaction formation as outpatients' utilization increased at the same hospital. This investigation was based on the data collected in South Korea where patients have substantial freedom when choosing their medical providers. Therefore, this study further affords an opportunity for a cross-cultural examination of some of the existing findings in patient satisfaction.
Theoretical Background
Satisfaction and Service Quality
Although there seems to be a consensus in the literature that satisfaction and service quality are unique constructs, distinctions in their definitions have not always been made clear (Tomiuk 2000). An important source of confounding between these two constructs has been the use of the expectancy disconfirmation model in defining both concepts conceptually and operationally (Grönroos 1982; Oliver 1993 Oliver 1997; Parasuraman Zeithaml and Berry 1985 Parasuraman Zeithaml and Berry 1994; Rust and Oliver 1994). In an attempt to provide clarity to the distinction between these two constructs, two different types of standards have been proposed—one reflecting a desired state and the other an ideal state (Oliver 1993). Boulding et al. (1993) proposed that the ideal expectation (or “should”) be used as the referent in the expectancy disconfirmation involving service quality and the desirable expectation (or “will”) as a referent in the case of satisfaction.
Others proposed a distinction that involves a more fundamental clarification of the conceptual domains of these constructs. Oliver (1981) defined satisfaction as “the summary psychological state resulting when the emotion surrounding disconfirmed expectations is coupled with consumer's prior feelings about the consumption experience” (p. 27). This definition suggests that satisfaction is a consequence of, or a reaction to, expectancy disconfirmation and the resulting outcome is an affective one. In the health care service context, the affective status of satisfaction was also evident in Pascoe's (1983) definition in which satisfaction was referred to as “patients’ emotional reaction to salient aspects of the context, process, and result of their experience” (p. 189).
There appears to be greater accord in the literature that service quality, on the other hand, is a cognitive construct (e.g., Oliver 1997; Brady and Robertson 2001). Parasuraman, Zeithaml, and Berry (1988), who developed the widely used SERVQUAL scale, defined it as a judgment or evaluation relating to the superiority of the service, assuming that consumers apply a mental calculus to reach an evaluation. According to Rust and Oliver (1994), the evaluation of service quality results from specific attributes or cues related to the service, while satisfaction involves a wider range of determinants, including quality judgments, needs, and perceptions of equity.
The lack of clarity in the definitions of service quality and satisfaction is further linked to the ongoing controversy surrounding the causal order of service quality and satisfaction (Bitner 1990; Bolton and Drew 1991). This debate over which comes first has many similarities to the cognition–emotion debate (Tomiuk 2000). Distinguishing between service quality as a cognitive construct and satisfaction as an affective construct suggests a causal order that positions service quality as an antecedent to satisfaction. This is consistent with the attitude theoretical framework proposed by Fishbein and Ajzen (1975) and refined further by Bagozzi (1992). Although not absolute, much evidence has been documented for the service quality to satisfaction link in recent consumer satisfaction studies including those in the area of health care marketing (Brady and Robertson 2001; Gotlieb, Grewal and Brown 1994; Rust and Oliver 1994; Andaleeb 2001).
Multidimensionality of Service Quality
Quality assessments of a service are not unidimensional. Patients are known to use various aspects of medical care to evaluate the quality of services received (Hall and Doran 1988; Pascoe 1983). The literature on service quality delineates two rather distinct facets of the construct: (a) a technical dimension (i.e., the core service provided) and (b) a process dimension (i.e., how the service is provided) (Grönroos 1983).
Traditionally, the quality of medical care has been described as its ability to increase the probability of desired patient outcomes and decrease the probability of undesired outcomes (Donabedian 1988). This approach implies that care quality can be measured by the extent to which patients' physiological functions have improved as a consequence of receiving medical care services. Although this outcome-based quality assessment seems to be relatively concrete, cautions have been raised (Donabedian 1966). Specifically, it is problematic to decide who evaluates the quality of the outcome, what features of outcomes should be measured, and when the assessment takes place.
Furthermore, past studies (e.g., Fitzpatrick and Hopkins 1983; Newcome 1997) indicate that patients cannot properly evaluate the outcome of health care services and the technical competence of practitioners, since they often lack sufficient expertise and skill to make such judgments. As a consequence, patients have a tendency to infer the level of technical quality based on nontechnical aspects, such as care providers' compassion and empathy, responsiveness, and coordination of care among individual health care personnel (Donabedian 1988: Ettinger 1998). Thus, the process-related factors of service take on special significance for health care consumers.
Korean Health Care Delivery System
Under the new National Health Insurance system (NHI) which covers all Koreans, medical service facilities in South Korea are categorized into three tiers based on numbers of beds and degree of specialization: first tier (0–30 beds), second tier (31–700 beds), and third tier (more than 700 beds, and university hospitals) (Choi, Kim, and Lee 1998). Korean patients are allowed to visit any first- or second-tier facility without a medical referral. They may choose any general practitioner, or any specialist who works at a first- or second-tier facility. However, in order to get medical service from one of the third-tier hospitals, which account for less than 4 percent of the total medical facilities, a patient is required to have a referral.
A major difference in the health care delivery system between the United States and South Korea relates to the latitude patients have in choosing a specialist. In the United States, the majority of health care costs are paid by either private insurers or by the government. The kind of insurance held by patients puts constraints on what type of medical services they can get and on who provides them. In contrast, the NHI system in Korea allows patients substantial freedom in service provider selection. Also, Korean patients typically are served by hospital-based physicians regardless of the severity of their illness, whereas patients in the United States typically only visit hospitals if they are quite ill.
Methodology
Sample
The study was conducted at a general hospital with 430 beds located in Sungnam, a satellite city of Seoul, which is the capital of South Korea. This hospital is one of 16,610 medical facilities located within a 40-mile radius of Sungnam. Over a 10-day period, data collection took place in the area where outpatients wait for medication after being examined by physicians. According to Jee (2000), 83.9 percent of hospital outpatients in Korea receive a prescription from their physicians and get the medication from the hospital. Thus, our sampling frame covered most of the outpatients for the data collection period. A total of 800 outpatients were personally asked to participate in the survey by filling out a confidential self-administered questionnaire that took about 10 minutes to complete. In all, 557 patients answered the questionnaire containing questions about their assessment of the hospital service they received and demographic information. A decision was subsequently made to limit the sample to adults who ranged in age from 18 to 65. Patients receiving psychological services were not included in the final sample. A total of 537 usable questionnaires were used for the final data analysis.
In the final sample, 68.9 percent were female, almost all (97.2 percent) had at least a high school education, and the respondents were on average 33 years of age. To test the match between the demographic profiles of our sample and the outpatient population of the hospital, the proportions within each of the three demographic variables in the sample were compared with those of the outpatient population for the previous year provided by the hospital administration. The goodness-of-fit between the sample and the population proportions was tested for gender, age, and education using the χ2 tests. The gender composition in our sample was 68.9 percent male and 31.1 percent female as compared with 65.8 percent male and 34.2 percent female in the entire outpatient population. The proportions of sample respondents belonging to the age <30, 30≤age <40, 40≤age <50, and age≥50 categories were 40.8 percent, 40 percent, 14 percent, and 5.2 percent as compared with 43.6 percent, 38.2 percent, 12.2 percent, and 6 percent respectively in the outpatient population. For education, the sample proportions with a less than high school, high school, part or all college, and post-college education were 2.8 percent, 32.2 percent, 55.6 percent, and 9.4 percent respectively whereas for the outpatient population, the proportions were 2 percent, 34.5 percent, 57.9 percent, and 5.6 percent in the same order. It turned out that none of the three χ2-test results was significant, which suggests that our sample was not systematically biased.
Measures
The measurement task in this study required developing a multidimensional service quality measurement scale and a patient satisfaction scale. Especially for the measurement of service quality, it has been recommended that measurement items be developed that are unique to each specific service situation (Babakus and Mangold 1992; Dabholkar Thrope and Rentz 1996). The service quality scale was developed based on focus group interviews conducted with three different groups of adult outpatients to generate insights into how Korean health care users viewed the health care services they were receiving and the aspects of health care service they felt were important. Two investigators examined transcripts from the interviews without injecting prior conceptions of salient health care service dimensions. Transcript contents were reduced to chunks, each relating to the perceived importance of a particular health care service dimension. Then, these chunks were categorized into different dimensional categories by each investigator independently. Discrepancies between the two examiners were resolved after discussion. The results of this content analysis indicated that Korean outpatients were largely concerned with four dimensions when assessing medical service quality: the convenience of the care process, physician's concern for the patient, nonphysicians' concern, and tangibles. These dimensions have showed strong resemblance to the process-related factors identified by Grönroos (1983). Thirty items tapping these dimensions were subsequently developed based on the interviewees' comments and the SERVQUAL scale items (Parasuraman, Zeithaml, and Berry 1985). All items used seven-point Likert scales (1=strongly disagree; 7=strongly agree).
The second construct, patient satisfaction, was measured using three items: (1) “How satisfied were you with the treatment you received in the hospital?” (2) “How satisfied were you with your decision to use the hospital?” and (3) “How satisfied would you be if you visit again and receive the same treatment?” All three used seven-point scales (1=very dissatisfied; 7=very satisfied). The first two items were similar to those used by Ware and Hays (1988) and Reidenbach and Sandifer-Smallwood (1990).
Data Analysis and Results
Data analysis was conducted in three phases. The first phase involved a measurement analysis (i.e., purification and confirmation) of the key measures used in this study, namely, those for service quality and patient satisfaction. In the second phase, a structural equation model specifying relationships between patient satisfaction as an endogenous construct and the service quality dimensions as exogenous constructs was estimated to investigate the relative importance of each of the service quality dimensions. In the final stage, an examination was made on the (in)variance of the structural relationships across three groups that were divided according to the number of outpatient visits to the hospital that respondents had made at the time of the survey.
Measurement Analysis
The assessment of measurement properties (reliability and validity) and the item purification for the initial service quality scale with 30 items were carried out in an iterative procedure (Bohrnstedt 1983; Kim and Lee 1997). The item purification process resulted in 19 reliable items that conformed to the hypothesized four-dimensional factor structure (see Figure 1 for the actual items) with Cronbach's α values ranging from .80 to .94.
Figure 1.
Measurement Model
Note:
ξ1: Physician's concern (Cronbach's α=.94)
X1: The physician was polite.
X2: The physician adequately explained my condition, examination results, and treatment process.
X3: The physician allowed me to ask many questions, enough to clarify everything.
X4: The physician paid enough consideration to my concerns for deciding medical procedure.
X5: The physician made me feel comfortable.
ξ2: Nonphysicians' concern (Cronbach's α=.88)
X6: The nurses were friendly.
X7: The nurses explained the medication process well.
X8: Care providers seemed to try to help me as much as they could.
X9: Care providers truly cared for me.
X10: There was a good coordination among the care providers.
ξ3: Convenience of care process (Cronbach's α=.80)
X11: The procedure to get the lab test was convenient.
X12: The lab test was done in a prompt way.
X13: The payment procedure was quick and simple.
X14: The process for setting up the appointment was simple and easy.
X15: I did not have to wait long for the medical examination from the physician.
ξ4: Tangibles (Cronbach's α=.86)
X16: The waiting areas for medication and for the doctor's office were pleasant.
X17: It was easy to use the amenities (public telephone, cafeteria, etc.) in the hospital.
X18: The hospital seemed to be equipped with the latest equipment.
X19: It was easy to find care facilities (lab, doctor's office).
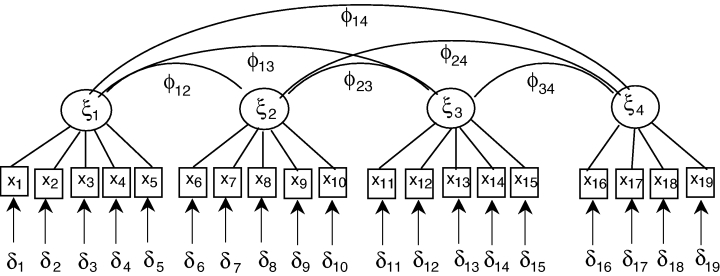
In the next stage, confirmatory factor analysis (CFA) using LISREL VIII (Jöreskog and Sörbom 1993) was conducted to test the four-factor measurement model based on the final 19 service quality items. For this measurement model, the overall model fit as indicated by the χ2 statistic (χ2=534.2, df =146, p <.00) was unsatisfactory. However, the χ2 test is very sensitive to sample size. Given the relatively large size of our sample (n =537), our attention was focused on incremental fit measures, the comparative fit index (CFI) and the normed fit index (NFI), which explain the practical significance of the variance explained by the model and is less sensitive to sample size effects (Bagozzi, Yi, and Phillips 1991; Bentler 1990). For the measurement model, the CFI and NFI values were .94 and .92 respectively, indicating that the model's fit was satisfactory.
The demonstration of construct validity for a scale requires evidence of convergent validity and discriminant validity (Campbell and Fiske 1959). In the CFA, convergent validity is assessed based on the significance and magnitude of factor loadings computed for indicators (or measurement items) of each construct in the model (Bagozzi, Yi, and Phillips 1991; Kim and Lee 1997). The size of factor loadings ranged between .64 and .94, and all of them were significant (p <.05; the range of t-values: 10.61 to 21.14). In addition, the extent of convergent validity can be examined based on the variance in each indicator explained by its corresponding construct, which is referred to as the “trait variance ()” (Bagozzi, Yi, and Phillips 1991). In our case, the average trait variances were: 49 percent for “tangibles”; 77 percent for “physician's concern”; 63 percent for “convenience of care process”; and 62 percent for “nonphysicians' concern.” Since an average trait variance greater than 50 percent is regarded to be strong evidence of convergent validity (Baggozi and Yi 1991), the above trait variance magnitudes demonstrated a quite satisfactory level of convergent validity for the four-dimensional service quality scale.
Discriminant validity among the four dimensional measures of health care service quality was examined by performing a chi-square difference test between a model where all the factor correlations were fixed at 1.0 and the unconstrained model. The unconstrained model showed a significantly better fit compared to the constrained model. This finding indicates that the four service quality dimensions were distinct from each other. In addition, the 95 percent confidence intervals were computed for the 6 factor correlations (range: .54 to .74; mean: .64). None of these intervals contained unity. This provides further evidence that our scale was competent in discriminating among the service quality dimensions.
In sum, results of the measurement analysis showed evidence of convergent validity for the four-dimensional service quality scale. Furthermore, the four dimensions, although correlated, were sufficiently distinct. These results allowed us to construct additive, equally weighted indices for each of four service dimensions. These dimensional indices of service quality were later incorporated into structural modeling as exogenous variables. With respect to the three-item patient satisfaction scale, since the items have been used in past studies (Reidenbach and Sandifer-Smallwood 1990; Ware and Hays 1988), only their reliability was examined (Cronbach's α=.94).
Structural Equation Model
The second phase of analysis involved an investigation into the structural relationships between four dimensions of service quality and patient satisfaction. The structural model consisted of four service quality dimensions as exogenous variables and patient satisfaction as an endogenous construct with three indicators. It is a form of a Multiple Indicators and Multiple Causes (MIMIC) model (Jöreskog and Sörbom 1993).
When estimated for the total sample using LISREL VIII (Jöreskog and Sörbom 1993), the MIMIC model showed an excellent fit (χ2=13.15, df =8, p =0.11; CFI=1.00; NFI=1.00). Based on the squared multiple correlation, 60 percent of the total variation in patient satisfaction was explained by the four service quality dimensions. The estimated structural coefficients (see Table 1) show that “nonphysicians' concern” emerged as the most important service quality dimension affecting patient satisfaction (γ12=.37, p <.01), followed by “convenience of care process” (γ13=.30, p <.01) and “physician's concern” (γ11=.16, p <.01). On the other hand, the “tangibles” dimension (γ14=.06) did not reach the 5 percent significance level (p =.06). A notable finding here was that nonphysicians' concern and convenience played a greater role than physician concern in patient satisfaction formation.
Table 1.
Results of MIMIC Model for Total Sample and Subsamples Divided Based on Visit Frequencies
| Total Sample | Group 1: (Visit=1) | Group 2: (2≤Visits≤6) | Group 3: (Visits≥7) | |||||
|---|---|---|---|---|---|---|---|---|
| Structural Path | Estimate* | T-value | Estimate* | T-value | Estimate* | T-value | Estimate* | T-value |
| Physician Concern | 0.16 | 3.54 | 0.1 | 0.84 | 0.09 | 1.14 | 0.32 | 5.05 |
| →Satisfaction | ||||||||
| Nonphysicans' Concern | 0.37 | 7.94 | 0.36 | 3.62 | 0.44 | 5.92 | 0.26 | 3.71 |
| →Satisfaction | ||||||||
| Convenience | 0.3 | 7.06 | 0.37 | 3.5 | 0.31 | 4.53 | 0.31 | 4.89 |
| →Satisfaction | ||||||||
| Tangible | 0.06 | 1.57 | −0.13 | −1.27 | 0.07 | 1.11 | 0.14 | 2.37 |
| →Satisfaction | ||||||||
Parameter Estimates are standardized.
Next, the total sample was divided into three groups based on the number of times respondents visited the hospital in the past 12 months as outpatients. After classifying the first-time visitors as the first group, the remaining outpatients were divided into two groups using their median number of visits. The resulting three groups were: first-time visitors (n =133); those with two to six visits (n =219); and those with more than six visits (n =184). Before estimating the structural coefficients and comparing them across different subgroups, patient satisfaction for each group was calculated. The average satisfaction level was 5.25 for the first group, 5.04 for the second, and 5.30 for the third (1=very dissatisfied; 7=very satisfied). A one-way ANOVA was conducted to test the equality of the three-group mean satisfaction values. Results showed that the mean levels were significantly different (F(2,533)=3.08, p <0.05). According to post hoc comparison tests, the second group was significantly less satisfied than the third group, while the third group's satisfaction level was not different from the first group.
In the subsequent stage, for each of the three patient subgroups, the MIMIC model was tested and the causal paths between the four dimensions and satisfaction were estimated. For the first group (visit=1), the overall model fit was satisfactory (χ2=27.91, df =8, p <.00; CFI=.96; NFI=.95; R2=.43). The estimated structural coefficients for the first group (see Table 1) showed that “convenience” had the largest impact on patient satisfaction (γ13=.37, p <.01), closely followed by “nonphysicians' concern” (γ12=.36, p <.01). Surprisingly, “physician's concern” was not significant in satisfaction formation (γ11=.10, p =.20). The “tangibles” dimension also was not significant (γ14=−.13, p =.11).
The MIMIC model for the second group (2≤visits≤6) produced substantially better fit indications (χ2=7.21, df =8, p =0.51; CFI=1.00; NFI=.99; R2=.61). The estimated structural coefficients (in Table 1) indicated that, as was for the first group, “convenience” and “nonphysicians' concern” significantly affected patient satisfaction (p <.01). Both “physician's concern” and “tangibles” were not significant determinants of patient satisfaction (p =.13 for both).
Finally, the MIMIC model for the third group (visits > 6) also showed satisfactory fit indications (χ2=32.00, df =8, p <0.00; CFI=1.00; NFI=.99; R2=.32). The pattern of structural relationships found for this group was markedly different from those found for the two previous groups. For these patients, satisfaction formation was significantly impacted by all four service quality dimensions. Most notably, “physician's concern,” which had been a nonsignificant factor thus far, emerged as the most important determinant of patient satisfaction (γ11=.32, p <.01), followed by “convenience” (γ13=.31, p <.01), “nonphysicians' concern” (γ12=.26, p <.01), and “tangibles” (γ14=.14, p <.01).
Three-Group Invariance Analysis
The pattern of the structural relationships across the three MIMIC models suggested that the relative importance of each of the four service quality dimensions in patients' satisfaction formation was likely to vary depending upon the number of visits outpatients have made to the hospital. A formal test based on the multigroup LISREL analysis (Jöreskog and Sörbom 1993) was conducted to examine the invariance of structural paths across the three groups. The test involved a simultaneous estimation of the three MIMIC models (for the three groups) with no restrictions on the elements in the Γ matrix (i.e., structural coefficients), followed by another simultaneous estimation of the three MIMIC models with equality constraints (Γgroup 1=Γgroup 2=Γgroup 3). The fit of a multigroup model (also called a “stacked model”) is calculated as a weighted average of the fits obtained for each of the groups individually. Since the stacked model with the invariance constraint is nested in the stacked model without this constraint, the difference in the χ2 statistics corresponding to the fit of the two models provides a basis for determining the appropriateness of the equality constraints.
For the three-group model without constraints, the estimated χ2 statistic was 67.12 (df =24, p <.01), while the three-group model with equality constraints yielded a χ2 statistic of 84.92 (df =32, p <.01). The χ2 difference value of 27.80 for 8 degrees of freedom was significant (p <.01). Therefore, the equality constraints have caused a significantly worsening of the fit of the unconstrained multigroup model. This suggests that the pattern of structural relationships between the service quality dimensions and patient satisfaction was not the same across the three groups. The rejection of the invariant structural coefficients across the three groups called for an examination of pairwise between-group differences. Toward this end, a round of between-two-group invariance tests (involving between groups 1 and 2, 1 and 3, and, 2 and 3) were conducted.
For the invariance test involving groups 1 and 2, the χ2 statistic difference between the two-group stacked model without the invariance constraints (χ2=35.12, df =16) and the two-group model with the invariance constraints (i.e., Γgroup1=Γgroup2) (χ2=39.22, df =20) was 4.10 with 4 degrees of freedom, which was not statistically significant (p =.39). This suggests that the impact of each of the four service quality dimensions on satisfaction did not vary between the first-time visitors to the hospital and those who visited the hospital two to six times in the past 12 months. On the other hand, the two-group invariance test involving the second group and the third group showed a χ2 difference value of 9.56 for 4 degrees of freedom, which was significant (p <.05). The final invariance test conducted for the first group and the third group similarly resulted in a significant χ2 difference value (χ2=13.57, df =4, p <.01). Hence, the overall inequality in the pattern of the structural relationships was likely caused by the difference between the third group with seven or more visits and the rest with less than seven visits to the hospital.
Discussion
In this study, a health care service quality measure initially containing 30 items was purified and subjected to confirmatory factor analysis to verify its construct validity. The functional relationships between the four service quality dimensions and patient satisfaction were tested in the subsequent stage. The hypothesized relationships were derived from the multiattribute attitude model framework, that is, cognition (health care service quality) to affect (patient satisfaction). Results of the data analysis strongly supported the hypothesized model in the context of the South Korean medical delivery system, and provided evidence that the service quality to satisfaction link is robust across different cultures and health care systems.
More revealing insights on the relative importance of service quality dimensions in satisfaction formation were obtained from the analyses of subgroups of patients with varying numbers of previous outpatient visits to the same hospital. First of all, results showed that patient satisfaction itself varied with the number of outpatient visits. While this was also observed in past studies (Linn, Linn, and Stein 1982; Pascoe and Attkisson 1983; Ware, Davies-Avery, and Stewart 1978), the variation seen in this study was not linear as previously reported. Instead, the first group (visit=1) and the third group (visits > 6) were more satisfied than the second group (2≤visits≤6). One possible explanation is that the nature of the medical care that some patients were receiving may have temporarily restrained them from easily moving to a new medical facility. For example, when a patient has reoccurring dizzy spells, he or she needs to visit the same medical facilities until a diagnosis is reached after a series of tests. This type of outpatient would have had to use the same facilities regardless of their feelings of dissatisfaction with the services provided to them. However, if patients return to the same hospital repeatedly over time (such as the third group in our study), it may be because they were satisfied. In the U.S. health care system, Pascoe (1983) similarly suggested that when patients (such as those using VA medical facilities or a public health center) cannot easily switch to other medical facilities, they may need to continue using the same provider at least for a while despite their less than satisfactory experience.
A key finding of the three-group analyses relates to the (in)stability of the structural relationships between service quality dimensions and patient satisfaction. For both the first and second group, patient satisfaction was largely determined not by “physician's concern” and “tangibles,” but by “nonphysician care providers' concern” and “convenience.” However, the estimated structural pattern for the third group (visits > 6) showed a significant departure. Specifically, these outpatients weighed all four service quality dimensions significantly in their satisfaction formation. Notably, “physician's concern” emerged as the most important determinant of satisfaction for this group. Past studies on the doctor–patient relationship (Calnan 1988; West 1976; Williams and Calnan 1991) have suggested that the relationship between the patient and the physician is unlike that of a buyer and seller. Rather, it is a “fiduciary” one in which patients want to maintain respect and faith in their physicians (Parsons 1951). However, West (1976) found that during the early visits, patients were more passive and less critical about how they were treated. But as the level of interaction increased with their physicians, patients gained more information and became more critical about the professional practices (Calnan 1988).
Therefore, it appears that as patients become more informed about the health care service and their physician through frequent visits, they are able to incorporate a wider range of factors into their assessment of overall service quality. Perhaps a more notable finding of this study was that as the frequency of visits increased, patients in this study were weighing “physician's care,” a core health care service dimension, as the most important determinant of their satisfaction. This contrasts to the attention paid to the more auxiliary or peripheral dimensions of health care service by patients in their early visits to the hospital.
A similar tendency has been found in studies on how consumers evaluate the quality of products. Consumers evaluate products based on intrinsic and extrinsic dimensions. Intrinsic dimensions include tangible and core attributes directly related to quality, while extrinsic dimensions are image variables such as price, brand name, and country of origin. It has been found that as consumers become more educated and experienced, they tend to engage in comprehensive processing of all available dimensions, while novice consumers are more likely to rely on extrinsic attributes for the product evaluation (Maheswaran 1994; Maheswaran and Sternthal 1990).
Our study indicated that auxiliary service quality dimensions such as “nonphysicians' care” and “convenience” were important for satisfaction formation of outpatients during their early visits to health institutions. Since patient satisfaction influences patient retention rate and effectiveness of medical care by affecting patient compliance with physician advice, findings of this study should be useful for health care institutions and public health care policymakers who are striving for efficient allocation of the limited resources available to achieve patient satisfaction. Improvement of these two service quality dimensions can be achieved primarily through education and system redesign at relatively low cost. Medical personnel need to be educated on how to make various aspects of care delivery convenient for patients and on the importance of the care process that exhibits staff concern and empathy for patient well being, particularly new patients. It should be stressed, however, that the perceived quality of the doctor–patient relationship may, in the long run, emerge as the most significant factor in bringing about patient satisfaction and loyalty. Therefore, our findings suggest that everyone in the organization needs to become part of an institution-wide commitment to patient satisfaction, because quality management is not the monopoly of top administrators. In addition, this study revealed that the relation between outpatient satisfaction and frequency of visits is not positively linear, but rather U-shaped. Hospital management should be aware that repeat visits to the hospital do not necessarily reflect patient loyalty resulting from patient satisfaction. It seems that policymakers and hospital management should look at the level of satisfaction with discretion. They should consider the patient's conditions and care situation when interpreting the satisfaction data for decision-making purposes.
A discussion of some limitations of this study is in order. The first involves the outpatient sample used in this study. Compared to inpatients that spend more time in the hospital, outpatients leaving the hospital after a brief visit may have limited experience with the hospital environment as well as with physician and nonphysician care providers. Therefore, the key dimensions that underlie the service quality impressions may differ between inpatients and outpatients. The single-site sample used in this study also represents a limitation to the generalizability of the findings. Different hospitals may have different systems of service delivery and physical atmospheres. Clearly, a type of cluster sample drawn from multiple hospitals would enhance the external validity of the study findings.
The next potential concern relates to the measurement scope of service quality, which was limited to the process aspects of services. The service quality dimensions used in this study were derived from focus group interviews, and technical outcome did not surface as an important health care service quality criterion. This result, in a way, attests to the belief that patients lack sufficient medical knowledge to judge the technical quality of the medical service (Newcome 1997; Williams 1994). The relative importance of process dimensions of health care service was further demonstrated by the large amount of variance in the satisfaction measure that was accounted for by the four service quality dimensions (R2=.60 for the total sample MIMIC model). Nonetheless, the ultimate goal for patients is to restore or maintain their health. In many cases, patients may be able to judge how much they are helped by their physician to relieve pain and reduce functional limitations. It is also conceivable that patients with chronic illnesses may over time become relative experts in their illness and conditions, and therefore be able to assess certain technical aspects of the health care they have been receiving. In future studies, it may be desirable to develop and incorporate a health service quality scale that includes the outcome dimensions that lay people can properly evaluate. Considering that 40 percent of the variance in patient satisfaction was still left to be accounted for in the present study, a further inclusion of outcome dimensions may substantially add to the overall power of the service quality measure in explaining patient satisfaction.
A potentially significant pitfall of the focus group interview as an approach to eliciting salient service dimensions should also be noted here. According to Kano (1984, 1995), product/service characteristics can be classified into the categories of: (1) basic, (2) performance, and (3) excitement. Basic characteristics are those that the customers take for granted. If these are not present, customers will be highly dissatisfied. However, stronger performance on these attributes provides diminishing returns in terms of satisfaction (e.g., brakes in an automobile). Performance characteristics are directly correlated to customer satisfaction (e.g., gas mileage). Excitement characteristics, when provided, generate disproportionately high levels of customer satisfaction. These attributes are often unexpected and can fulfill latent customer needs (e.g., automobile seat warmer). Given these three types of product/service characteristics, focus groups are likely to be sensitive primarily to the performance attributes. The excitement attributes that result in customer delight and loyalty may not be easily identified through focus group interviews (Burns and Evans 2000). This should be recognized as a potential limitation in our focus group approach to finding key health care service dimensions. Consequently, one of the challenges for health care providers would be the identification and implementation of these excitement attributes in order to excel in this harsh competitive environment.
Since most past studies on satisfaction have been geographically concentrated in the United States and Western Europe, the findings of this study contribute to establishing the external validity of the functional relationship between service quality and patient satisfaction. Nonetheless, because the dimensional and item content of the service quality measure used in this study are not equivalent to those used in the past U.S. or European studies, a caution is clearly called for in making conclusions regarding the extent of similarity in the findings. While the fundamental linkage between service quality and satisfaction may endure across different cultures and health care systems, salient service quality dimensions and their relative importance in satisfaction formation may not. A rigorous test of equivalence in measures or in structural relationships is only possible when the study involves multinational samples of health care consumers. Also, as an extension of this study, we suggest that future studies focus on the delineation of how the functional relationships between the service quality dimensions and patient satisfaction vary across different types of care (e.g., primary versus specialty care, and internal medicine versus surgical).
References
- Andaleeb SS. Service Quality Perceptions and Patient Satisfaction A Study of Hospitals in a Developing Country. Social Science and Medicine. 2001;52(9):1359–70. doi: 10.1016/s0277-9536(00)00235-5. [DOI] [PubMed] [Google Scholar]
- Babakus E, Mangold WG. Adapting SERVQUAL Scale to Hospital Services An Empirical Investigation. Health Services Research. 1992;26(1):767–86. [PMC free article] [PubMed] [Google Scholar]
- Bagozzi RP. The Self Regulation of Attitudes, Intentions, and Behavior. Social Psychology Quarterly. 1992;55(4):178–204. [Google Scholar]
- Baggozi RP, Yi Y. Mutitrait-Multimethod Matrices in Consumer Research. Journal of Consumer Research. 1991;17(4):426–39. [Google Scholar]
- Bagozzi RP, Yi Y, Phillips LW. Assessing Construct Validity in Organization Research. Administrative Science Quarterly. 1991;36(3):421–58. [Google Scholar]
- Bentler PM. Comparative Fit Indexes in Structural Models. Psychological Bulletin. 1990;107(2):238–46. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- Bitner MJ. Evaluating Service Encounters Effects of Physical Surroundings and Employee Responses. Journal of Marketing. 1990;54(2):69–82. [Google Scholar]
- Bohrnstedt GW. Measurement. In: Rossi P, Wright J, Anderson A, editors. Handbook of Survey Research. New York: Academic Press; 1983. pp. 69–121. [Google Scholar]
- Bolton RN, Drew JH. A Multistage Model of Customers' Assessments of Service Quality and Value. Journal of Consumer Research. 1991;17:375–84. [Google Scholar]
- Boulding W, Kalra A, Staelin R, Zeithaml VA. A Dynamic Process Model of Service Quality From Expectation to Behavioral Intentions. Journal of Marketing Research. 1993;30(1):7–27. [Google Scholar]
- Brady MK, Robertson CJ. Searching for a Consensus on the Antecedent Role of Service Quality and Satisfaction An Exploratory Cross-Sectional Study. Journal of Business Research. 2001;51:53–60. [Google Scholar]
- Burns AD, Evans S. Insights into Customer Delight. In: Scrivener SAR, Ball LJ, Woodcock A, editors. Collaborative Design. London: Springer; 2000. [Google Scholar]
- Calnan M. Towards a Conceptual Framework of Lay Evaluation of Health Care. Social Science and Medicine. 1988;27(9):927–33. doi: 10.1016/0277-9536(88)90283-3. [DOI] [PubMed] [Google Scholar]
- Campbell DT, Fiske DW. Convergent and Discriminant Validation by the Multitrait-Multimethod Matrix. Psychological Bulletin. 1959;56(2):81–105. [PubMed] [Google Scholar]
- Choi E, Kim J, Lee W. Health Care Systems in Korea. Seoul: Korea Institute for Health and Social Affairs; 1998. [Google Scholar]
- Dabholkar PA, Thrope DI, Rentz JO. A Measure of Service Quality for Retail Stores Scale Development and Validation. Journal of the Academy of Marketing Science. 1996;24(1):3–16. [Google Scholar]
- Donabedian A. Evaluating the Quality of Medical Care. Milbank Memorial Fund Quarterly: Health and Society. 1966;44(3):166–203. [PubMed] [Google Scholar]
- Donabedian A. Quality Assessment and Assurance Unity of Purpose, Diversity of Means. Inquiry. 1988;25(1):175–92. [PubMed] [Google Scholar]
- Donabedian A. The Effectiveness of Quality Assurance. International Journal for Quality in Health Care. 1996;8(4):401–7. doi: 10.1093/intqhc/8.4.401. [DOI] [PubMed] [Google Scholar]
- Emanuel EJ, Dubler NN. Preserving the Physician–Patient Relationship in the Era of Managed Care. Journal of the American Medical Association. 1995;273(4):323–9. [PubMed] [Google Scholar]
- Ettinger WH., Jr Consumer-Perceived Value The Key to a Successful Business Strategy in the Healthcare Marketplace. Journal of the American Geriatrics Society. 1998;46(1):111–3. doi: 10.1111/j.1532-5415.1998.tb01024.x. [DOI] [PubMed] [Google Scholar]
- Fishbein M, Ajzen I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research. Reading, MA: Addison-Wesley; 1975. [Google Scholar]
- Fitzpatrick R, Hopkins A. A Problem in the Conceptual Framework of Patient Satisfaction Research An Empirical Exploration. Sociology of Health and Illness. 1983;5(3):297–311. doi: 10.1111/1467-9566.ep10491836. [DOI] [PubMed] [Google Scholar]
- Fletcher RH, O'Malley M, Earp JA, Littleton TA, Fletcher SW, Greganti MA, Davison RA, Taylor J. Patients' Priorities for Medical Care. Medical Care. 1983;21(2):234–42. doi: 10.1097/00005650-198302000-00010. [DOI] [PubMed] [Google Scholar]
- Gotlieb JB, Grewal D, Brown SW. Consumer Satisfaction and Perceived Quality Complementary or Divergent Constructs? Journal of Applied Psychology. 1994;79(6):875–85. [Google Scholar]
- Grönroos C. An Applied Services Marketing Theory. European Journal of Marketing. 1982;16(7):30–41. [Google Scholar]
- Grönroos C. Strategic Management and Marketing in the Service Sector. Boston: Marketing Science Institute; 1983. [Google Scholar]
- Hall JA, Doran MC. Meta-Analysis of Satisfaction with Medical Care Description of Research Domain and Analysis of Overall Satisfaction Levels. Social Science and Medicine. 1988;27(6):637–44. doi: 10.1016/0277-9536(88)90012-3. [DOI] [PubMed] [Google Scholar]
- Hibbard JH, Jewett JJ. What Type of Quality Information Do Consumers Want in a Health Care Report Card? Medical Research and Review. 1996;53(1):28–47. doi: 10.1177/107755879605300102. [DOI] [PubMed] [Google Scholar]
- Jee Y. Cost-Analysis of Mandatory Prescription in Korea. Seoul: Public Health Department, The Graduate School of Yonsei University; 2000. [Google Scholar]
- Jöreskog KG, Sörbom D. LISREL8 User's Reference Guide. Chicago: Scientific Software; 1993. [Google Scholar]
- Kano N. Upsizing Organisation by Attractive Quality Creation. In: Kanji GK, editor. Total Quality Management: Proceedings of the First World Congress. London: Chapman Hall; 1995. pp. 60–72. [Google Scholar]
- Kano N. Attractive Quality and Must-be Quality. Journal of the Japanese Society for Quality Control. 1984;14(2):39–48. [Google Scholar]
- Kim C, Lee H. Development of Family Triadic Measures for Children's Purchase Influence. Journal of Marketing Research. 1997;34(3):307–21. [Google Scholar]
- Linn MW, Linn BS, Stein SR. Satisfaction with Ambulatory Care and Compliance in Older Patients. Medical Care. 1982;20:606–14. doi: 10.1097/00005650-198206000-00006. [DOI] [PubMed] [Google Scholar]
- Lytle RS, Mokwa MP. Evaluating Health Care Quality The Moderating Role of Outcomes. Journal of Health Care Marketing. 1982;12(1):4–14. [PubMed] [Google Scholar]
- Maheswaran D. Country of Origin as a Stereotype Effects of Consumer Expertise and Attribute Strength on Product Evaluations. Journal of Consumer Research. 1994;21(2):354–65. [Google Scholar]
- Maheswaran D, Sternthal B. The Effects of Knowledge, Motivation, Type of Message on Ad Processing and Product Judgments. Journal of Consumer Research. 1990;17(1):66–73. [Google Scholar]
- Nelson E, Rust RT, Zahorik A, Rose RL, Batalden P, Siemanski B. Do Patient Perceptions of Quality Relate to Hospital Financial Performance? Journal of Healthcare Marketing. 1992;12(4):1–13. [PubMed] [Google Scholar]
- Newcome LN. Measuring of Trust in Health Care. Health Affair. 1997;16(1):50–1. doi: 10.1377/hlthaff.16.1.50. [DOI] [PubMed] [Google Scholar]
- Oliver RL. Effects of Expectation and Disconfirmation on Postexposure Product Evaluations An Alternative Interpretation. Journal of Applied Psychology. 1977;64(4):246–50. [Google Scholar]
- Oliver RL. Measurement and Evaluation of Satisfaction Process in Retail Settings. Journal of Retailing. 1981;57(3):25–48. [Google Scholar]
- Oliver RL. Cognitive, Affective, and Attribute Bases of the Satisfaction Response. Journal of Consumer Research. 1993;20(4):1–13. [Google Scholar]
- Oliver RL. Satisfaction: A Behavioral Perspective on the Consumer. Boston: Irwin-McGraw-Hill; 1997. [Google Scholar]
- Pascoe GC. Patient Satisfaction in Primary Health Care A Literature Review and Analysis. Evaluation and Program Planning. 1983;6(3/4):185–97. doi: 10.1016/0149-7189(83)90002-2. [DOI] [PubMed] [Google Scholar]
- Pascoe GC, Attkisson CC. The Evaluation Ranking Scale A New Methodology for Assessing Satisfaction. Evaluation and Program Planning. 1983;6(3/4):335–47. doi: 10.1016/0149-7189(83)90013-7. [DOI] [PubMed] [Google Scholar]
- Parasuraman A, Zeithaml V, Berry L. A Conceptual Model of Service Quality and Its Implications for Future Research. Journal of Marketing. 1985;49:41–50. [Google Scholar]
- Parasuraman A, Zeithaml V, Berry L. SERVQUAL A Multiple-Item Scale for Measuring Consumer Perceptions of Service Quality. Journal of Retailing. 1988;64(1):12–40. [Google Scholar]
- Parasuraman A, Zeithaml V, Berry L. Reassessment of Expectations as a Comparison Standard in Measuring Service Quality Implications for Future Research. Journal of Marketing. 1994;58(1):111–24. [Google Scholar]
- Parsons T. The Social System. London: Routledge & Kegan Paul; 1994. [Google Scholar]
- Reidenbach RE, Sandifer-Smallwood B. Exploring Perceptions of Hospital Operations by a Modified SERVQUAL Approach. Journal of Health Care Marketing. 1990;10(4):47–55. [PubMed] [Google Scholar]
- Roter DL, Hall JA, Katz NR. Relations between Physicians, Behaviors and Analogue Patients' Satisfaction, Recall, and Impressions. Medical Care. 1987;25(5):437–51. doi: 10.1097/00005650-198705000-00007. [DOI] [PubMed] [Google Scholar]
- Rust RT, Oliver RL. Service Quality Insights and Managerial Implications from the Frontier. In: Rust RT, Oliver RL, editors. Service Quality: New Directions in Theory and Practice. Thousand Oaks, CA: Sage; 1994. pp. 1–19. [Google Scholar]
- Tomiuk MA. 2000. The Impact of Service Providers' Emotional Displays on Service Evaluation: Evidence of Emotional Contagion. Ph.D. Dissertation. Montreal, Canada: Concordia University. [Google Scholar]
- Ware JE, Jr, Davies-Avery A, Stewart AL. The Measurement and Meaning of Patient Satisfaction A Review of the Recent Literature. Health and Medical Care Services Review. 1978;1:1–15. [PubMed] [Google Scholar]
- Ware JE, Jr, Hays RD. Methods for Measuring Patient Satisfaction with Specific Medical Encounters. Medical Care. 1988;26(4):393–402. doi: 10.1097/00005650-198804000-00008. [DOI] [PubMed] [Google Scholar]
- Ware JE, Jr, Snyder MK, Wright WR. Some Issues in the Measurement of Patient Satisfaction with Health Care Services. Santa Monica, CA: Rand; 1977. [Google Scholar]
- West P. The Physician and Management of Childhood Epilepsy. In: Wadsworth M, Robinson D, editors. Studies in Everyday Medical Life. London: Martin Robertson; 1976. pp. 13–31. [Google Scholar]
- Williams SJ. Patient Satisfaction A Valid Concept? Social Science and Medicine. 1994;38(4):509–16. doi: 10.1016/0277-9536(94)90247-x. [DOI] [PubMed] [Google Scholar]
- Williams SJ, Calnan M. Convergence and Divergence Assessing Criteria of Consumer Satisfaction across General Practice, Dental and Hospital Care Setting. Social Science and Medicine. 1991;33(6):707–16. doi: 10.1016/0277-9536(91)90025-8. [DOI] [PubMed] [Google Scholar]
- Zaslavsky AM, Beaulieu ND, Landon BE, Cleary PD. Dimensions of Consumer-Assessed Quality of Medicare Managed-Care Health Plans. Medical Care. 2000;38(2):162–74. doi: 10.1097/00005650-200002000-00006. [DOI] [PubMed] [Google Scholar]