

Abstract
Objective
To evaluate the effect of a publicly sponsored drug-free workplace program on reducing the risk of occupational injuries.
Data Sources
Workers' compensation claims data from the Washington State Department of Labor and Industries covering the period 1994 through 2000 and work-hours data reported by employers served as the data sources for the analysis.
Study Design
We used a pre–post design with a nonequivalent comparison group to assess the impact of the intervention on injury risk, measured in terms of differences in injury incidence rates. Two hundred and sixty-one companies that enrolled in the drug-free workplace program during the latter half of 1996 were compared with approximately 20,500 nonintervention companies. We tested autoregressive, integrated moving-average (ARIMA) models to assess the robustness of our findings.
Principal Findings
The drug-free workplace intervention was associated (p<.05) with a statistically significant decrease in injury rates for three industry groups: construction, manufacturing, and services. It was associated (p<.05) with a reduction in the incidence rate of more serious injuries involving four or more days of lost work time for two industry groups: construction and services. The ARIMA analysis supported these findings.
Conclusions
The drug-free workplace program we studied was associated with a selective, industry-specific preventive effect. The strongest evidence of an intervention effect was for the construction industry. Estimated net cost savings for this industry were positive though small in magnitude.
Keywords: Substance abuse prevention, workers' compensation, occupational injuries, drug-free workplace programs
Substance abuse remains one of the nation's most important public health problems resulting in significant morbidity and premature mortality (National Institute on Alcohol Abuse and Alcoholism and National Institute on Drug Abuse 1998;Office of National Drug Control Policy 2001). Current national data reported by the 2000 National Household Survey on Drug Abuse (NHSDA) indicate that 15.4 percent of persons aged 18 years and older used illicit drugs during the past year, while 8.8 percent were current (past month) users (Office of Applied Studies, Substance Abuse and Mental Health Services Administration 2002). Heavy drinking (drinking five or more drinks on the same occasion on each of five or more days in the past 30 days) was reported by 7.3 percent of the population. Persons aged 18 to 25 had the highest reported rates of current illicit drug use and heavy drinking, 15.9 percent and 12.8 percent, respectively.
Considerable attention has focused on substance abuse as a risk factor for occupational injuries and accidents (Alleyne, Stuart and Copes 1991;Lehman and Simpson 1992;National Research Council 1994;Gust and Walsh 1989). Widely publicized accidents in which drug or alcohol use was implicated, in particular, the aircraft crash on the carrier Nimitz, a passenger train crash in Chase, Maryland, involving the deaths of 16 people, and, more recently, the catastrophic oil spill in Alaska involving the Exxon Valdez tanker, heightened public concern about the role of substance abuse in workplace accidents. Studies have produced somewhat conflicting evidence regarding the risk gradient of alcohol and drug use for occupational injuries due, in part, to differences in research methods, measures, and study populations and settings. Some studies have failed to show a link between alcohol and drug use and occupational injuries or have shown only a weak link (Parish 1989;Hertz and Emmett 1986;Normand, Salyards and Mahoney 1990). Other studies have documented a clearer link, with the risk of occupational injury associated with substance use rising by 50 percent to 100 percent depending upon the substance used (alcohol, marijuana, other drugs) and the frequency and amount of use (Zwerling, Ryan and Orav 1990;Hingson, Lederman and Walsh 1985;Gutierrez-Fisac, Regidor and Ronda 1992;Pollock et al. 1998; Moll van Charante and Mulder 1990; Lewis and Cooper 1989). Beyond increasing the risk of occupational injuries, substance abuse has adverse effects on other workplace outcomes, including absenteeism, turnover, and disciplinary actions (Normand, Salyards and Mahoney 1990;Zwerling, Ryan and Orav 1990;Substance Abuse and Mental Health Services Administration 1999;Bush and Autry 2002).
In response to growing national concern over the problem of substance abuse and its effect on workplace safety and productivity, the federal government in 1986 established by executive order the Federal Drug-Free Work-place Program. This federal initiative defined a model drug-free workplace (DFW) program that included the following components (Bush and Autry 2002): (1) a written policy describing the employer's expectations about drug use and consequences of policy violations; (2) an employee assistance program (EAP) to provide confidential problem assessment, counseling, referral to treatment, and follow-up support after treatment; (3) supervisor training to orient supervisors to the employer's drug abuse policy, to define the supervisor's responsibility to refer employees when job performance deficits are noted, and to recognize and respond to employees with problems; (4) employee education to describe the signs and symptoms of drug abuse and its effects on performance and to explain the program; and (5) drug testing on a controlled and carefully monitored basis.
Following the federal initiative, private employers and public sector agencies adopted DFW programs. Reliable data on the use of DFW programs are unavailable, but surveys suggest that workplace substance abuse prevention activities, especially drug testing, are now used by more than one-half to two-thirds of major U.S. businesses (Bush and Autry 2002). Despite the importance attached to substance abuse prevention, little formal evaluation of DFW programs has been conducted. In fact, we could not identify any study in the peer-reviewed, scientific literature that systematically documented the impact of a DFW program, though many articles in trade publications provide conceptual support for the value of DFW programs. The lack of empirical understanding about the effect of DFW programs hinders the development of public policy as well as resource allocation for workplace substance abuse prevention.
This article presents the findings of an evaluation from Washington State conducted to determine the impact of a publicly sponsored DFW program on the occurrence of occupational injuries. Using claims data from a workers' compensation database, we examine changes in injury rates over a seven-year period, beginning in 1994, among workers of firms enrolled in the DFW program relative to workers in non-DFW comparison firms.
Methods
Program Setting
To address the problem of workplace substance abuse and to improve workplace safety, the Washington State legislature enacted the Washington Drug-Free Discount Act (2SSB 5516) in 1996 establishing the Washington Drug-Free Workplace (WDFW) Program. The law authorized the workers' compensation program to offer 5 percent discounts in workers' compensation premiums for up to three years for private employers who enrolled in the program. The maximum aggregate amount that could be offered through premium discounts was $5 million. The discount program was designed as a demonstration project. Thus, the law included a sunset provision that was to take effect January 1, 2001, unless subsequent legislation was enacted extending the program. Though legislation was introduced to extend the program, a divided state legislature did not pass it, and the program expired in 2001.
The federal drug-free workplace program, described earlier, served as a model for the WDFW Program. To participate in the WDFW Program, employers had to meet several program requirements. First, they had to develop a comprehensive formal written substance abuse policy outlining prohibitions and sanctions for drug and alcohol abuse, procedures for drug testing, use of employee assistance programs (EAP) for referral to treatment, and provisions to protect worker confidentiality. Second, the employer had to require and pay for preemployment, postaccident, and posttreatment drug testing (random drug testing was optional). Third, the employer had to select an EAP from an approved list of EAPs and had to agree to provide treatment for employees through that EAP. Employees violating the substance abuse policy could not be terminated if they agreed to receive treatment, abide by procedures for follow-up care, and have no subsequent violations. Fourth, the employer had to ensure that employees received an annual educational program on substance abuse. Finally, the employer had to ensure that all supervisors and managers received a minimum of two hours training regarding substance abuse, treatment referral, and drug testing.
Two state agencies, the Department of Labor and Industries (DLI) and the Division of Alcohol and Substance Abuse (DASA) within the Department of Social and Health Services, were responsible for administering the WDFW Program. The DLI operates the state workers' compensation program and provides workers' compensation insurance for two-thirds of the state's nonfederal workforce (by law, unless employers self-insure, they must purchase worker's compensation insurance through the DLI). The DLI was responsible for administering the premium discount; the DASA was responsible for reviewing applications to the program and for certifying program eligibility.
Design, Data, and Measures
This study has a pre–post design with a nonequivalent comparison group. We obtained the following data for this analysis from the DLI: (1) claims information on all reported injuries that occurred from January 1994 through October 2000, and (2) data on aggregate hours worked per quarter for the same period for each company insured through the DLI. The injury claim records contained administrative and medical information about each reported injury, including company identification, date of injury, age and sex of claimant, claim payment, and nature of injury. Data on hours worked are submitted to the DLI on a quarterly basis by each company insured for workers' compensation for the purpose of paying workers' compensation premiums. We used the work-hours data to estimate person-years of exposure (2,000 hours equals one person-year of exposure) in order to construct injury rates. Because the work-hours data are subject to detailed audit, they are known to be reliable and accurate.
For this analysis, we created a study cohort of companies using the following selection criteria. The company existed on January 1, 1994, and was still operating and insured through the DLI on Dec 31, 1999. This ensured that each company analyzed would have approximately two and a half years of baseline observation prior to the start of the program (October 1996) and three years of subsequent observation. We then divided these companies into an intervention cohort and a comparison cohort. The comparison cohort consisted of all (20,215) non-WDFW companies. The intervention cohort consisted of 261 companies that enrolled in the WDFW Program between July 1, 1996, and December 31, 1996. We grouped companies by two-digit Standard Industrial Classification (SIC) code into eight standard industry groups: (1) Agriculture, Forestry, and Fishing; (2) Mining; (3) Construction; (4) Manufacturing; (5) Transportation and Public Utilities; (6) Wholesale and Retail Trade; (7) Finance, Insurance, and Real Estate; and (8) Services. Some companies had subsidiaries that had SIC codes from more than one industry group. These companies were classified as “Multiple Codes.”
We constructed injury incidence rates by dividing the number of injury claims by the number of person-years, and report the rates as injuries per 100 person-years. Two different incidence rates were constructed: (1) an overall rate representing all reported injuries, and (2) a rate representing more serious time loss injuries, defined by the DLI as claims involving four or more days of lost work time.
Analytical Approach
We stratified our analysis by industry group to control for differences in background injury risk (e.g., construction workers have higher injury risk than accountants or retail sales clerks) and examined injury rates over three time periods: (1) a preintervention (Before) period representing 33 months beginning January 1994; (2) an intervention (During) period representing 36 months beginning October 1996; and (3) a postintervention (After) period representing 12 months beginning October 1999.
We calculated a “difference in injury incidence rate” (injuries per 100 person-years in intervention cohort minus injuries per 100 person-years in comparison cohort) for each time period and constructed 95 percent confidence intervals (CI) around these differences (Rothman 1986). The primary measure of program effect for this analysis is the change in the rate difference between the preintervention and intervention periods. For example, if the injury rates in the preintervention period for the intervention and comparison cohorts are, respectively, 27 injuries per 100 person-years and 22 injuries per 100 person-years, the injury rate difference would be 5 injuries per 100 person-years. If the injury rate for the intervention cohort declines to 22 injuries per 100 person-years and the corresponding rate for the comparison group decreases to 20 injuries per 100 person-years, the injury rate difference would change from 5 injuries per 100 person-years to 2 injuries per 100 person-years for a net reduction of 3 injuries per 100 person-years.
Whether the observed change in the injury rate difference is statistically significant is determined by examining the 95 percent confidence intervals associated with the rate differences. If these confidence intervals do not overlap, the change in the rate difference is statistically significant. By examining injury rate differences over time, the analysis, in effect, takes account of the general downward secular trend in occupational injuries that occurred in the United States during the latter half of the 1990s (Bureau of Labor Statistics 2002) and has the added advantage of generating information that is readily interpretable.
In addition, to assess the robustness of the findings based upon our confidence-interval analysis, we specified and tested autoregressive, integrated moving-average (ARIMA) models for those industry groups for which we report statistically significant changes in injury rate differences (Pindyck and Rubinfeld 1991). ARIMA models are useful for evaluation research when longitudinal data are being used to assess the existence of an intervention effect. Such data typically do not conform to the standard assumption regarding independence of observations. ARIMA models take account of this and also allow adjustment for other effects related to the longitudinal nature of the data, for example, secular trends. ARIMA models have been used to evaluate the effect of changes in speed limit laws on accident rates (Ledolter and Chan 1996), the effect of gun control laws on homicides and suicide rates (Loftin et al. 1991), and the impact of evaluation guidelines on lumbar-fusion surgery (Elam et al. 1997). The ARIMA procedure we used allowed us to control for an autoregressive component, random effects, a seasonal component, and a secular trend in injury rates. The time unit of analysis for this ARIMA procedure is the calendar quarter (n =28), with the dependent variable specified in terms of quarterly injury rate differences. The ARIMA model included an intervention dummy variable set equal to 1 for all quarters after October 1996 and 0 for quarters before that time. If the intervention dummy variable is a statistically significant component of the ARIMA model, an intervention effect is assumed to exist.
Results
Table 1 shows the distribution of companies within the cohorts and the number of person-years used to calculate the injury rates shown in Tables 2 and 3. A person-year represents one full-time employee working for one full year. Thus, one person working full time during the 36-month intervention period would be counted as three person-years for purposes of Table 1. Manufacturing companies accounted for 28 percent of the 261 WDFW companies, construction 25 percent, transportation 16 percent, wholesale and retail trade 13 percent, and service companies 8 percent. Three industry groups, (1) agriculture, forestry, and fishing, (2) mining, and (3) finance, insurance, and real estate, had only one company in the intervention cohort (Table 1). Although we include these three industry groups in the analysis for the sake of completeness, the reported injury rates are not meaningful because of the limited numbers of person-years used to calculate them. The number of person-years shown in Table 1 varies across industry group because of differences in the number and size of companies. Variation in the number of person-years within industry group over time (preintervention, intervention, and postintervention periods) reflects differences in the length of the three observation periods and fluctuations in the number of workers employed. Although not shown in Table 1, the intervention companies at the start of the WDFW Program, on average, were larger than the comparison companies (57 FTE workers versus 33 FTE workers, p <.01).
Table 1.
Number of Companies and Number of Person-Years in Intervention and Comparison Companies by Intervention Period and Type of Industry
| Washington Drug-Free Workplace Companies | Comparison Companies | |||||||
|---|---|---|---|---|---|---|---|---|
| Person-years | Person-years | |||||||
| Type of Industry | Number of Companies | Preintervention | Intervention | Postintervention | Number of Companies | Preintervention | Intervention | Postintervention |
| Multiple codes | 22 (8.4%) | 2,932 | 3,481 | 1,034 | 242 (1.2%) | 106,285 | 143,475 | 48,171 |
| Agriculture, forestry, and fishing | 1 (0.4%) | 167 | 303 | 112 | 1,949 (9.6%) | 81,834 | 111,650 | 35,399 |
| Mining | 1 (0.4%) | 136 | 121 | 34 | 82 (0.4%) | 3,556 | 4,841 | 1,566 |
| Construction | 65 (24.9%) | 7,225 | 8,305 | 3,305 | 3,895 (19.3%) | 138,740 | 197,802 | 65,720 |
| Manufacturing | 74 (28.4%) | 12,739 | 14,968 | 5,648 | 2,109 (10.4%) | 196,604 | 265,850 | 80,095 |
| Transportation and public utilities | 42 (16.1%) | 6,433 | 5,845 | 1,534 | 867 (4.3%) | 71,486 | 105,094 | 34,791 |
| Wholesale and retail trade | 33 (12.6%) | 4,434 | 5,105 | 1,566 | 5,431 (26.9%) | 423,125 | 571,896 | 182,912 |
| Finance, insurance, and real estate | 1 (0.4%) | 161 | 199 | 92 | 717 (3.5%) | 93,987 | 132,876 | 45,435 |
| Services | 22 (8.4%) | 3,133 | 3,806 | 1,455 | 4,923 (24.4%) | 540,257 | 750,506 | 239,958 |
| TOTAL | 261 (100%) | 37,359 | 42,133 | 14,780 | 20,215 (100%) | 1,655,874 | 2,283,990 | 734,047 |
Table 2.
Injury Rates and Rate Differences by Intervention Period and Type of Industry
| BEFORE | DURING | AFTER | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rate per 100 Person-years | Rate per 100 Person-years | Rate per 100 Person-years | ||||||||||
| WDFWP1 | Comparison | Difference2 | 95% CI | WDFWP | Comparison | Difference2 | 95% CI | WDFWP | Comparison | Difference | 95% CI | |
| Multiple codes | 22.42 | 12.12 | 10.30 | (8.50 to 12.11) | 23.64 | 10.862 | 12.77 | (11.21 to 14.33) | 19.34 | 10.82 | 8.52 | (6.80 to 13.61) |
| Agriculture, forestry, and fishing3 | 12.51 | 16.22 | −3.71 | (−9.67 to 2.23) | 14.37 | 14.69 | −0.32 | (−4.39 to 3.76) | 9.20 | 17.21 | −8.00 | (−14.84 to −1.16) |
| Mining3 | 26.44 | 22.97 | 3.47 | (−5.72 to 12.57) | 20.41 | 19.62 | 0.78 | (−6.99 to 8.65) | 50.22 | 21.21 | 29.01 | (1.47 to 56.09) |
| Construction | 28.18 | 28.02 | 0.17 | (−1.11 to 1.44) | 21.11 | 25.72 | −4.61 | (−5.59 to −3.65) | 20.63 | 26.93 | −6.30 | (−8.33 to −4.28) |
| Manufacturing | 28.67 | 22.25 | 6.42 | (5.45 to 7.39) | 22.35 | 19.34 | 3.01 | (2.27 to 3.76) | 23.13 | 18.81 | 4.32 | (2.71 to 5.92) |
| Transportation and public utilities | 25.32 | 16.60 | 8.71 | (7.43 to 10.00) | 24.16 | 14.95 | 9.22 | (7.97 to 10.46) | 21.33 | 15.15 | 6.18 | (3.31 to 9.04) |
| Wholesale and retail trade | 21.72 | 15.37 | 6.35 | (4.93 to 7.77) | 18.49 | 13.74 | 4.76 | (3.62 to 5.89) | 15.11 | 14.50 | 0.62 | (−1.72 to 2.94) |
| Finance, insurance, and real estate3 | 1.87 | 5.35 | −3.49 | (−5.60 to −1.38) | 2.31 | 4.52 | −2.21 | (−4.24 to −0.18) | 1.81 | 5.59 | −3.78 | (−7.34 to −0.20) |
| Services | 31.87 | 10.71 | 21.17 | (19.13 to 23.20) | 23.47 | 9.41 | 14.06 | (12.59 to 15.53) | 23.03 | 10.29 | 12.74 | (9.71 to 15.75) |
| TOTAL | 26.79 | 14.66 | 12.13 | (11.59 to 12.67) | 21.93 | 13.13 | 8.80 | (8.36 to 9.23) | 21.18 | 13.82 | 7.36 | (6.44 to 8.29) |
WDFWP represents the intervention group of companies that enrolled in the Washington Drug-Free Workplace Program.
The change in the difference measures between the preintervention and intervention periods provides an indication of program effect. If the 95% CIs around these differences do not overlap, the observed change can be interpreted as having statistical significance.
This industry group had only one intervention company and thus had too few person-years to produce meaningful injury rate estimates for the intervention cohort (see Table 1).
Table 3.
Rates and Rate Differences for Injuries Involving Four or More Lost Work Days by Intervention Period and Type of Industry
| BEFORE | DURING | AFTER | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rate per 100 Person-years | Rate per 100 Person-years | Rate per 100 Person-years | ||||||||||
| WDWFP1 | Comparison | Difference2 | 95% CI | WDWFP | Comparison | Difference2 | 95% CI | WDWFP | Comparison | Difference | 95% CI | |
| Multiple codes | 4.18 | 2.36 | 1.82 | (1.04 to 2.60) | 3.84 | 2.00 | 1.84 | (1.21 to 2.47) | 3.41 | 1.79 | 1.62 | (0.25 to 2.99) |
| Agriculture, forestry, and fishing3 | 0.74 | 3.19 | −2.45 | (−3.90 to 1.01) | 1.20 | 2.76 | −1.56 | (−2.74 to 0.38) | 1.31 | 3.15 | −1.84 | (−4.43 to 0.75) |
| Mining3 | 1.60 | 5.03 | −3.43 | (−5.77 to −1.10) | 1.51 | 4.75 | −3.24 | (−5.42 to −1.05) | 7.73 | 4.41 | 3.31 | (−7.45 to 14.01) |
| Construction | 5.21 | 5.77 | −0.56 | (−1.11 to 0.01) | 3.44 | 4.95 | −1.51 | (−1.91 to −1.12) | 2.45 | 4.79 | −2.34 | (−3.05 to −1.64) |
| Manufacturing | 4.55 | 3.75 | 0.80 | (0.41 to 1.19) | 3.61 | 3.21 | 0.41 | (0.11 to 0.71) | 3.28 | 3.01 | 0.27 | (−0.34 to 0.87) |
| Transportation and public utilities | 8.08 | 4.06 | 4.02 | (3.30 to 4.74) | 7.42 | 3.52 | 3.90 | (3.21 to 4.59) | 7.01 | 3.26 | 3.75 | (2.11 to 5.38) |
| Wholesale and retail trade | 3.93 | 2.52 | 1.40 | (0.80 to 2.01) | 3.32 | 2.29 | 1.03 | (0.55 to 1.51) | 2.78 | 2.30 | 0.48 | (−0.52 to 1.48) |
| Finance, insurance, and real estate3 | 0.62 | 0.91 | −0.29 | (−1.51 to 0.93) | 0.46 | 0.73 | −0.27 | (−1.18 to 0.64) | — | 0.92 | −0.92 | (−1.03 to 0.82) |
| Services | 6.72 | 1.74 | 4.98 | (3.75 to 5.62) | 4.21 | 1.74 | 2.47 | (1.85 to 3.09) | 3.91 | 1.67 | 2.24 | (0.99 to 3.48) |
| TOTAL | 5.33 | 2.70 | 2.63 | (2.39 to 2.87) | 4.09 | 2.38 | 1.71 | (1.53 to 1.90) | 3.50 | 2.33 | 1.17 | (0.79 to 1.55) |
WDFWP represents the intervention group of companies that enrolled in the Washington Drug-Free Workplace Program.
The change in the difference measures between the preintervention and intervention periods provides an indication of program effect. If the 95% CIs around these differences do not overlap, the observed change can be interpreted as having statistical significance.
This industry group had only one intervention company and thus had too few person-years to produce meaningful injury rate estimates for the intervention cohort (see Table 1).
Table 2 shows the injury rates for all reported injuries that occurred in the intervention and comparison cohorts and the rate differences between the cohorts for each of the three observational periods. Examination of the rate differences and confidence intervals shown in Table 2 indicates that the WDFW Program was associated with a statistically significant (p <.05) decrease in injury rates for three industry groups: construction, manufacturing, and services. The rate difference for construction companies declined from 0.17 injuries per 100 person-years in the BEFORE period to −4.61 injuries per 100 person-years in the DURING period (p <.05). Compared to the observed change in the injury rate difference of 4.78 (0.17 to −4.61 injuries per 100 person-years) for construction companies, the magnitude of change was smaller (3.41 injuries per 100 person-years) for manufacturing companies but larger (7.11 injuries per 100 person-years) for service companies. Due primarily to the change in injury rate differences for these three industry groups, the overall injury rate difference across all industry groups declined from 12.13 injuries per 100 person-years in the baseline (BEFORE) period to 8.80 injuries per 100 person-years in the intervention (DURING) period (p <.05). The net effect is a reduction of 3.33 (12.13 to 8.80) injuries per 100 person-years. In other words, on average, 3.33 fewer injuries per 100 person-years were observed in the WDFW companies during the intervention period than otherwise would have been expected to occur in the absence of the WDFW Program.
Often with health interventions of the type analyzed here a question arises regarding the durability of the intervention effect. The WDFW Program provided premium discounts to companies for up to three years. After that time, companies were not eligible for the discount and did not have to abide by the program requirements for drug testing, supervisor training, or use of EAPs for referral to treatment. We could not collect information on changes that occurred in the substance abuse prevention activities for companies whose eligibility had expired. However, we were able to gather data on reported injuries that occurred during a 12-month postintervention period (October 1999 through September 2000) and to examine injury rate differences for this time period. This enabled us to determine in a limited fashion the durability of the intervention effect.
As shown in Table 2, the difference in injury rates between the DURING and AFTER periods either stayed the same or continued to decline modestly. Among all companies, the difference in injury rates declined by 1.44 injuries per 100 person-years (8.80 to 7.36, p <.05) during the AFTER period. A similar positive change is shown for construction companies, with the difference in injury rates declining by 1.69 injuries per 100 person-years (−4.61 to −6.30, p <.05). In the services industry, the change was also favorable, with the injury rate difference declining by 1.32 injuries per 100 person-years, though this change achieved only borderline statistical significance. The opposite trend occurred in the manufacturing industry; that is, a negative change occurred in the injury rate difference because the injury rate increased slightly for the intervention cohort while decreasing slightly for the comparison cohort.
To gain additional insight into the change in injury rates associated with the WDFW Program, we present graphical information (Figure 1) regarding the (quarterly) injury incidence rates for the intervention and comparison cohorts within the construction, manufacturing, and services industries over the seven-year period of observation. To reduce the variability in the quarterly injury rates, we use two-quarter moving averages to graph the injury rates. As Figure 1 shows, the patterns of change in injury rates, though favorable for all three industry groups, are somewhat different. Within the construction industry, the baseline injury rates of the intervention and comparison companies were almost identical but trending down before the start of the WDFW Program. Shortly after the program's start, the injury rate for the intervention cohort declined sharply, whereas it stayed relatively constant for the comparison cohort. Intervention companies within the manufacturing industry had higher initial baseline injury rates that began declining before the start of the WDFW Program and continued declining thereafter until reaching a rate of 20 injuries per 100 person-years. Injury rates for comparison companies also declined, but the magnitude of change was smaller. Finally, whereas the injury rate for the comparison cohort within the services industry remained unchanged throughout the entire seven-year period of observation, the injury rate for the intervention cohort declined markedly.
Figure 1.
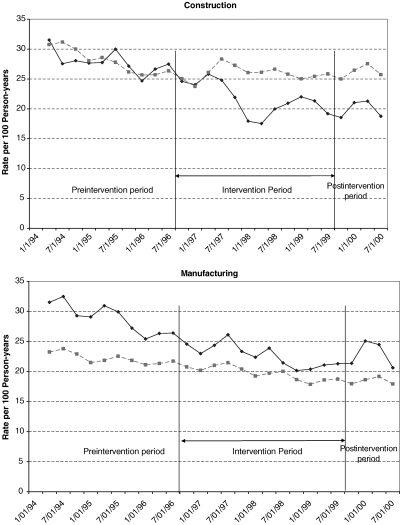
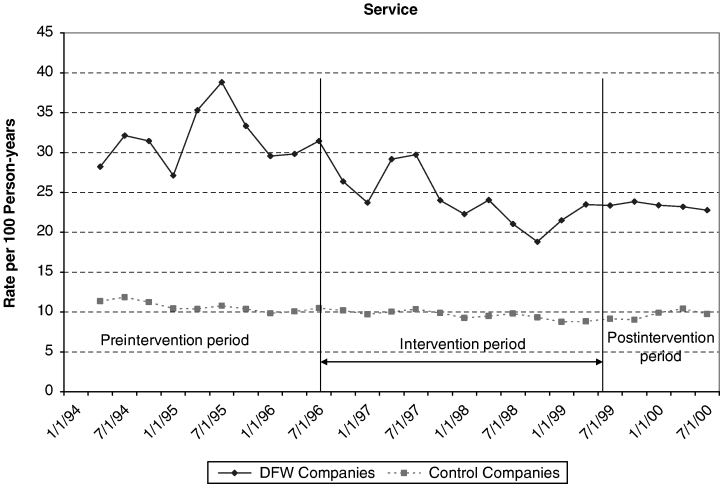
Two-Quarter Moving Average Injury Rates by Intervention Period and Type of Industry
The observed changes in injury rates shown in Figure 1 and reported in Table 2 could reflect underlying differences in the size of the intervention and comparison cohort companies noted earlier (mean size for intervention cohort companies equals 57 FTE employees versus 33 FTE employees for intervention cohort companies, p <.05). Larger companies, on average, have more sophisticated injury prevention programs and generally have lower injury rates. To assess whether the change in injury rates could have resulted from systematic differences in company size, we repeated the primary analysis for the construction and manufacturing industries with the companies stratified by size (the analysis for service companies was not redone because there was little difference in company size between the intervention and comparison cohorts). The stratified analysis generated results that were very similar to the results of the initial analysis reported in Table 2 and shown in Figure 1, with no meaningful difference in parameter estimates or statistical significance tests.
Of particular concern to employers and workers' compensation insurers are injuries that result in lost work time. These injuries require employers to pay a portion of the injured worker's lost wage in addition to all medical expenses, and they therefore have a substantial impact on workers' compensation premiums. Shown in Table 3 are injury rates and rate differences for the subset of (time loss) injuries that resulted in four or more days of lost work time. (In Washington State, employers are required to pay wage replacement only for injuries that result in four or more days of lost work time.) As would be expected, the injury rates shown in Table 3 are considerably lower than the rates shown in Table 2.
The WDFW Program was associated with a statistically significant change (p <.05) in the rate difference for time loss injuries for the construction and services industries. The injury rate differences for these two industries, respectively, in the preintervention period were −.056 and 4.98 injuries per 100 person-years. These rate differences decreased to −1.56 and 2.47 injuries per 100 person-years in the intervention period. Other industries exhibited favorable changes in the rate difference for time loss injuries but the magnitude of change did not achieve statistical significance. Across all industry groups, the change in the rate difference for time loss injuries was statistically significant, declining from 2.63 injuries per 100 person-years to 1.71 injuries per 100 person-years.
To assess the robustness of the findings generated by our confidence-interval analysis, we tested ARIMA models for each of the three industry groups where a significant change in injury rate differences occurred (construction, manufacturing, and service industries). The results of the three ARIMA models tested indicated that the intervention was associated with a statistically significant change (p <.05) in the quarterly injury rate difference after adjusting for an autoregressive component, random effects, seasonal effects, and a secular trend.
Discussion
Our study indicates that the Washington Drug-Free Workplace Program was associated with a selective, industry-specific preventive effect. For three industries, construction, manufacturing, and services, the net reduction in (all) injury rates was both meaningful and statistically significant. In terms of more serious injuries involving lost work time, a significant preventive effect was documented for two industry groups: construction and service. Due largely to this selective effect, the annual risk of any injury was reduced by about three cases per 100 person-years, while the risk of more serious (time loss) injuries was reduced by about one injury per 100 person-years. How would the reductions in injury risk reported here translate into savings for employers in workers' compensation medical and disability (wage replacement) costs? For construction, manufacturing, and service industries the average (medical and disability) cost per injury was $4,851, $2,228, and $3,222, respectively (1996 dollars). Given these costs, the injury risk reduction associated with the drug-free workplace program for a company with 50 employees would generate estimated annual savings of approximately $11,600 for construction companies, $3,800 for manufacturing companies, and $11,450 for service companies. These figures, however, do not represent net savings because they do not account for the costs of drug testing or EAP services that the employer would pay. Depending upon the frequency of testing and the cost of EAP services, these gross cost savings figures could be reduced by $1,500 to $2,000 assuming a per drug-test cost of $50 and an annual EAP cost of $20 per employee.
Occupational injuries are a major public health problem resulting in substantial disability. In the construction industry alone, there were 194,000 reported occupational injuries in 2000 involving at least one day of lost work time (Bureau of Labor Statistics 2002). It is unclear how many of these injuries could potentially have been avoided by preventive actions organized through drug-free workplace programs. Our results suggest that such programs do offer potential to reduce the occurrence of occupational injuries but on a selective basis. Two key factors influence the potential of drug-free workplace programs to reduce injury risk: the background level of injury risk and the prevalence of substance abuse in the workforce. Companies with low injury rates are unlikely to benefit from DFW programs in terms of injury risk reduction regardless of the effectiveness of these programs, although they may benefit in other ways from reduced absenteeism or decreased employee turnover. Similarly, if the prevalence of substance abuse among employees is low, a company is unlikely to benefit from a DFW program. The relatively strong intervention effect observed for the construction industry in our study may reflect, in part, the combined effect of these two factors. Both injury risk and the prevalence of substance abuse are higher in the construction industry than in other industries (Substance Abuse and Mental Health Services Administration 1999;Bureau of Labor Statistics 2002).
In a review article on drug testing published in 1993, Zwerling (1993) drew attention to the growth of the drug testing industry and its ability to actively promote drug testing as an approach to address the problem of workplace substance abuse. We would echo this concern. Over the past 20 years, the “workplace substance abuse prevention industry” has grown enormously in size and become more sophisticated in its marketing. Drug testing alone has become a $6 billion industry (Costantinou 2001). Employee assistance programs are now widely used by employers at significant cost. Our results suggest that drug-free workplace programs do bear consideration as an approach to improving workplace safety and health through substance abuse prevention. However, their use should be based upon the best available empirical evidence regarding the potential of such programs to yield positive outcomes, not on theoretical benefits or anecdotal information made through marketing claims.
Our study focused on assessing the outcomes of the intervention in terms of injury rates. We were unable to examine the effects of individual program components, for example, drug testing, use of EAPs, or supervisor training. We did conduct a limited process evaluation that included both a survey (mailed questionnaire) of WDFW participant employers and site visits to selected participant companies. The survey revealed that the great majority of employers fully implemented the program and complied with its requirements with respect to performing drug testing, developing a formal workplace policy, and offering training, education, and treatment. Qualitative information gathered through the site visits suggested the program may have helped to change the work culture in ways that promoted safety. Before the program, employers and employees, especially in the construction trades, often accepted the inevitability of workplace injuries. For companies experiencing high injury rates and substance abuse problems, the program appeared to help promote a work culture that emphasized safety and the importance of reducing injury risk through substance abuse prevention and treatment activities.
The main limitation of this study arises from its quasi-experimental design. Intervention companies enrolled in the drug-free workplace program on a voluntary basis, and therefore may have differed from the comparison companies (other than exposure to the intervention) on characteristics we could not observe. Given the data available to us, we could not adjust for this self-selection through formal statistical techniques. However, this self-selection would create a bias only if the intervention companies were more likely to experience injury risk reduction than the comparison companies, independent of the intervention. The fact that we found an intervention effect in some industries but not others suggests that a general self-selection bias is unlikely. For example, although the preintervention injury rates for the transportation and wholesale and retail trade industries were higher than the corresponding rates for the comparison cohort, these industries did not exhibit significant changes in injury rates consistent with an intervention effect. Further, although the intervention companies, on average, were larger in size than comparison companies, when we stratified for company size and repeated the analysis, we found no meaningful change in the results. The strongest evidence of an intervention effect may come from the construction industry. Injury rates in the preintervention period for the intervention and comparison cohorts were similar (Table 2), but the rate for the intervention cohort declined markedly shortly after the start of the drug-free workplace program (Figure 1).
This study has several important strengths that also bear mention. First, the study spans a substantial period of observation, seven years that includes a two and a half-year baseline (preintervention) period as well as a three-year intervention period. Second, the injury rates analyzed by the study are based on workers' compensation insurance claims information rather than worker self-report. Third, the intervention and comparison cohorts are based upon a large number of companies representing a large workforce in different industries. Fourth, we were able to test the robustness of our confidence-interval analysis by applying more sophisticated statistical analyses (ARIMA models) to control for possible time series effects. That analysis confirmed the findings of our primary statistical approach.
To our knowledge, this study represents the most detailed analysis of a drug-free workplace program conducted to date. Data for the study were based on the experience of 261 companies that enrolled in the drug-free workplace program representing a population of approximately 14,500 workers. Injury rates among this population of workers were compared to the injury rates of 20,000 comparison companies representing a workforce of approximately 650,000 workers. The drug-free workplace program we studied had a selective, preventive effect on occupational injuries. What effect it may have had on other workplace outcomes, such as absenteeism or turnover, is unknown. Substance abuse remains an important public health problem affecting the health, safety, and well-being of a sizable segment of the population. Drug-free workplace programs may offer a useful approach to substance abuse prevention under certain circumstances for selected occupational groups.
Footnotes
This study was supported by a grant from the Robert Wood Johnson Foundation's Substance Abuse Policy Research Program. Support for the process evaluation described in the paper was provided by the Washington State Division of Alcohol and Substance Abuse. The opinions and conclusions presented in the paper are those of the authors and do not represent the views of the Robert Wood Johnson Foundation or the Washington State Division of Alcohol and Substance Abuse.
References
- Alleyne BC, Stuart P, Copes R. Alcohol and Other Drug Use in Occupational Facilities. Journal of Occupational Medicine. 1991;33(4):496–500. [PubMed] [Google Scholar]
- Bureau of Labor Statistics . Washington, DC: U.S. Department of Labor; 2002. Workplace Injuries and Illnesses in 2000. [Google Scholar]
- Bush DM, Autry JH. Substance Abuse in the Workplace: Epidemiology, Effects, and Industry Response. Occupational Medicine: State of the Art Reviews. 2002;17:13–25. [PubMed] [Google Scholar]
- Costantinou M. The Drug Testing Industry Is a Multibillion Dollar Profit Center. 2001. San Francisco Chronicle August 12.
- Elam E, Taylor V, Ciol MC, Franklin GM, Deyo RA. Impact of a Workers' Compensation Practice Guideline on Lumbar Spine Fusion in Washington State. Medical Care. 1997;35(5):417–24. doi: 10.1097/00005650-199705000-00001. [DOI] [PubMed] [Google Scholar]
- Gust SW, Walsh JM. Drugs in the Workplace: Research and Evaluation Data. Rockville, MD: National Institute on Drug Abuse; 1989. [Google Scholar]
- Gutierrez-Fisac JL, Regidor E, Ronda E. Occupational Accidents and Alcohol Consumption in Spain. International Journal of Epidemiology. 1992;21(6):1114–20. doi: 10.1093/ije/21.6.1114. [DOI] [PubMed] [Google Scholar]
- Hertz R, Emmett E. Risk Factors for Occupational Hand Injury. Journal of Occupational Medicine. 1986;26(4):2639–43. doi: 10.1097/00043764-198601000-00010. [DOI] [PubMed] [Google Scholar]
- Hingson RW, Lederman RI, Walsh DC. Employee Drinking Patterns and Accidental Injury: A Study of Four New England States. Journal of Studies of Alcohol. 1985;46(4):298–303. doi: 10.15288/jsa.1985.46.298. [DOI] [PubMed] [Google Scholar]
- Ledolter J, Chan KS. Evaluating the Impact of the 65 mph Maximum Speed Limit on Iowa Rural Interstates. American Statistician. 1996;50(1):79–86. [Google Scholar]
- Lehman W, Simpson D. Employee Substance Use and On-the-Job Behaviors. Journal of Applied Psychology. 1992;77(3):309–21. doi: 10.1037/0021-9010.77.3.309. [DOI] [PubMed] [Google Scholar]
- Lewis RJ, Cooper SP. Alcohol, Other Drugs, and Fatal Work Injuries. Journal of Occupational Medicine. 1989;31(1):23–8. [PubMed] [Google Scholar]
- Loftin C, McDowall D, Wiersema B, Cottey TJ. Effects of Restrictive Licensing of Handguns on Homicide and Suicide in the District of Columbia. New England Journal of Medicine. 1991;325(23):1615–20. doi: 10.1056/NEJM199112053252305. [DOI] [PubMed] [Google Scholar]
- Moll van Charante A, Mulder PG. Perceptual Acuity and the Risk of Industrial Accidents. American Journal of Epidemiology. 1990;131(4):652–63. doi: 10.1093/oxfordjournals.aje.a115549. [DOI] [PubMed] [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism and National Institute on Drug Abuse. The Economic Costs of Alcohol and Drug Abuse in the United States—1992. Washington, DC: U.S. Government Printing Office; 1998. [Google Scholar]
- National Research Council. Under the Influence? Drugs and the American Work Force. Washington, DC: National Academy Press; 1994. [PubMed] [Google Scholar]
- Normand J, Salyards SD, Mahoney J. An Evaluation of Preemployment Drug Testing. Journal of Applied Psychology. 1990;75(6):629–39. doi: 10.1037/0021-9010.75.6.629. [DOI] [PubMed] [Google Scholar]
- Office of Applied Studies, Substance Abuse and Mental Health Services Administration. National Household Survey on Drug Abuse: Main Findings, 2000. Rockville, MD: U. S. Department of Health and Human Services; 2002. [Google Scholar]
- Office of National Drug Control Policy. The Economic Costs of Drug Abuse in the United States, 1992–1998. Washington, DC: Executive Office of the President; 2001. Publication no. NCJ-190636. [Google Scholar]
- Parish DC. Relation of the Pre-Employment Drug Testing Result to Employment Status: A One-Year Follow-up. Journal of General Internal Medicine. 1989;4(1):44–7. doi: 10.1007/BF02596490. [DOI] [PubMed] [Google Scholar]
- Pindyck S, Rubinfeld DL. Econometric Models and Economic Forecasts. New York: McGraw-Hill; 1991. [Google Scholar]
- Pollock ES, Franklin GM, Fulton-Kehoe D, Chowdhury R. Risk of Job-Related Injury among Construction Laborers with a Diagnosis of Substance Abuse. Journal of Occupational and Environmental Medicine. 1998;40(6):573–83. doi: 10.1097/00043764-199806000-00011. [DOI] [PubMed] [Google Scholar]
- Rothman KJ. Toronto: Little, Brown; 1986. Modern Epidemiology; pp. 153–236. [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA) Rockville, MD: 1999. Worker Drug Use and Workplace Policies and Programs: Results from the 1994 and 1997 Household Survey. DHHS Publication no. (SMA) 99-3252. [Google Scholar]
- Zwerling C. Current Practice and Experience in Drug and Alcohol Testing in the Workplace. Bulletin of Narcotics. 1993;45(2):155–96. [PubMed] [Google Scholar]
- Zwerling C, Ryan J, Orav JE. The Efficacy of Preemployment Drug Screening for Marijuana and Cocaine in Predicting Employment Outcome. Journal of the American Medical Association. 1990;264(20):2639–43. [PubMed] [Google Scholar]