

Abstract
A life-span health-behavior model was investigated in this longitudinal study of personality influences on health. Teachers assessed 963 elementary school children on traits that formed scales assessing the dimensions of the five-factor (Big Five) model of personality. Smoking, alcohol use, body mass index (BMI), and self-rated health were assessed 40 years later in midlife. Childhood personality traits were significantly associated with all four outcomes, and the effects were consistently larger for women than men. For men and women, childhood Conscientiousness was associated with less adult smoking and better adult self-rated health and, for women only, with lower adult BMI. Mediation analyses suggested that the effects of Conscientiousness on self-rated health were partially mediated by smoking and BMI. These findings add to the growing evidence that childhood personality traits predict adult health outcomes, and are discussed in terms of future testing of the life-span health-behavior model.
Keywords: Big Five, smoking, alcohol, BMI, self-rated health, longitudinal study,
Forty Years On1: Teachers’ Assessments of Children’s Personality Traits Predict Self-Reported Health Behaviors and Outcomes at Midlife
Chronic diseases are the end product of a lifetime of genetic, environmental, and situational influences. Studies spanning long intervals in adulthood suggest that temperament and personality variables can have far-reaching effects on health (e.g., Adams, Cartwright, Ostrove, Stewart, & Wink, 1998; Graves, Mead, Wang, Liang, & Klag, 1994; Danner, Snowden, & Friesen, 2001). The question remains whether personality traits assessed in childhood, when personality is still developing, are important for adult health outcomes. For the purpose of preventing chronic illness, the earlier that at-risk individuals can be identified the better.
Personality traits have been shown to influence children’s and adolescents’ health-damaging behaviors such as smoking and alcohol use (e.g., Caspi, 2000; Caspi et al., 1995; Tarter et al., 1999). These and other studies implicate personality traits associated with low restraint (e.g., low achievement orientation, unconventionality, sensation seeking, lack of ego control, high activity, learning difficulties, unconscientiousness) and poor social adaptation (e.g., low positive affect, aggressiveness, shyness, disagreeableness) as determinants of children’s health-damaging behaviors (e.g., Gerrard, Gibbons, Benthin, & Hessling, 1996; Jessor & Jessor, 1977; Markey, Markey, & Tinsley, 2003; Shedler & Block, 1990; Wills, DuHamel, & Vaccaro, 1995; Zuckerman, 1991). However, with one important exception (Friedman et al., 1993), none of the longitudinal studies of children’s personality traits have followed the sample beyond young adulthood.
Evidence for childhood personality influences on adult health outcomes, specifically on longevity, has emerged from the Terman Life Cycle study (Terman & Oden, 1947). Childhood Conscientiousness was predictive of greater longevity for both men and women (more strongly for men than women); permanence of mood showed some evidence of being protective for men; and childhood cheerfulness was predictive of a shorter lifespan (Friedman et al., 1993). The magnitude of these childhood personality risk factors was comparable to those of elevated serum cholesterol level and elevated resting systolic blood pressure in adulthood. The Terman Life Cycle study, which provides initial support for a continuous developmental path from child personality to adult health outcomes, inspired the present study.
In the absence of other studies spanning the decades from childhood to midlife, research on associations between adult personality traits and adult health behaviors provides another source of hypotheses about enduring influences of childhood personality. Personality influences on adult health behaviors and outcomes have been examined using the five-factor model (Digman, 1990; John & Srivastava, 1999). This model has the advantage of providing a unifying, hierarchical taxonomy for traits (Goldberg, 1993), and enables the study of both broad and narrow personality influences using a widely accepted framework (Marshall, Wortman, Vickers, Kusulas, & Hervig, 1994; Smith & Williams, 1992). At the broadest level of personality description, the model identifies five bipolar dimensions referred to as the Big Five: Extraversion versus Introversion (e.g., assertive, energetic versus shy, submissive), Agreeableness versus Hostility (e.g., helpful, kind versus rude, cruel), Conscientiousness versus Unconscientiousness (e.g., controlled, hardworking versus careless, impulsive), Emotional Stability versus Neuroticism (e.g., calm, well-balanced versus anxious, moody), and Intellect/Openness versus Unintellectual/Not open to experience (e.g., curious, creative versus unintelligent, unimaginative).
One or more of the Big Five traits have been associated with a number of self-reported health behaviors and health outcomes among adults (Booth-Kewly & Vickers, 1994; Ingledew & Brunning, 1999). In particular, traits related to Conscientiousness have been consistently associated with health behaviors that are risk factors for chronic illness (Bogg & Roberts, 2004). For example, Conscientiousness has been associated with less tobacco use (Clark & Watson, 1999; Tucker et al., 1995), reduced exposure to environmental tobacco smoke (Hampson, Andrews, Barckley, Lichtenstein, & Lee, 2000), and less alcohol consumption (Tucker et al., 1995). Christensen et al. (2002) observed higher mortality rates over four years in chronic renal-insufficiency patients with low Conscientiousness scores.
Other studies have implicated each of the remaining Big Five domains as predictors of adult health behaviors and/or health outcomes. Extraversion has been associated with higher levels of smoking and physical exercise (Gilbert, 1995; Rhodes & Courneya, 2003), and the sociability facet of Extraversion was protective against the common cold (Cohen, Doyle, Turner, Alper, & Skoner, 2003). Extraverts and those with higher scores on Agreeableness tend to perceive themselves to be in better health (Goodwin & Engstrom, 2002). Lack of Agreeableness subsumes hostility, which has been associated with cardiovascular and other diseases (Barefoot et al., 1991). Individuals with lower scores on Emotional Stability (i.e., higher scores on Neuroticism or Negative Affect) tend to report more symptoms and perceive themselves in poorer health (Costa & McCrae, 1987; Jerram & Coleman, 1999). Christensen et al. (2002) observed higher mortality rates in chronic renal-insufficiency patients with high Neuroticism scores, although Emotional Stability/Neuroticism has not been consistently associated with mortality (Korten et al., 1999). Intellect/Openness was associated with more healthful food habits (Goldberg & Strycker, 2002), and childhood intelligence (distinct from but related to Intellect/Openness) has been associated with longevity (Whalley & Deary, 2001).
Personality traits influence health by processes involving three broad classes of factors: health behaviors, social environmental variables, and physiological mechanisms (Adler & Matthews, 1994; Friedman, 2000). Models of the relations between personality and health typically focus on a subset of these variables and mechanisms. In the present study, we tested elements of a health-behavior model, and did so from a life-span perspective (Smith & Spiro, 2002). The health-behavior model postulates that the influence of personality traits on morbidity and mortality is mediated by health behaviors. Good health status is expected to result from enduring patterns of performance of health-enhancing behaviors and avoidance of health-damaging behaviors. The Terman Life Cycle study only partially supported the health-behavior model. The effects of conscientiousness (Friedman et al., 1995) and of cheerfulness (Martin et al., 2002) on longevity were not fully mediated by their associations with risky hobbies, alcohol and tobacco use, and obesity. These findings are a reminder that health outcomes are determined by numerous other factors which may also be influenced by personality traits.
In the present study, childhood personality traits were assessed by teachers when the participants were in elementary school. Entire classrooms participated, so to the extent that the adult sample is representative of the original cohort, it should also be representative of the elementary school population in these islands of Hawaii at that time (1959–1967). These data were used to derive scores on the Big Five (Goldberg, 2001). Forty or so years later, the participants completed a questionnaire asking about their health behaviors and their health status. The participants differ markedly from the exclusively white and high IQ sample of the Terman study because they are drawn from diverse cultural groups in Hawaii, and they represent a wide range of educational attainment.
This report presents findings for four outcomes: cigarette smoking, alcohol use, body mass index (BMI), and self-rated health. Smoking, alcohol use, and BMI are established behavioral risk factors for the leading causes of mortality (cardiovascular disease, cancers, and diabetes). They were analyzed extensively in the Terman data by Friedman and his colleagues (e.g., Friedman et al., 1993; 1995; Tucker et al., 1995). Self-rated health is of particular interest as a self-report measure of health status because it is one of the best predictors of mortality (Idler & Benyamini, 1997; Benyamini, Leventhal, & Leventhal, 1999).
Based on the life-span health-behavior model, it was hypothesized that there would be significant prospective associations between childhood personality traits and adult health behaviors and health outcomes assessed 40 years later. Past research on adults and children, including the Terman Life Cycle study, provided grounds for predicting independent contributions from all of the Big Five personality domains in the prediction of health behaviors and health outcomes. It was hypothesized that higher levels of childhood Conscientiousness would predict lower levels of adult smoking, alcohol use, and BMI, and higher self-rated health. Higher levels of Extraversion were predicted to be associated with more smoking and alcohol use. For the remaining Big-Five traits (Agreeableness, Emotional Stability, and Openness/Intellect), higher scores in childhood were expected to predict better adult outcomes (i.e., less smoking and alcohol use, lower BMI, and better self-rated health).
Personality traits may exert different influences on adult outcomes for men versus women. Friedman et al. (1993) reported stronger effects of Conscientiousness on mortality for men than women, and permanence of mood was only protective for men, which suggests that corresponding gender differences would be expected in the associations between personality traits and intermediate outcomes such as the ones studied here. In other analyses of the Terman data, Tucker et al. (1995) did not find trait-by-gender interactions in the prediction of smoking and alcohol use. However, not all possible interactions were examined in that study. In a study of older people, Jerram and Coleman (1999) found that Agreeableness and Openness were more important predictors of various health measures (including self-rated health) for women, and Emotional Stability and Conscientiousness were more important for men. Given these indications that personality traits may influence health-related outcomes differently for men and women, the gender-by-trait interactions for the five traits were examined here.
This study also provided an opportunity to begin to test possible mediational pathways (i.e, from childhood personality through health behaviors to adult health outcome) implied by a life-span, health-behavior model. Smoking, alcohol use, and BMI (a proxy for over-eating and under-exercising) are expected to be mediators of the influence of childhood traits on self-rated health.
Method
Participants
The sample consisted of people who, as children in elementary schools in Hawaii, were assessed on personality scales by their teachers and as adults completed a self-report questionnaire assessing health behaviors and outcomes. Of the 2,337 members of the original childhood cohort not known to be deceased and for whom first and second names were available, 1,707 (73%) were located. Of those, 1,057 (62% of those located) gave their written consent to participate in this follow-up study and for their childhood personality assessments to be used, and completed the adult questionnaire2. These participants are representative of the original sample of children in terms of gender (47% women) and scores on the Big Five personality dimensions derived from the teacher assessments (Hampson et al., 2001). The adult sample is composed of 37% Japanese Americans, 21% Native Hawaiian or part-Hawaiian Americans, 18% of European ancestry, and 24% of Filipino, Chinese, Okinawan, Korean, or other Pacific Island ancestry. For the analyses reported here, the participants (N = 963; 518 men and 445 women) included the three of the six subsamples referred to by Goldberg (2001) as the Oahu and Kauai samples; the three samples of children from the University of Hawaii laboratory school (who were assessed on other variables) were not analyzed.
Study Design
Teachers’ assessments of childhood personality traits were obtained between 1959–1967 when the children were in grades 1, 2, 5, or 6. Self-reports of health behaviors and outcomes were obtained by mailed questionnaires completed between November 1999 and October 2000 when participants ranged in age from 41 to 50 years (Mean age = 45 years, SD = 2 years).
Measures
Child personality traits.
A detailed description of the childhood measures and the teacher assessment procedures has been provided by Goldberg (2001). Six subsamples of elementary-school children were assessed by their teachers (N = 88) at the end of the school year on 36 to 63 personality attributes that differed somewhat across samples. The variables were originally chosen by Digman to represent at least 10 personality dimensions, although his analyses of these data revealed a robust five-factor structure (Digman & Inouye, 1986). For the subsamples used in this study, extensive definitions developed from focus groups with teachers were provided along with each trait (e.g., “Persevering: Keeps at his (her) work until it is completed; sees a job through despite difficulties, painstaking and thorough”). Teachers rank-ordered all the students in their classroom from lowest to highest on each trait using a fixed 9-step quasi-normal distribution. Scores on each trait were standardized within each gender (M = 0, SD = 1) so as to remove any confound between the child’s gender and their level on the trait.
In recent analyses of these data, Goldberg (2001) identified no more than five broad factors and demonstrated their equivalence to the Big-Five factor structure. The five-factor structure was recovered from both analyses of selected marker traits and from analyses of all the traits included in the assessments. These analyses were conducted separately for the Oahu 1st and 2nd graders, the Oahu 5th and 6th graders, and the Kauai sample. The mean factor loadings for the markers on their targeted factors ranged from .66 to .85 across these three subsamples. Childhood personality factor scores for each of the Big Five were derived for each participant based on the analyses of all the traits included in the assessments.
Smoking.
To qualify as ever having smoked cigarettes, participants had to report smoking at least 100 cigarettes in their entire lives. The present extent of smoking was assessed using the following scale: 0 = “Never smoked,” 1 = “Ex-smoker,” 2 = “Smokes less than half a pack day,” and 3 = “Smokes half a pack or more a day.”
Alcohol use.
This variable was constructed by multiplying the number of days in the past month that alcohol was drunk by the amount of drinks typically drunk on one occasion.
BMI.
Participants reported their height and weight, which were converted to BMI (weight/[height2]).
Self-reported health.
This variable was assessed by a widely used item from the SF-36 Medical Outcomes Health Survey (Ware & Sherbourne, 1992): “Compared to others of your same age and gender, would you say that in general your health is Poor, Fair, Good, Very Good, or Excellent?”
Participants indicated the highest level of education they had attained, and they identified their cultural/ethnic background.
Procedures
Participants completed these measures as part of a questionnaire sent to them by mail. Upon return of the completed survey and consent form, they received a modest payment.
Results
Preliminary Analyses
The correlations between each of the four outcomes and gender, grade, educational attainment, and cultural group membership are presented in Table 1. Being male was associated with smoking and drinking more, and having higher BMI. Higher educational attainment was associated with less smoking, less alcohol use, lower BMI and better self-rated health. Japanese-Americans smoked less. Hawaiian-Americans smoked more, had higher BMIs and poorer self-rated health. European-Americans had better self-rated health. In preliminary regression analyses, including cultural-group variables as predictors had few effects on which traits predicted the adult outcomes. Therefore, cultural group was not included in the regression models reported below. Although not significant at the univariate level, grade (i.e., 1, 2, 5, or 6) was still included in all the multivariate analyses reported below to control for any effects of age differences at the time of the personality assessments.
Table 1.
Correlations Between Participant Characteristics and Adult Outcomes
| Smoking | Alcohol Use | BMI | Self-Rated Health | |
|---|---|---|---|---|
| Grade at childhood assessment | .00 | −.00 | .02 | −.04 |
| Gender (M = 0, F = 1) | −.11** | −.23** | −.15** | .06 |
| Educational attainment | −.32** | −.09** | −.22** | .20** |
| Japanese-American | −.06 | −.03 | −.20** | −.12 |
| Hawaiian-American | .16** | −.01 | .18** | −.08* |
| European-American | −.04 | .06 | −.03 | .18** |
* p < .05, ** p < .01
Predicting adult outcomes separately for men and women.
Step-wise multiple regressions were conducted to investigate the childhood trait predictors of each of the four outcomes (smoking, alcohol use, BMI, and self-rated health). To obtain an estimate of the amount of variance predicted by personality traits without the influence of gender, these analyses were conducted separately for men and women. The results, presented in Table 2, indicated that the childhood traits were consistently more highly associated with women’s outcomes than with men’s. For women, lower levels of childhood Agreeableness and Conscientiousness were associated with smoking; none of the childhood traits predicted adult smoking for men. For women, higher levels of childhood Extraversion and lower levels of childhood Conscientiousness were associated with alcohol use; lower levels of childhood Emotional Stability were associated with alcohol use for men. For women, lower levels of childhood Agreeableness and Conscientiousness were associated with higher BMI; higher levels of childhood Emotional Stability were associated with higher BMI for men. For women, higher levels of childhood Extraversion and Conscientiousness were associated with better self-rated health; none of the childhood traits predicted self-rated health for men.
Table 2.
Childhood Trait Predictors of Adult Outcomes Analyzed Separately for Women and Men
| R | Adj R | F | df | ß | t | |
|---|---|---|---|---|---|---|
| Smoking | ||||||
| Women | .27 | .26 | 16.80*** | 2, 442 | ||
| Agreeableness | −.25 | −5.41*** | ||||
| Conscientiousness | −.11 | −2.47* | ||||
| Men | - | - | - | - | - | - |
| Alcohol Use | ||||||
| Women | .18 | .17 | 7.10*** | 2, 432 | ||
| Extraversion | .13 | 2.71** | ||||
| Conscientiousness | −.13 | −2.70** | ||||
| Men | .10 | .10 | 5.68* | 1, 506 | ||
| Emotional Stability | −.10 | −2.38* | ||||
| Body Mass Index | ||||||
| Women | .21 | .19 | 9.52*** | 2, 433 | ||
| Agreeableness | −.11 | −2.33* | ||||
| Conscientiousness | −.18 | −3.86*** | ||||
| Men | .12 | .11 | 6.88** | 1, 506 | ||
| Emotional Stability | .12 | 2.62** | ||||
| Self-Rated Health | ||||||
| Women | .18 | .17 | 7.27*** | 2, 440 | ||
| Extraversion | .11 | 2.36* | ||||
| Conscientiousness | .14 | 2.93** | ||||
| Men | - | - | - | - | - | - |
* p < .05, ** p < .01, *** p < .001
Predicting Adult Outcomes Including Gender in the Regression Models
Analyses conducted separately for men and women do not evaluate the significance of gender differences or of gender-by-trait interactions. Therefore, regressions were conducted in which the predictors were the five childhood traits and the interactions between each of the traits and gender. Nonsignificant (p > .05) predictors were removed by backwards elimination, starting with the trait-by-gender interactions. Significant interactions with gender were evaluated in simple slope analyses following procedures recommended by Aiken and West (1991). Table 3 shows the significant variables to enter the final models. In Table 3, for the significant gender interactions, the statistics for the main effect of the trait involved in the interaction are reported with gender coded men = 0, women = 1. To determine the main effect for women, the regression was re-run with reverse coding for gender, and the relevant statistics for the main effect are provided in the text.
Table 3.
Final Models of Childhood Trait Predictors of Adult Outcomes
| R | Adj R | F | df | ß | t | |
|---|---|---|---|---|---|---|
| Smoking | .21 | .20 | 9.27*** | 5, 957 | ||
| Gender | −.07 | −2.11* | ||||
| Agreeableness | −.05 | −1.11 | ||||
| Conscientiousness | −.10 | −3.00** | ||||
| Gender X Agreeableness | −.12 | −2.86** | ||||
| Alcohol Use | .26 | .26 | 17.39*** | 4, 938 | ||
| Gender | −.23 | −7.26*** | ||||
| Extraversion | .09 | 2.94** | ||||
| Emotional Stability | −.08 | −2.49*** | ||||
| Body Mass Index | .22 | .21 | 6.96*** | 7, 936 | ||
| Gender | −.10 | −2.77** | ||||
| Agreeableness | −.06 | −1.99* | ||||
| Conscientiousness | −.02 | −0.40 | ||||
| Emotional Stability | .11 | 2.49** | ||||
| Gender X Conscientiousness | −.12 | −2.85* | ||||
| Gender X Emotional | −.09 | −2.00* | ||||
| Stability | ||||||
| Self-Rated Health | .14 | .13 | 5.08*** | 4, 954 | ||
| Extraversion | .06 | 2.01* | ||||
| Conscientiousness | .11 | 3.31** |
Note. Gender coded: Men = 0, women = 1
* p < .05, ** p < .01, *** p < .001
Table 3 presents the final models for each of the four adult outcomes: (a) For both men and women, lower levels of childhood Conscientiousness were associated with smoking. For women only, lower levels of childhood Agreeableness were associated with smoking (ß = −.23, t = −4.96, p > .01). (b) Men were likely to be drinking more alcohol than women. For both men and women, higher levels of childhood Extraversion and lower levels of Emotional Stability were associated with alcohol use. (c) For both men and women, lower levels of childhood Agreeableness were associated with higher BMI. For men only, higher levels of childhood Emotional Stability were associated with higher BMI. For women only, lower levels of childhood Conscientiousness were associated with higher BMI (ß = −.21, t = −4.00, p < .001). (d) Gender was not a significant predictor of self-rated health. For both men and women, higher levels of childhood Extraversion and Conscientiousness were associated with better self-rated health.3
Mediation Analyses
The possibility that the relations identified above suggest life-course pathways from childhood personality traits to adult outcomes was examined in mediation analyses. Tests for mediation were conducted following procedures described by Baron and Kenny (1986). The requirements for mediation are that (1) the independent variable must predict the dependent variable, (2) the independent variable must predict the mediator, and the mediator must predict the dependent variable, and (3) when the mediator is included in the model with the independent variable, the relation between the independent variable and the dependent variable is substantially reduced (Baron & Kenny, 1986). This last step may be operationalized by testing the significance of the indirect path through the mediator using Sobel’s (1982) standard error. Testing the indirect path is superior to relying on comparison of the coefficients in steps (1) and (3) because these can be affected by the multicollinearity between the mediator and the independent variable. Focusing only on the most robust of the findings summarized in Table 3 (i.e., only those at p < .0125), there were two plausible pathways.
First, for both men and women, smoking may mediate the relation between childhood Conscientiousness and adult self-rated health. Lower levels of childhood Conscientiousness were associated with more adult smoking, and lower levels of childhood Conscientiousness predicted poorer self-rated health. The correlation between smoking and self-rated health was −.20, p < .01. Thus, childhood Conscientiousness may influence adult self-rated health through its effect on smoking. The results of the mediation analysis are shown in Figure 1. The direct path coefficient between Conscientiousness and self-rated health was reduced but remained significant with the inclusion of the mediator. The indirect path was significant, indicating that smoking partially mediated the effect of childhood Conscientiousness on adult self-rated health (z = −2.49, p < .05).
Figure 1.
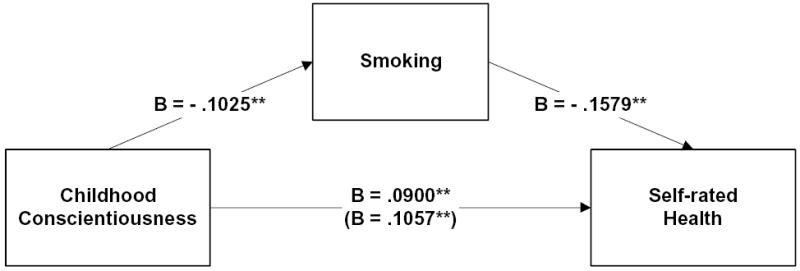
Direct and Indirect Influence of Childhood Conscientiousness on Self-Rated Health with Smoking as the Mediator (Men and Women)
Note to Figure 1. Unstandardized path coefficients are shown. The coefficient in parentheses is from the model that did not include the mediator.
* p < .05, ** p < .01
Second, for women only, BMI may mediate the relation between childhood Conscientiousness and adult self-rated health. Lower levels of childhood Conscientiousness were associated with higher adult BMI and lower levels of childhood Conscientiousness predicted poorer self-rated health. The correlation between BMI and adult self-rated health was −.36, p < .01. Thus, women’s childhood Conscientiousness may influence adult self-rated health through its effect on BMI. The results of the mediation analysis are shown in Figure 2. The direct path between Conscientiousness and self-rated health was reduced but remained significant with the inclusion of the mediator. The indirect path was significant, indicating that BMI partially mediated the effect of childhood Conscientiousness on adult self-rated health (z = 3.65, p < .001).
Figure 2.
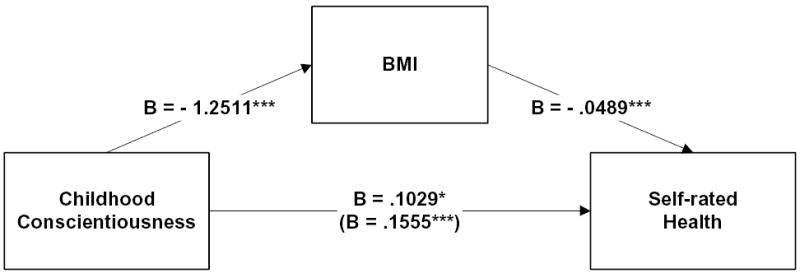
Direct and Indirect Influence of Childhood Conscientiousness on Self-Rated Health with BMI as the Mediator (Women Only)
Note to Figure 2. Unstandardized path coefficients are shown. The coefficient in parentheses is from the model that did not include the mediator.
* p < .05, ** p < .01, *** p < .001
Discussion
In this prospective study spanning the forty years from childhood to mid-life, personality traits assessed by teachers when the participants were in elementary school predicted health-related outcomes in adulthood. The effect sizes were consistently larger for women than men. All of the childhood traits were associated with outcomes for one or both genders, except Openess/Intellect. In particular, childhood Conscientiousness was associated with smoking, BMI, and self-rated health. The influence of childhood Conscientiousness on adult self-rated health was partially mediated by smoking and BMI. Together, these findings provide preliminary support for a life-span health-behavior model and point to mechanisms underlying trajectories from childhood personality traits to adult health outcomes.
The results replicate several findings from analyses of smoking, alcohol use, and BMI in the Terman Life Cycle study and also demonstrate some associations not revealed in the Terman data. Friedman et al. (1995) found that conscientious children were less likely to grow up to become smokers, although the effect was only marginally significant for women. In the present study, less childhood Conscientiousness was associated with more adult smoking for both men and women. The measure of Conscientiousness used in Friedman and colleagues’ analyses included elements of Agreeableness (e.g., “freedom from vanity”). Consistent with this overlap, in the present study, less childhood Agreeableness for women was also found to be associated with more adult smoking, perhaps because less agreeable girls were more likely to experiment with this counter-normative behavior and become smokers. Unlike findings from the Terman data, the present study did not observe an association between childhood Conscientiousness and adult alcohol use. However, Tucker et al.’s (1995) analyses of the Terman data showed that childhood sociability was associated with adult alcohol use, and in the present study childhood Extraversion (which subsumes sociability) was associated with adult alcohol use. Childhood Conscientiousness was not associated with adult BMI in the Terman data (Friedman et al., 1995) but it was for women in the present study.
The greater predictability of women’s outcomes than men’s was an unanticipated finding. Friedman et al. (1993) found some evidence of the reverse gender difference for the association between childhood Conscientiousness and longevity (i.e., greater predictability for men). They speculated that, through restricted social roles, women in the Terman sample may have shown less variation in their health behaviors and that this provided fewer opportunities for low Conscientiousness to work its ill effects on longevity. The Hawaii cohort may differ in this regard. The expansion of gender-appropriate roles for women compared to men over the latter half of the twentieth century (e.g., women’s increased representation in the work-force) may have increased women’s opportunities for behavioral choices influenced by personality traits.
A life-span health-behavior model proposes that the influences of children’s personality traits on adult health outcomes are mediated by health behaviors. Friedman et al. (1995) tested this model by examining whether smoking and alcohol use mediated the effects of low childhood Conscientiousness on mortality. Their findings showed partial mediation whereby the effects of Conscientiousness on mortality were still significant even after accounting for the indirect effects through these health behaviors. In the present study, the effects of childhood Conscientiousness on adult self-rated health were partially mediated by smoking and BMI. The absence of fully mediated effects in either sample is not really surprising given that the influence of childhood Conscientiousness unfolded over decades with numerous opportunities for other biological and social-environmental variables to influence morbidity and mortality. Fortunately, the Hawaii cohort offers opportunities to investigate many aspects of participants’ past lives as well as to continue to study them in the future. Therefore, more comprehensive evaluations of mediators of health outcomes will be possible.
The major finding from the Terman Life Cycle study that prompted this investigation was the association between childhood Conscientiousness and longevity. The Hawaii cohort is currently relatively free from morbidity and mortality. However, there are indications in this sample that Conscientiousness may eventually exert a similar influence among these individuals. Lower childhood Conscientiousness predicted poorer self-rated health for both men and women in the present sample, and self-rated health is a reliable predictor of mortality (Idler & Benyamini, 1997). As reported previously by Hampson et al. (2000), the 32 men known to have died in the Hawaii cohort scored over one quarter of a deviation below the average for their peers on childhood Conscientiousness. As the cohort is followed into the future, associations between Conscientiousness and self-rated health and mortality will be closely monitored.
The present study has a number of limitations related to the numerous as yet unanswered questions about the influence of other variables over the life span on this cohort’s health behaviors and health outcomes. For example, the influence of socio-economic status was not examined. Lower educational attainment is linked to lower socio-economic status, which is associated with poorer health (Adler, Marmot, McEwen, & Stewart, 1999). As shown in Table 1, educational attainment was associated with all of the outcomes reported here. Educational attainment is influenced by childhood personality traits, particularly those associated with Conscientiousness and Intellect/Openness (Shiner, Masten, & Roberts, 2003) and may be a powerful way to capture important aspects of an individual’s life path. Therefore, instead of offering an alternative explanation for heath outcomes, educational attainment (and socioeconomic status) may mediate the influence of childhood traits such as Conscientiousness on adult health-related outcomes. We will investigate this hypothesis in a later report.
In conclusion, the associations between childhood personality traits and four key health-related outcomes at midlife found here provide compelling, preliminary support for the life-span health-behavior model. At midlife, most people do not have manifest disease, although the pathological processes that lead to diseases such as diabetes, cardiovascular disease, and cancer may already be well-established. This study identified childhood personality traits that predicted adult risk factors for these diseases. This representative, multi-ethnic sample with comprehensive childhood personality data provides a unique opportunity for ongoing prospective research into the early determinants of lifelong behavior patterns and their relations to health outcomes.
Footnotes
This research was supported by grants from the National Institute on Aging (AG20048) and the National Institute of Mental Health (MH556000). authors are indebted to John M. (Jack) Digman 1923-1998) for obtaining the childhood teacher assessments. We thank Anthony J. Marsella for his many contributions to the project, and Winter Hamada, Jennifer Matsukawa, Heather Morse, and Edward Suarez for their assistance in locating the adult sample. We are also grateful to Sheldon Cohen and Howard Friedman for commenting on a previous version of the manuscript, Maureen Barkley for her assistance with the data analyses, and Chris Arthun, Susan Long and Melissa Peterson for their help with manuscript preparation.
With apologies to dramatist Alan Bennett for borrowing the title from one of his plays (Forty Years On; Getting On; Habeas Corpus. London: Faber, 1985).
The findings reported here are from the first wave of adult recruitment. To date, we have now located 1,944 and recruited 1,224 members of the original cohort.
These regressions were repeated using a Bonferroni correction to adjust for testing predictors of four outcomes. Nonsignificant predictors (p > .0125) were removed from the models. The more stringent significance level did not alter the pattern of results for smoking but did reduce the number of significant trait predictors for the other three outcomes. The remaining significant effects were as follows. Higher levels of childhood Extraversion predicted more alcohol use for both men and women. For women only, lower levels of childhood Conscientiousness predicted higher BMI. Higher levels of childhood Conscientiousness predicted better self-rated health for both men and women.
Contributor Information
Sarah E. Hampson, University of Surrey and Oregon Research Institute.
Lewis R. Goldberg, Oregon Research Institute
References
- Adams SH, Cartwright LK, Ostrove JM, Stewart AJ, Wink P. Psychological predictors of good health in three longitudinal samples of educated midlife women. Health Psychology. 1998;17:412–420. doi: 10.1037//0278-6133.17.5.412. [DOI] [PubMed] [Google Scholar]
- Adler N, Matthews K. Health psychology: Why do some people get sick and some stay well? Annual Review of Psychology. 1994;45:229–259. doi: 10.1146/annurev.ps.45.020194.001305. [DOI] [PubMed] [Google Scholar]
- Adler, N. E., Marmot, M., McEwen, B. S., & Stewart, J. (Eds.) (1999). Socioeconomic status and health in industrial nations: Social, psychological and biological pathways New York, NY: New York Academy of Sciences. [PubMed]
- Aiken, L. S, & West, S. G. (1991). Multiple regression: Testing and interpreting interactions. Newbury Park, CA: Sage.
- Barefoot JC, Peterson BL, Dahlstrom WG, Siegler IC, Anderson NB, Williams RB. Hostility patterns and health implications: Correlates of Cook-Medley Hostility scales scores in a national survey. Health Psychology. 1991;10:18–24. doi: 10.1037//0278-6133.10.1.18. [DOI] [PubMed] [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Benyamini Y, Leventhal EA, Leventhal H. Self-assessments of health: What do people know that predicts their mortality? Research on Aging. 1999;21:777–800. [Google Scholar]
- Bogg T, Roberts BW. Conscientiousness and health-related behaviors: A meta-analysis of the leading behavioral contributors to mortality. Psychological Bulletin. 2004;130:887–919. doi: 10.1037/0033-2909.130.6.887. [DOI] [PubMed] [Google Scholar]
- Booth-Kewley S, Vickers RR., Jr Associations between the major domains of personality and health behavior. Journal of Personality. 1994;62:281–298. doi: 10.1111/j.1467-6494.1994.tb00298.x. [DOI] [PubMed] [Google Scholar]
- Caspi A. The child is father of the man: Personality continuities from childhood to adulthood. Journal of Personality and Social Psychology. 2000;78:158–172. doi: 10.1037//0022-3514.78.1.158. [DOI] [PubMed] [Google Scholar]
- Caspi A, Begg D, Dickson N, Langley J, Moffitt TE, McGee R, Silva PA. Identification of personality types at risk for poor health and injury in late adolescence. Criminal Behavior & Mental Health. 1995;5:330–350. [Google Scholar]
- Christensen AJ, Ehlers SL, Wiebe JS, Moran PJ, Raichle K, Ferneyhough K, Lawton WJ. Patient personality and mortality: A 4-year prospective examination of chronic renal insufficiency. Health Psychology. 2002;21:315–320. doi: 10.1037//0278-6133.21.4.315. [DOI] [PubMed] [Google Scholar]
- Clark, L. A., & Watson, D. (1999). Temperament: A new paradigm for trait psychology. In L. Pervin & O. John (Eds.), Handbook of personality research and theory (Vol. 2). New York: The Guilford Press.
- Cohen S, Doyle WJ, Turner R, Alper CM, Skoner D. Sociability and susceptibility to the common cold. Psychological Science. 2003;14:389–395. doi: 10.1111/1467-9280.01452. [DOI] [PubMed] [Google Scholar]
- Costa PT, Jr., McCrae RR. Neuroticism, somatic complaints, and disease: Is the bark worse than the bite? Journal of Personality. 1987;55:299–316. doi: 10.1111/j.1467-6494.1987.tb00438.x. [DOI] [PubMed] [Google Scholar]
- Danner DD, Snowden DA, Friesen WV. Positive emotions in early life and longevity: Findings from the Nun study. Journal of Personality and Social Psychology. 2001;80:804–813. [PubMed] [Google Scholar]
- Digman, J. M. (1990). Personality structure: Emergence of the five-factor model. In L. W. Porter & M. R. Rosenzweig (Eds.), Annual Review of Psychology: Vol. 41 (pp. 417–440) Palo Alto: Annual Reviews.
- Digman JM, Inouye J. Further specification of the five robust factors of personality. Journal of Personality and Social Psychology. 1986;50:116–123. [Google Scholar]
- Friedman HS. Long-term relations of personality and health: Dynamisms, mechanisms, and tropisms. Journal of Personality. 2000;68:1089–1107. doi: 10.1111/1467-6494.00127. [DOI] [PubMed] [Google Scholar]
- Friedman HS, Tucker JS, Tomlinson-Keasy C, Schwartz JE, Wingard DL, Criqui MH. Does childhood personality predict longevity? Journal of Personality and Social Psychology. 1993;65:176–185. doi: 10.1037//0022-3514.65.1.176. [DOI] [PubMed] [Google Scholar]
- Friedman HS, Tucker JS, Schwartz JE, Martin LR, Tomlinson-Keasy C, Wingard DL, Criqui MH. Childhood conscientiousness and longevity: Health behaviors and cause of death. Journal of Personality and Social Psychology. 1995;68:696–703. doi: 10.1037//0022-3514.68.4.696. [DOI] [PubMed] [Google Scholar]
- Gerrard M, Gibbons FX, Benthin AC, Hessling RM. A longitudinal study of the reciprocal nature of risk behaviors and cognitions in adolescents: What you do shapes what you think and vice versa. Health Psychology. 1996;15:344–354. doi: 10.1037//0278-6133.15.5.344. [DOI] [PubMed] [Google Scholar]
- Gilbert, D. (1995). Smoking: Individual differences, psychopathology, and emotion. Washington, DC: Taylor & Francis.
- Goldberg LR. The structure of phenotypic personality traits. American Psychologist. 1993;48:26–34. doi: 10.1037//0003-066x.48.1.26. [DOI] [PubMed] [Google Scholar]
- Goldberg LR. Analysis of Digman’s child-personality data: Derivation of Big-Five factor scores from each of six samples. Journal of Personality. 2001;69:709–743. doi: 10.1111/1467-6494.695161. [DOI] [PubMed] [Google Scholar]
- Goldberg LR, Strycker L. Personality traits and eating habits: The assessment of food preferences in a large community sample. Personality and Individual Differences. 2002;32:49–65. [Google Scholar]
- Goodwin R, Engstrom G. Personality and the perception of health in the general population. Psychological Medicine. 2002;32:325–332. doi: 10.1017/s0033291701005104. [DOI] [PubMed] [Google Scholar]
- Graves PL, Mead LA, Wang NY, Liang KY, Klag MJ. Temperament as a potential predictor of mortality: Evidence from a 41-year prospective study. Journal of Behavioral Medicine. 1994;17:111–126. doi: 10.1007/BF01858100. [DOI] [PubMed] [Google Scholar]
- Hampson SE, Andrews JA, Barckley M, Lichtenstein E, Lee M. Conscientiousness, perceived risk, and risk-reduction behaviors: A preliminary study. Health Psychology. 2000;19:496–500. [PubMed] [Google Scholar]
- Hampson SE, Dubanoski JP, Hamada W, Marsella AJ, Matsukawa J, Suarez E, Goldberg LR. Where are they now? Locating former elementary-school students after nearly 40 years for a longitudinal study of personality and health. Journal of Research in Personality. 2001;35:375–387. [Google Scholar]
- Idler EL, Benyamini Y. Self-rated health and mortality: A review of twenty-seven community studies. Journal of Health and Social Behavior. 1997;38:21–37. [PubMed] [Google Scholar]
- Ingledew DK, Brunning S. Personality, preventive health behavior and comparative optimism about health problems. Journal of Health Psychology. 1999;4:193–208. doi: 10.1177/135910539900400213. [DOI] [PubMed] [Google Scholar]
- Jerram KJ, Coleman PG. The Big Five personality traits and reporting of health problems and health behavior in old age. British Journal of Health Psychology. 1999;4:181–192. [Google Scholar]
- Jessor, R., & Jessor, S. L. (1977). Problem behavior and psychosocial development: A longitudinal study of youth. New York, NY: Academic Press.
- John, O. P., & Srivastava, S. (1999). The Big Five trait taxonomy: History, measurement, and theoretical perspectives. In L. A. Pervin & O. P. John (Eds.), Handbook of personality theory and research (pp. 139–153). New York: Guilford Press.
- Korten AE, Jorm AF, Jiao AF, Letenneur L, Jacomb PA, Henderson AS, Christensen H, Rodgers B. Health, cognitive, and psychological factors as predictors of mortality in an elderly community sample. Journal of Epidemiology and Community Health. 1999;53:83–88. doi: 10.1136/jech.53.2.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markey CN, Markey PM, Tinsley BJ. Personality, puberty, and preadolescent girls’ risky behaviors: Examining the predictive value of the Five-Factor model of personality. Journal of Research in Personality. 2003;37:405–419. [Google Scholar]
- Marshall GN, Wortman CB, Vickers RR, Kusulas JW, Hervig LK. The five-factor model of personality as a framework for personality-health research. Journal of Personality and Social Psychology. 1994;67:278–286. doi: 10.1037//0022-3514.67.2.278. [DOI] [PubMed] [Google Scholar]
- Martin LR, Friedman HS, Tucker JS, Tomlinson-Keasy C, Criqui MH, Schwartz JE. A life course perspective on childhood cheerfulness and its relation to mortality risk. Personality and Social Psychology Bulletin. 2002;28:1155–1165. [Google Scholar]
- Rhodes RE, Courneya KS. Relationships between personality, an extended theory of planned behavior model and exercise behavior. British Journal of Health Psychology. 2003;8:18–36. doi: 10.1348/135910703762879183. [DOI] [PubMed] [Google Scholar]
- Shedler J, Block J. Adolescent drug use and psychological health: A longitudinal perspective. American Psychologist. 1990;45:612–629. doi: 10.1037//0003-066x.45.5.612. [DOI] [PubMed] [Google Scholar]
- Shiner RL, Masten AS, Roberts JM. Childhood personality foreshadows adult personality and life outcomes two decades later. Journal of Personality. 2003;71:1145–1170. doi: 10.1111/1467-6494.7106010. [DOI] [PubMed] [Google Scholar]
- Smith TW, Spiro A. Personality, health, and aging: Prolegomenon for the next generation. Journal of Research in Personality. 2002;36:363–394. [Google Scholar]
- Smith TW, Williams PG. Personality and health: Advantages and limitations of the five factor model. Journal of Personality. 1992;60:395–423. doi: 10.1111/j.1467-6494.1992.tb00978.x. [DOI] [PubMed] [Google Scholar]
- Sobel, M. E. (1982). Asymptotic confidence intervals for indirect effects in structural equation models. In S. Leinhart (Ed.), Sociological methodology 1982 (pp. 290–312). San Francisco: Jossey-Bass.
- Tarter RE, Vanyukov M, Giancola P, Dawes M, Blackson T, Mezzich A, Clark D. Etiology of early age onset substance use disorder: A maturational perspective. Development and Psychopathology. 1999;11:657–683. doi: 10.1017/s0954579499002266. [DOI] [PubMed] [Google Scholar]
- Terman, L. M., & Oden, M. H. (1947). Genetic studies of genius: The gifted child grows up (Vol. 4). Stanford, CA: Stanford University Press.
- Tucker JS, Friedman HS, Tomlinson-Keasey C, Schwartz JE, Wingard DL, Criqui MH, Martin LR. Childhood psychosocial predictors of adulthood smoking, alcohol consumption, and physical activity. Journal of Applied Social Psychology. 1995;25:1885–1899. [Google Scholar]
- Ware JJ, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection Medical Care. 1992;30:473–483. [PubMed] [Google Scholar]
- Whalley LJ, Deary IJ. The longitudinal cohort study of childhood IQ and survival up to age 76. British Medical Journal. 2001;322:819–824. doi: 10.1136/bmj.322.7290.819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wills TA, DuHamel K, Vaccaro D. Activity and mood temperament as predictors of adolescent substance use: Test of a self-regulation mediational model. Journal of Personality and Social Psychology. 1995;68:901–916. doi: 10.1037//0022-3514.68.5.901. [DOI] [PubMed] [Google Scholar]
- Zuckerman, M. (1991). Psychobiology of personality York, NY: Cambridge University Press.