

Venous ulceration
Venous leg ulceration is due to sustained venous hypertension, which results from chronic venous insufficiency. In the normal venous system, pressure decreases with exercise as a result of the action of the calf muscle pump. When the muscles relax, the valves in the perforating veins connecting the superficial to the deep venous circulation prevent reflux and the pressure remains low. The venous pressure remains high, however, in a system where the valves are incompetent.
Table 1.
Risk factors for venous ulceration
| Direct risk factors |
| • Varicose veins |
| • Deep vein thrombosis |
| • Chronic venous insufficiency |
| • Poor calf muscle function |
| • Arterio-venous fistulae |
| • Obesity |
| • History of leg fracture |
| Indirect risk factors |
| • All risk factors leading to deep vein thrombosis including protein-C, protein-S, and anti-thrombin III deficiency |
| • Family history of varicose veins |
| • A history of minor trauma prior to the development of ulceration may also be identified |
Up to 10% of the population in Europe and North America has valvular incompetence, with 0.2% developing venous ulceration. Forty to fifty per cent of venous ulcers are due to superficial venous insufficiency and/or perforating vein incompetence alone with a normal deep venous system.
There are many risk factors for venous ulceration. Recurrent venous ulceration occurs in up to 70% of those at risk. Many venous ulcers are painful, so appropriate pain relief and advice should be given.
Examination
Ninety five per cent of venous ulceration is in the gaiter area of the leg, characteristically around the malleoli. Ulceration may be discrete or circumferential. The ulcer bed is often covered with a fibrinous layer mixed with granulation tissue, surrounded by an irregular, gently sloping edge. Ulcers occurring above the mid-calf or on the foot are likely to have other origins.
Figure 1.



From left to right: Haemosiderin associated with a venous leg ulcer; lipodermatosclerosis; venous leg ulcer in area of atrophie blanche; wenous leg ulcer with severe “champagne bottle” deformity of the leg
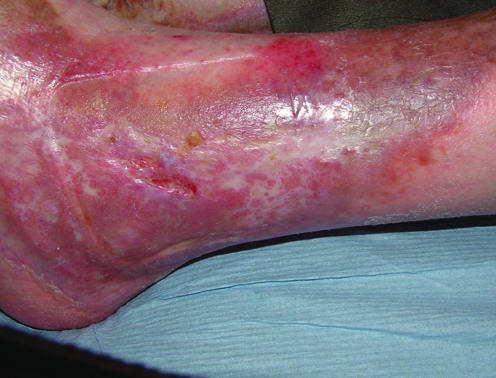
Pitting oedema is often present and may predate the ulcer. It is often worse towards the end of the day. Extravasation of erythrocytes into the skin occurs, resulting in the deposition of haemosiderin within macrophages, which stimulates melanin production, pigmenting the skin brown. In long term venous insufficiency, lipodermatosclerosis occurs. This is characterised by the dermis and subcutaneous tissue becoming indurated and fibrosed with the lack of pitting oedema; the skin also becomes atrophic, loses sweat glands and hair follicles, and becomes variably pigmented (ranging from hypopigmented to hyperpigmented). Severe lipodermatosclerosis may lead to atrophie blanche—white fibrotic areas with low blood flow. Lipodermatosclerosis often precedes venous ulceration. As a result of lipodermatosclerosis, a rigid woody hardness often develops, which at its worst may result in the leg resembling an “inverted champagne bottle.” Venous eczema (erythema, scaling, weeping, and itching) is also common and is distinct from cellulitis.
Figure 2.


Typical venous leg ulcer over the medial malleolus (left) and venous leg ulcer over malleolus with a fibrinous base (right)
Table 2.
Features of venous eczema and cellulitis
| Venous eczema | Cellulitis |
|---|---|
| Red, warm, painful, and tender to touch | Red, warm, painful, and tender to touch |
| Usually chronic | Insidious (usually develops over 24-72 hours) |
| Diffuse and poorly demarcated | Usually well demarcated |
| Increase in exudate | No increase in exudate |
| Itchy | Not itchy |
| Scaly | Not scaly |
| Treated with topical steroids | Treated with systemic antibiotics |
This is the second in a series of 12 articles
Management
Compression is the mainstay of venous ulcer management (see also 11th article in this series). Graded compression, with greatest pressure (about 40 mm Hg) at the ankle, tapering off to lower pressure (about 18 mm Hg) below the knee, increases the limb hydrostatic pressure and concomitantly reduces the superficial venous pressure. Various compression bandage systems are used. These include the single and multilayer elastic banadage system, short stretch bandage, and elasticated tubular bandages (for example, Tubigrip). Compression with pneumatic devices (for example, Flowtron) has been used to promote healing of venous ulcers in patients with oedematous legs.
Patients should be warned to remove the compression if they notice any side effects (such as numbness, tingling, pain, and dusky toes) and seek advice.
Table 3.
Choice of dressing
| • Dressing choice will reflect the nature of the ulcer (see ninth article in this series) |
| • The leg should always be raised when a patient is seated |
| • Patients should be encouraged, however, to remain active provided they are wearing some form of compression system |
Sharp debridement of non-viable tissue may expedite healing of venous ulcers and can be done in the primary care setting. Surgery is normally indicated to correct superficial venous disease in an attempt to prevent ulcers from recurring. Shave therapy (excision of the whole ulcer) followed by skin grafting, or skin grafting alone, may be useful in patients where other treatments have failed.
Figure 3.


Unhealthy venous leg ulcer before debridement (left) and sharp debridement of venous leg ulcer (right)
Venous leg ulcers often become infected (see 10th article in this series for how to detect signs of infection). The most common organisms include Staphylococcus aureus, Pseudomonas aeruginosa, and β-haemolytic streptococci. Initially, these should be treated empirically (with broad spectrum penicillin or macrolide or quinolone antibiotics) until definitive culture and sensitivities are available. Infection should be treated with a two week course of antibiotics. Topical antibiotics should be avoided owing to the risk of increasing bacterial resistance and contact dermatitis. Associated venous eczema should be treated with topical steroids and emollients. The eczema may be secondarily infected and require systemic antibiotic therapy.
Table 4.
Compression stockings
| Class | Pressure at ankle (mm Hg) | Indication |
|---|---|---|
| I | 14-17 | Mild varicose veins |
| II | 18-24 | Prevention of recurrence of venous ulcers on narrow legs and in slim patients and for mild oedema |
| III | 25-35 | Chronic venous insufficiency and oedema, and large heavy legs |
Once the venous ulcer has healed, it is essential that patients follow simple advice aimed at preventing the recurrence of the ulcer: this includes wearing compression stockings, skin care, leg elevation, calf exercises, and adopting a suitable diet. The reported annual recurrence rate of venous ulcers (20%) is strongly influenced by patient adherence. Local “leg clubs” (www.legclub.org) may help to reduce this rate.
Figure 4.

Compression stocking
Arterial ulceration
Arterial ulceration is due to a reduced arterial blood supply to the lower limb. The most common cause is atherosclerotic disease of the medium and large sized arteries. Other causes include diabetes, thromboangiitis, vasculitis, pyoderma gangrenosum, thalassaemia, and sickle cell disease, some of which may predispose to the formation of atheroma. Further damage to the arterial system occurs with concurrent hypertension through damage of the intimal layer of the artery. The reduction in arterial blood supply results in tissue hypoxia and tissue damage. Thrombotic and atheroembolic episodes may contribute to tissue damage and ulcer formation.
Figure 5.

Guidelines for management of different categories of venous eczema. Arrows indicate direction of possible change in condition of eczema
Unna's boot, a wet zinc oxide bandage applied from toes to knee and covered with elastic compression bandage, is commonly used in the United States. The surrounding skin, however, can develop contact dermatitis, and this type of bandaging may fail to control high levels of exudate from the ulcer
Arterial ulceration often occurs after seemingly trivial trauma or as the result of localised pressure
Peripheral vascular disease is most common in men older than 45 and women older than 55, and patients may have a family history of premature atherosclerotic disease. Modifiable risk factors for peripheral vascular disease include smoking, hyperlipidaemia, hypertension, diabetes, and obesity, with associated decreased activity. Patients may also have a history of generalised vascular problems, such as myocardial infarction, angina, stroke, and intermittent claudication.
Table 5.
Pain with arterial ulceration
| • Pain may be present at rest and may be alleviated by hanging the foot over the side of the bed or sleeping in a chair |
| • Pain usually begins distal to the obstruction, moving proximally as ischaemia progresses |
| • The ulcer itself is often painful |
Examination
Arterial ulceration typically occurs over the toes, heels, and bony prominences of the foot. The ulcer appears “punched out,” with well demarcated edges and a pale, non-granulating, often necrotic base. The surrounding skin may exhibit dusky erythema and may be cool to touch, hairless, thin, and brittle, with a shiny texture. The toenails thicken and become opaque and may be lost. Gangrene of the extremities may also occur. Examination of the arterial system may show a decreased or absent pulse in the dorsalis pedis and posterior tibial arteries. There may be bruits in the proximal leg arteries, indicating the presence of atherosclerosis.
Figure 6.



Top left: Dry gangrene of great toe in a patient with peripheral vascular disease with line of demarcation covered with slough. Top right: Wet gangrene of forefoot and toes in a patient with arterial disease, with soft tissue swelling due to infection. Left: Arterial ulcer over lower leg, with associated skin changes typical of arterial disease
Table 6.
Features of venous and arterial ulcers
| Venous | Arterial | |
|---|---|---|
| History | History of varicose veins, deep vein thrombosis, venous insufficiency or venous incompetence | History suggestive of peripheral arterial disease, intermittent claudication, and/or rest pain |
| Classic site | Over the medial gaiter region of the leg | Usually over the toes, foot, and ankle |
| Edges | Sloping | Punched out |
| Wound bed | Often covered with slough | Often covered with varying degrees of slough and necrotic tissue |
| Exudate level | Usually high | Usually low |
| Pain | Pain not severe unless associated with excessive oedema or infection | Pain, even without infection |
| Oedema | Usually associated with limb oedema | Oedema not common |
| Associated features | Venous eczema, lipodermatosclerosis, atrophie blanche, haemosiderosis | Trophic changes; gangrene may be present |
| Treatment | Compression is mainstay | Appropriate surgery for arterial insufficiency; drugs of limited value |
Patients with arterial ulcers have a reduced capillary refill time. With normal capillary refill, after compression of the great toe or dorsum of the foot for a few seconds, the skin colour should return to normal in less than two to three seconds. Delay in return of the normal colour is indicative of vascular compromise. A delay of more than 10 to 15 seconds in return of colour after raising an ischaemic leg to 45 degrees for one minute (Buerger's test) indicates vascular compromise.
Table 7.
Interpreting ankle brachial pressure index
| Index | Signs and symptoms | Severity of disease | Action |
|---|---|---|---|
| ≥0.7-1 | Mild intermittent claudication, or no symptoms | Mild arterial disease | Reduce risk factors and change lifestyle: stop smoking, maintain weight, exercise regularly, consider antiplatelet agent |
| 0.7-0.5 | Varying degrees of intermittent claudication | Mild to moderate arterial disease | As for index ≥0.7-1, plus referral to outpatient vascular specialist and possible arterial imaging (duplex scan and/or angiogram) |
| 0.5-0.3 | Severe intermittent claudication and rest pain | Severe arterial disease | As for index ≥0.7-1, plus urgent referral to vascular specialist and possible arterial imaging (duplex scan and/or angiogram) |
| ≤ 0.3 or ankle systolic pressure <50 mm Hg | Critical ischaemia (rest pain >2 weeks) with or without tissue loss (ulcer, gangrene) | Severe arterial disease; risk of losing limb | Urgent referral to vascular emergency on-call team and possible surgical or radiological intervention |
An index of 1 to 1.1 is considered to be normal. The data in the table should be used as an adjunct to the clinical findings. Erroneous readings may be the result of incompressible arteries secondary to presence of calcification or presence of tissue oedema. Patients may present with an arterial ulcer even with a normal index. Patients may present with an acutely ischaemic limb either due to an embolus or a thrombus (“acute on chronic” ischaemia) and should be referred as an emergency to a vascular specialist or emergency department for urgent intervention to prevent imminent limb loss.
The ankle brachial pressure index is helpful in identifying peripheral vascular disease in the absence of non-compressible vessels resulting from vessel calcification (for example, diabetes) or tissue oedema. A duplex ultrasound scan will give further information—on arterial occlusion, stenosis, and areas of diffuse and continuous atheromatous disease. Arteriography is the ideal investigation in preoperative planning, allowing direct assessment of the vascular anatomy of the lower limb.
Management
Increasing the peripheral blood flow by, for example, reconstructive surgery (for diffuse disease) or angioplasty (for localised stenosis) is the intervention most likely to affect the healing process in arterial ulceration. Operative indications for chronic ischaemia include non-healing ulceration, gangrene, rest pain, and progression of disabling claudication.
The patient should stop smoking, and control of diabetes, hypertension, and hyperlipidaemia should be optimised. Patients may find benefits from sleeping in a bed raised at the head end. Patients should follow simple advice on foot and leg care. Walking is beneficial.
Table 8.
Guidelines for patients on protecting lower limbs and feet
| • Examine the feet daily for broken skin, blisters, swelling, or redness |
| • Report worsening symptoms—for example, decreasing walking distance, pain at rest, pain at night, changes in skin colour |
| • Keep the skin moist with, for example, 50/50 white soft paraffin and liquid paraffin mix |
| • Never walk barefoot |
| • Ensure shoes are well fitting and free of friction and pressure points; check them for foreign objects (such as stones) before wearing; and avoid open toed sandals and pointed shoes |
| • Give up smoking |
| • Take regular exercise within limits of pain and tolerance |
Infection can cause rapid deterioration in an arterial ulcer, and treatment with systemic antibiotics (along the lines for venous ulceration outlined above) should be started. Patients with rest pain or worsening claudication, or both, and a non-healing ulcer should be referred to a vascular surgeon; opioid analgesia may be necessary during the wait for surgery. It is not appropriate to debride arterial ulcers as this may promote further ischaemia and lead to the formation of a larger ulcer.
Figure 7.

Ulcer over medial malleolus of mixed arterial and venous aetiology, with lipodermatosclerosis and breakdown of scar over saphenous vein harvesting site (for cardiac bypass grafting)
Choice of wound dressings will be dictated by the nature of the wound. Vasoconstrictive drugs such as non-selective β blockers should be avoided. (See 11th article in this series for more information on drug treatment.)
Ulceration of mixed aetiology is not uncommon: patients may have a combination of venous and arterial diseases, resulting in ulcers of mixed aetiologies, which will limit the degree of compression (if any) that can be used.
The table on interpreting the ankle brachial pressure index is adapted from Beard JD, Gaines PA, eds. Vascular and endovascular surgery. 3rd ed. London: WB Saunders, 2005.
The ABC of wound healing is edited by Joseph E Grey (joseph.grey@cardiffandvale.wales.nhs.uk), consultant physician, University Hospital of Wales, Cardiff and Vale NHS Trust, Cardiff, and honorary consultant in wound healing at the Wound Healing Research Unit, Cardiff University, and by Keith G Harding, director of the Wound Healing Research Unit, Cardiff University, and professor of rehabilitation medicine (wound healing) at Cardiff and Vale NHS Trust. The series will be published as a book in summer 2006.
Competing interests: For series editors' competing interests, see the first article in this series.
References
- • Simon DA, Dix FP, McCollum CN. Management of venous leg ulcers. BMJ 2004;328: 1358-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- • Barwell JR, Davies CE, Deacon J, Harvey K, Minor J, Sassano A, et al. Comparison of surgery and compression with compression alone in chronic venous ulceration (ESCHAR study): randomised controlled trial. Lancet 2004;363: 1854-9. [DOI] [PubMed] [Google Scholar]
- • Cullum N, Nelson EA, Fletcher AW, Sheldon TA. Compression for venous leg ulcers. Cochrane Database Syst Rev 2001;(2): CD000265. [DOI] [PubMed]
- • Williams DT, Enoch S, Miller DR, Harris K, Price PE, Harding KG. The effect of sharp debridement using curette on recalcitrant non-healing venous leg ulcers: a concurrently controlled prospective cohort study. Wound Rep Regen 2005;13: 131-7. [DOI] [PubMed] [Google Scholar]
- • Morris PJ, Malt RA. Oxford textbook of surgery. 2nd ed. Oxford: Oxford University Press, 2001.
- • Burnand KG, Young AE, Lucas JD, Rowlands B, Scholefield J. The new Aird's companion in surgical studies. 2nd ed. Edinburgh: Elsevier Churchill Livingstone, 2005.
- • Nelson EA, Bell-Syer SE, Cullum NA. Compression for preventing recurrence of venous ulcers. Cochrane Database Syst Rev 2000;(4): CD002303. [DOI] [PubMed]
- • Gohel MS, Barwell JR, Earnshaw JJ, Heather BP, Mitchell DC, Whyman MR, et al. Randomized clinical trial of compression plus surgery versus compression alone in chronic venous ulceration (ESCHAR study)—haemodynamic and anatomical changes. Br J Surg 2005;92: 291-7. [DOI] [PubMed] [Google Scholar]