

Abstract
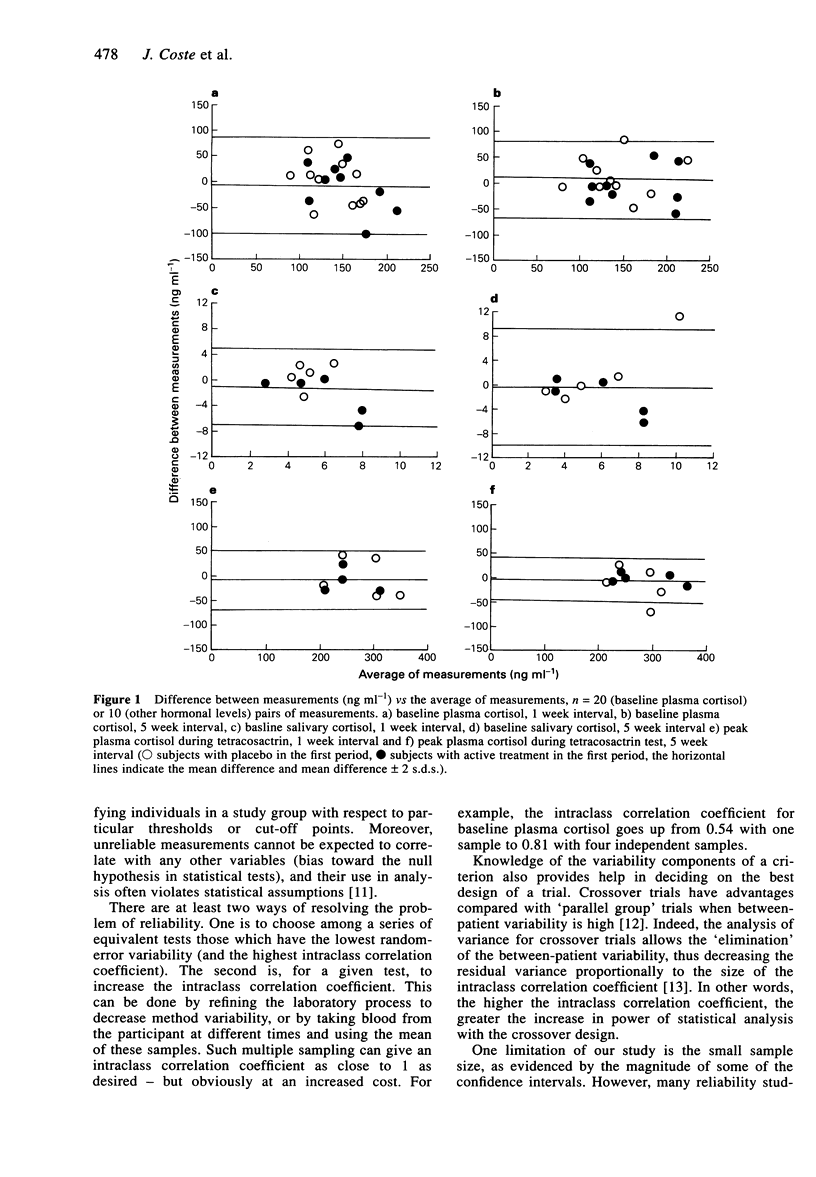
Few data are available on the reliability of measurements of adrenocortical and corticotroph hormones for use in clinical pharmacology. Two placebo controlled cross-over trials in 20 normal healthy male subjects offered the opportunity to perform three repeat samplings of adrenocortical and corticotroph hormones at 1 to 5 week intervals during the placebo periods. Measurements of baseline levels of plasma, salivary and urinary cortisol, plasma adrenocorticotroph hormone (ACTH), lipotrophic hormone (LPH), beta-endorphin, post tetracosactrin levels of plasma and salivary cortisol, post corticotrophin releasing hormone (CRH)-lysine vasopressine (LVP) levels of plasma cortisol, ACTH and LPH; and post metyrapone levels of plasma cortisol and 11-deoxycortisol (compound S), ACTH, LPH, beta-endorphin were performed in the same laboratory. The reliability of the measurements was estimated by computing the intraclass correlation coefficient (R) and by using Altman-Bland graphical method. The Rs of baseline parameters varied from 0.18 (for 08.00 h salivary cortisol) to 0.55 (for 08.00 h plasma cortisol and nocturnal urinary cortisol). In contrast, parameters obtained after direct stimulation or inhibition of the producing targets were much more reliable: Rs were above 0.80 for post tetracosactrin levels of plasma and salivary cortisol, post CRH-LVP levels of plasma ACTH and LPH. The Rs were below 0.50 for post metyrapone levels of plasma 11-deoxycortisol, ACTH, LPH and beta-endorphin. The interval between sampling did not affect R estimates. These data show that peak levels of plasma cortisol and ACTH after direct stimulation are highly reliable whereas baseline and main post-metyrapone levels are not.(ABSTRACT TRUNCATED AT 250 WORDS)
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Kaye T. B., Crapo L. The Cushing syndrome: an update on diagnostic tests. Ann Intern Med. 1990 Mar 15;112(6):434–444. doi: 10.7326/0003-4819-76-3-112-6-434. [DOI] [PubMed] [Google Scholar]
- Kuhn J. M., Bertagna X., Seurin D., Gourmelen M., Girard F. Plasma lipotropin increase in man after growth hormone administration. Comparison between extractive and biosynthetic hormones. J Clin Endocrinol Metab. 1983 Jun;56(6):1338–1340. doi: 10.1210/jcem-56-6-1338. [DOI] [PubMed] [Google Scholar]
- Laudat M. H., Billaud L., Thomopoulos P., Vera O., Yllia A., Luton J. P. Evening urinary free corticoids: a screening test in Cushing's syndrome and incidentally discovered adrenal tumours. Acta Endocrinol (Copenh) 1988 Nov;119(3):459–464. doi: 10.1530/acta.0.1190459. [DOI] [PubMed] [Google Scholar]
- Streeten D. H., Anderson G. H., Jr, Dalakos T. G., Seeley D., Mallov J. S., Eusebio R., Sunderlin F. S., Badawy S. Z., King R. B. Normal and abnormal function of the hypothalamic-pituitary-adrenocortical system in man. Endocr Rev. 1984 Summer;5(3):371–394. doi: 10.1210/edrv-5-3-371. [DOI] [PubMed] [Google Scholar]